Case Report
A 55-year-old female patient reported to Department of Prosthodontics, with the chief complaint of difficulty in chewing food. Weight of the denture was patient’s prime concern, as she was not able to chew food efficiently due to heaviness in her lower complete denture, and she reported of frequent dislodgement of the prosthesis during functional movements of the lower jaw. On probing past dental history, patient said she had been edentulous for past six years and had used many sets of complete denture prostheses; none satisfying her to optimum levels of functional usefulness. Medical history revealed no underlying systemic disorder. On intraoral examination, it was found that her mandibular residual ridge was severely resorbed (ACP type IV) [1] with increased inter-ridge distance.
The various treatment modalities were mutually discussed with the patient, taking into consideration the presenting clinical findings. She insisted for a more economically viable rehabilitative measure. Giving due respect to the patient’s expectations, it was decided to fabricate a new set of complete dentures. Relining of her previously worn prosthesis was not contemplated, due to altered vertical dimensions and grossly attrided teeth in them, while the fixed modality of treatment, i.e., implants supported overdentures were ruled out of contention due to unfavourable osseous morphology. As the patient expressed dissatisfaction with the heavy prostheses in the past, a “hollow” light weighing mandibular complete denture opposing conventional maxillary complete denture was planned for this patient. The previous denture was compromised in vertical height, appeared unaesthetic, had attrited teeth and was heavy. The new hollow denture was ameliorated to be 4% lighter in weight.
Procedure
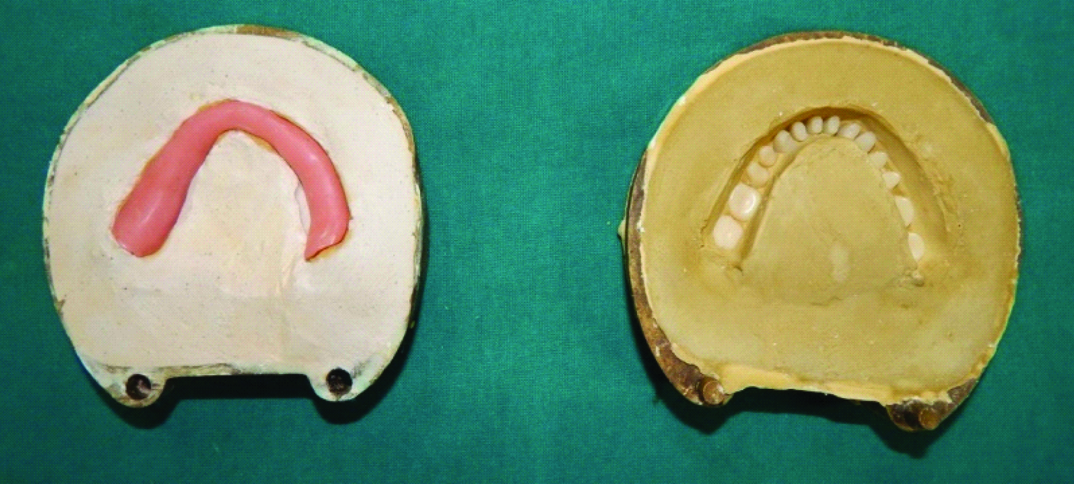
The routine steps of denture making were carried out using standard techniques for both maxillary and mandibular arches, after an informed consent undertaking from the patient. Preliminary impressions were recorded using impression compound (DPI Pinnacle, Apexion dental products, Calicut, Kerala, India) and poured in dental plaster (Type 2 model Plaster, Kalabhai Karson Pvt. Ltd. Vikhroli, Mumbai, India). Special trays were fabricated on the obtained primary casts using auto polymerising resins (Ashwin, Super Dental Products, Delhi, India), followed by verifying their correct extensions, and sequentially border moulded using low fusing impression compound (DPI Pinnacle tracing sticks, Mumbai, India). Wash impressions were made using elastomeric impression material of light body consistency (Speedex Coltene, Whale dent Inc. Products, America), which were beaded, boxed and subsequently poured in Dental Stone (Goldstone Stone Plaster Class 3). A processed record base of heat cure acrylic resin (Acralyn H Pink) was made on the mandibular final cast [Table/Fig-1]. Maxillary mandibular relation was recorded and was transferred to the semi adjustable articulator. Artificial teeth (Acry Pan, Ruthinium, India) were arranged and clinical try in was approved. After having completed the wax up, the “double flask” technique was employed for processing.
