Slingshot – An Easy Way Out
Shilpa M Kendre1, Khushbu D Agrawal2, Suresh K Kangane3, Anand S Ambekar4
1 Postgraduate Student, Department of Orthodontics and Dentofacial Orthopedics, Maharashtra Institute of Dental Sciences and Research, Latur, Maharashtra, India.
2 Postgraduate Student, Department of Orthodontics and Dentofacial Orthopedics, Maharashtra Institute of Dental Sciences and Research, Latur, Maharashtra, India.
3 Professor and Head, Department of Orthodontics and Dentofacial Orthopedics, Maharashtra Institute of Dental Sciences and Research, Latur, Maharashtra, India.
4 Professor, Department of Orthodontics and Dentofacial Orthopedics, Maharashtra Institute of Dental Sciences and Research, Latur, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shilpa M Kendre, Postgraduate Student, Department of Orthodontics, Midsr Dental College, Vishwanathpuram, Ambajogai Road, Latur-413531, Maharashtra, India.
E-mail: shilpabikkad@yahoo.in
Orthodontic alignment of ectopically placed incisors or canines can be challenging and time consuming. A variety of techniques are used to align such palatally or lingually placed teeth including indirect ties with ligature wires, E-chains, piggy-back methods. This article presents two case reports to describe an effective technique using ‘slingshot’ method. It is a relatively simple and rapid method which is operator friendly and easily tolerated by the patients.
E-chains, Indirect ligature ties, Piggyback
Case 1
An 11-year-old female presented with chief complaint of malalinged teeth in upper and lower front region of jaw. On extraoral examination, patient had mild convex facial profile and incompetent lips, intraoral examination revealed end-on molar relation bilaterally, U-shape maxillary and mandibular arches and crowding in upper and lower anterior region [Table/Fig-1].
Treatment plan involved non-extraction treatment with arch expansion using MBT 0.022” prescription. Alignment started with 0.012”NiTi wire in upper and lower arches. Lower right lateral insisior was lingually placed and infraoccluded, therefore was not bonded initially. Lower left lateral incisor was also lingually placed but was corrected with initial archwires during alignment. NiTi open coil spring was placed with teeth #41-43 on reaching 0.018” SS wire to create space for tooth #42. After creating sufficient space, arch was consolidated into right and left segment and GIC bite block was given for opening the bite. Composite stopper was placed lingually on middle third of tooth #42. The power chain extended from lower left first permanent molar to lower right first permanent molar passing beneath the composite stopper on tooth #42 forming a sling [Table/Fig-2]. Re-activation of power chain was done after three weeks and tooth #42 was brought into line of arch in six weeks period [Table/Fig-3].
Case 2
A 22-year-old female presented with chief complaint of malalinged upper front teeth. On extraoral examination patient had straight profile and competent lips, intraoral examination revealed Class I molar relation bilaterally. Upper right and left canines (teeth #13,23) were palatally placed [Table/Fig-4].
Non-extraction treatment was planned for the patient since sufficient space was present between the upper right and left lateral incisors and first premolars for alignment of canines. Initial alignment was started with 0.016” NiTi wire. Maxillary canines were not bonded initially. After reaching 0.018” SS wire, Begg’s auxiliary bracket was bonded on maxillary canines palatally. The upper arch was consolidated into two posterior and one anterior segment and power chain was placed from upper right first permanent molar to upper left first permanent molar engaging the auxiliary bracket on canines forming slings around the canines [Table/Fig-5]. Re-activation of power chain was done after three weeks and (teeth #13,23) were brought into line of arch in six weeks [Table/Fig-6].
Pretreatment intraoral photographs showing lingually placed right lateral incisor in the lower arch.

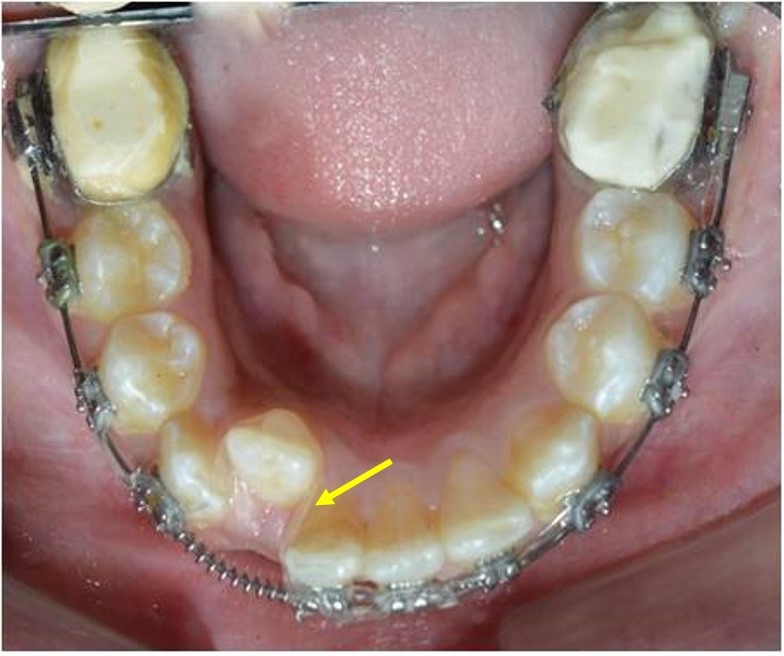
Power chain placed for alignment after reaching 0.018” stainless steel wire in a slingshot technique.