Principally the Fattore LD et al., double flask technique [2] was employed for imparting hollow property to the dentures; additionally specific orientation slots were sensibly created in the split denture segments that guided to ensure exact approximation between the tooth bearing portion and denture base. Two identical flasks with interchangeable lids were used. An ejector type flask was used in this case. After flasking and dewaxing, mould space was created in one part (cope) and cast with permanent denture base was in other part (drag) [Table/Fig-1]. Next, thicker portions were identified in the lower permanent denture base and retentive locks were created, so as to aid the accurate seating of two parts of split denture later on and simultaneously maintain actual vertical dimension. It was ensured that a butt joint [Table/Fig-2] be created between the walls of the lock, without any undercut. There were seven such locks prepared; four and three on buccal and lingual sides respectively. The dimensions of three buccal locks were kept to be 2x1x1 cm, while the remaining buccal and three lingual locks were sized 1x1x1 cm.
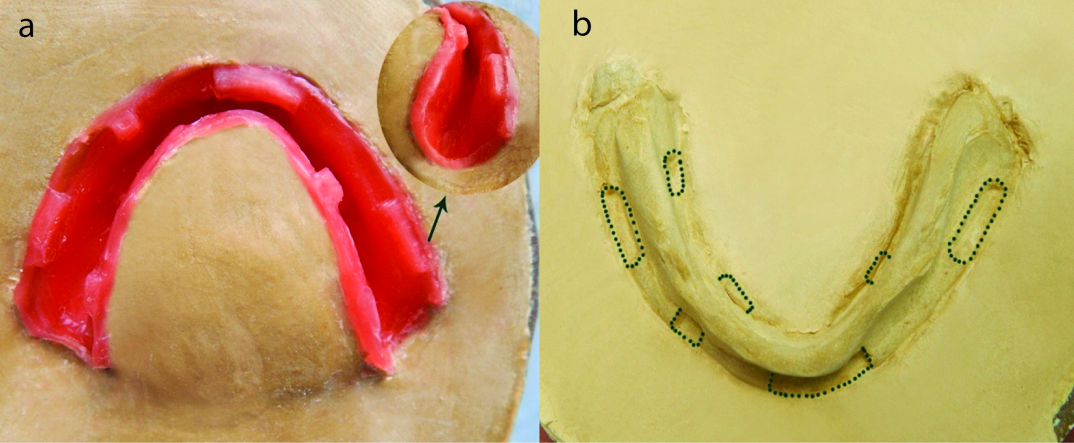
Thereafter, a wax shim of thickness 2 mm was adapted in the mould space (cope), that was eventually going to serve as the teeth bearing part of the denture and duplication of slots of permanent denture base onto the wax shim was achieved by repeated trial closure of permanent denture base. The slots were refined to desirable contours by carving out the excess wax each time after each trial closure [Table/Fig-3a]. A uniform layer of separating medium was applied on the investing stone surrounding the mould space.
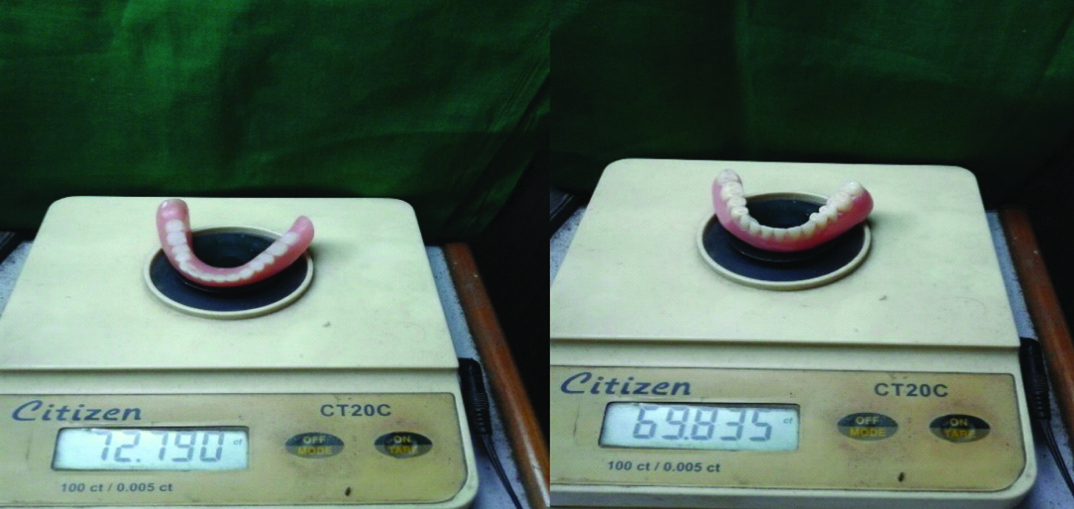
Then drag part of the identical flask was taken, dental stone was poured into the mould containing wax shim (cope) through the drag by removing knock out plate, with generous tapping, and stone was allowed to set. Another dewaxing cycle was carried out to remove wax shim after the setting of stone and a modified mould cavity was obtained, which had locks transferred on the stone master cast [Table/Fig-3b]. Final packing was done using heat cure acrylic resin (Acralyn H Pink) and split denture segment containing teeth portion [Table/Fig-4] was obtained upon completion of curing cycle. Excess flash was trimmed, finished and polished and the two portions were seated to verify accurate fitting through the retentive locks, serving as guides. Both the portions were ultimately apposed [Table/Fig-5] using auto polymerizing resin, and completeness of the seal (intactness of the hollow property) was put to test by placing it in a beaker filled with water [Table/Fig-6]. The reduction in weight achieved by hollowing of denture was calibrated and demonstrated numerically on a digital weighing machine [Table/Fig-7]. Patient’s preoperative [Table/Fig-8a] and post denture insertion immediate intraoral views [Table/Fig-8b] were captured analysed and verified through utmost scrutiny for form, function and comfort. Follow up visits were scheduled at regular intervals of 24 hours, one week, three weeks, two months and six months, without any notable complaint from patient’s side. Rather patient expressed increased comfort with the timely follow up visits.
Heat cured mandibular denture base and mold cavity containing teeth (“Drag” and “Cope” parts respectively).
Orientation slots with butt joint created in denture base; four on buccal side and three on lingual side.

a) Duplication of slots from permanent denture base onto the wax shim by repeated trial closures; b) Modified mould cavity-locks transferred on the stone master cast.
Parts of split denture base; Teeth bearing portion and denture base.
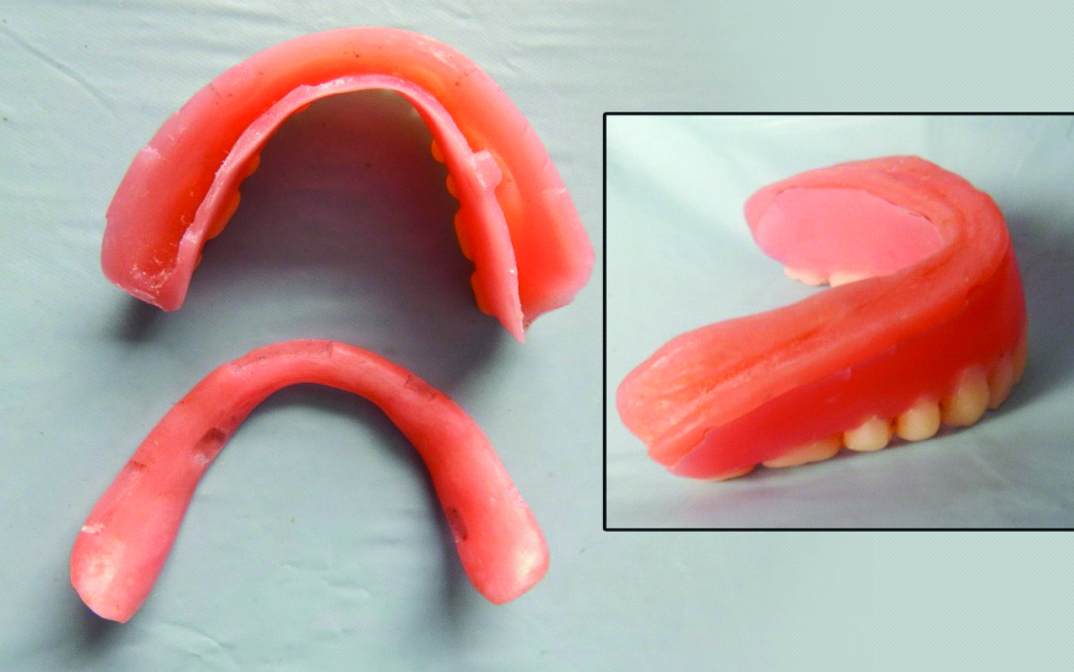
Finished and polished hollow mandibular denture (intaglio surface).

Intactness of the hollowness achieved being verified with the floating test.

Direct comparison of the weight reduction achieved with the newly fabricated denture against the old worn out denture on digitized weighing machine.
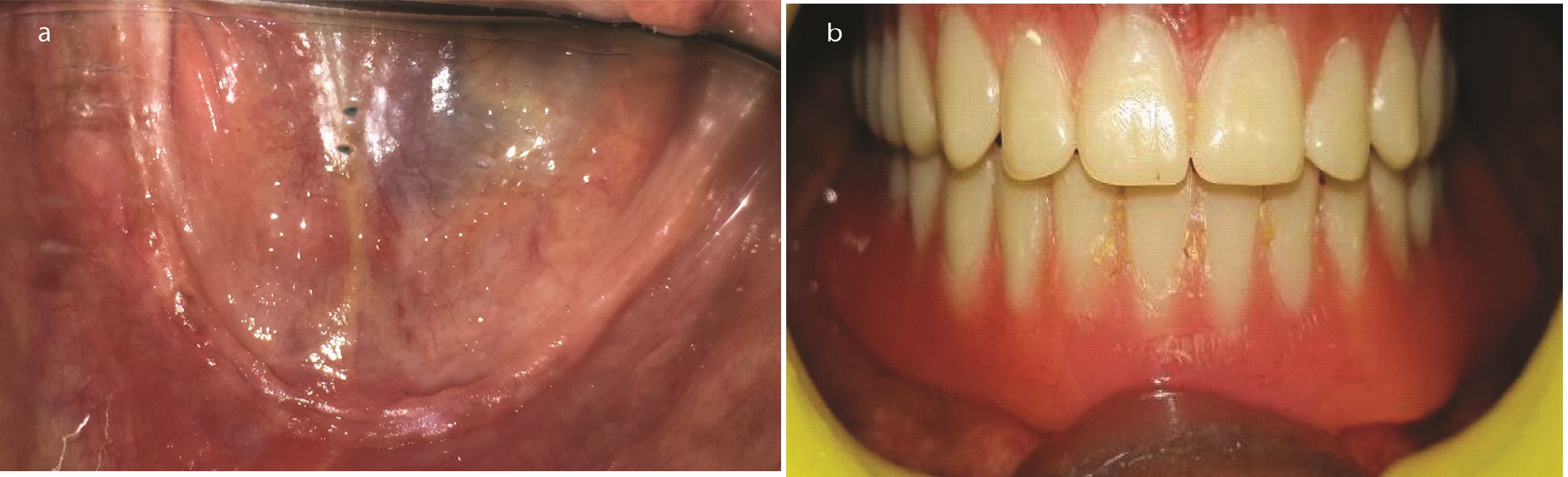
a) Patient’s preoperative intra oral view showing atrophic mandibular ridge; b) Post denture insertion rehabilitated intraoral view with mandibular hollow denture seated into place.
Discussion
Severe atrophy in the residual alveolar ridges has long been a confounding clinical challenge for successful prosthodontic rehabilitation. Pain, mucosal intolerance to loading, difficulties with eating and speech, loss of soft tissue support, altered facial appearance etc., are often encountered as their usual presenting complaints. Furthermore a severely resorbed mandibular ridge results in a more constricted residual ridge, decreased supporting tissue bed and a resultant large restorative inter-ridge space. A denture often replaces more bone than teeth to restore the proper dimensions of the face [3]. A 25-year longitudinal study of lateral cephalograms of edentulous patients conducted by Tallgren A, demonstrated a fourfold greater bone loss in the mandible [4].
Weight of the denture continues to remain an “ambivalent” criterion of consideration by notable authors, with convincing literary justifications existing for both, heavy and light weighing dentures. Grunewald AH in his study concluded that the gold denture bases employed, by virtue of its heaviness, served dual functions of an efficiently adapted denture base to the underlying tissue bed (stability), along with a sound retentive quality [5]. This ideology was supported by Wormley JH et al., who further went on with describing the advantages of weighted dentures, apart from offering the advantages of a cast metal base, namely the additional ease of adjustment and relining [6]. ‘Weighted’ mandibular denture was thus an advocated treatment modality for the management of severely resorbed ridges, as it contributes to both the retention and stability of mandibular prosthesis, aided by gravitational forces [7].
However, around that time, some additional studies also cropped up which promoted the thought that adding up a few extra ounces was not mandatorily essential for supplementing the stability of the dentures, rather by improvising upon the fit of the denture bases, resoundingly well stability could be equally met with [6,8]. One such study conducted by Ohkubo C and Hosoi T [9] stated that the mandibular denture retention or stability is not at all augmented by weight. Some criticism also arose that extra weight instead of benefitting the prosthesis, may cause accelerated resorption of the residual ridges [10,11] owing to its continuous pressure being exerted upon the residual ridge, even at rest [12,13,14].
These studies served as the guiding force to develop techniques that maintain volume of denture base without increasing the weight factor, by “hollowing out” the denture base. Given the extensive volume of the denture base material in prosthesis provided to patients with severe residual ridge resorption, reduction in prosthesis weight may be achieved by making the denture bases hollow.
To substantiate these facts, the following mathematical observational findings are put forth in this case report:
The weight of old worn out denture was found out to be 72.790 carat or 14.558 grams.
(1 carat = 200 mg = 0.2 grams)
Weight of newly fabricated hollow denture was measured to be 69.835 carat = 13.967 grams.
Percentage decrease in weight
Hence, a remarkable 4 % decrease in weight is achieved by virtue of the hollow denture, in comparison with the old worn out denture.
Fattore LD had modified and applied the double flask technique described by Chalian V and Barnett MD for the fabrication of the hollow bulb portion [14] of obturator prosthesis. Adhering to the same principles, this technique can be applied for the fabrication of a lightweight mandibular denture for cases, wherein there is excessive ridge resorption with adequate inter occlusal distance. A modified technique to manufacture hollow denture has been narrated in this case report, with the principal advantage of maintaining Vertical Dimension at Occlusion (VDO) by accurate seating of two parts of split denture, by means of retentive/orientation locks. Unwanted rotational forces and occlusal discrepancies are abated, and an optimal hollow space while fabrication can be gauged without compromising the overall strength of the mandibular denture.
However, this technique also accompanies some inherent flaws. Additional laboratory steps have to be incorporated making it technique sensitive, and as both segments were joined using autopolymerising resin, micro leakage and discoloration may be a concern.
In previously documented techniques, difficulties related to gauging of resin thickness, accurate maintenance of the hollow space and simultaneously maintaining the vertical dimension to maximal levels of precision were frequently encountered. Some techniques [15-18] even used silicone putty as a spacer for hollowing the prosthesis; however, its retrieval was a difficult prospect from the hollow cavity later on, due to its stiffness after complete polymerization of the prosthesis.
Conclusion
Hollow mandibular complete denture considerably reduces the weight of the prosthesis, which in turn prevents transmission of detrimental forces to the atrophic residual alveolar ridge that would otherwise be transmitted from a conventional heavy prosthesis to the underlying tissue bed, exerting its derogatory repercussions in the longer run. Residual ridge resorption, although an indispensable phenomenon, yet with innovatively entrusted and clinically efficacious prostheses such as the hollow denture described above, they can unarguably prove noteworthy in combating the challenges faced with pleasing outcomes.
[1]. SX Pan, JS Feine, HL Feng, Evaluation of clinical application of ACP classification for edentulous patientsBeijing Da Xue Xue Bao 2009 41:86-89. [Google Scholar]
[2]. LD Fattore, L Fine, DC Edmonds, The hollow denture: An alternative treatment for atrophic maxillaeJ Prosthet Dent 1988 59:514-16. [Google Scholar]
[3]. E Misch Carl, Contemporary implant dentistry: Mosby Elsevier 2008 :10-11. [Google Scholar]
[4]. A Tallgren, The reduction in face height of edentulous and partially edentulous subjects during long-term denturewear: A longitudinal roentgenographic cephalometric studyActa Odontol Scand 1966 24:195-239. [Google Scholar]
[5]. AH Grunewald, Gold base lower denturesJ Prosthet Dent 1964 14:432-41. [Google Scholar]
[6]. JH Wormley, DA Brunton, Weighted mandibular denturesJ Prosthet Dent 1974 34:101-02. [Google Scholar]
[7]. AJ Hurtado, Internally weighted mandibular denturesJ Prosthet Dent 1988 60:122-23. [Google Scholar]
[8]. VE Beresin, FJ Sciesser, The neutral zone in Complete and Partial dentures 1978 2nd EditionSt LouisCV Mosby:15-30. [Google Scholar]
[9]. C Ohkubo, T Hosoi, Effect of weight change of mandibular complete dentures on chewing and stability: A pilot studyJ Prosthet Dent 1999 82:636-42. [Google Scholar]
[10]. EF Brennon, Adding weight may promote retention of lower dentureDent Surv 1973 49:30 [Google Scholar]
[11]. K Nakashima, T Sato, T Hara, S Minagi, An experimental study on histopathological changes in the tissue covered with denture base without occlusal pressureJ Oral Rehabil 1994 21:263-72. [Google Scholar]
[12]. GE Carlsson, Responses of jawbone to pressureGerodontology 2004 21:65-70. [Google Scholar]
[13]. K Oki, T Sato, T Hara, S Minagi, Histopathological changes in the tissues under a denture base in experimental osteoporosis with a non-pressure covering or bearing continuous pressureJ Oral Rehabil 2002 29:594-603. [Google Scholar]
[14]. V Chalian, MD Barnett, A new technique for constructing a one-piece hollow obturator after partial maxillectomyJ Prosthet Dent 1972 28:448-53. [Google Scholar]
[15]. M O’Sullivan, N Hansen, RJ Cronin, DR Cagna, The hollow maxillary complete ]denture: A modified techniqueJ Prosthet Dent 2004 91:59-64. [Google Scholar]
[16]. U Radke, D Mundhe, Hollow maxillary complete dentureJ Indian Prosthodont Soc 2011 11:246-49. [Google Scholar]
[17]. SS Manoj, V Chitre, M Aras, Management of compromised ridges: A case reportJ Indian Prosthodont Soc 2011 11:125-29. [Google Scholar]
[18]. LS Kaira, Maxillary hollow denture: A case seriesJournal of Orofacial Research 2012 2:109-12. [Google Scholar]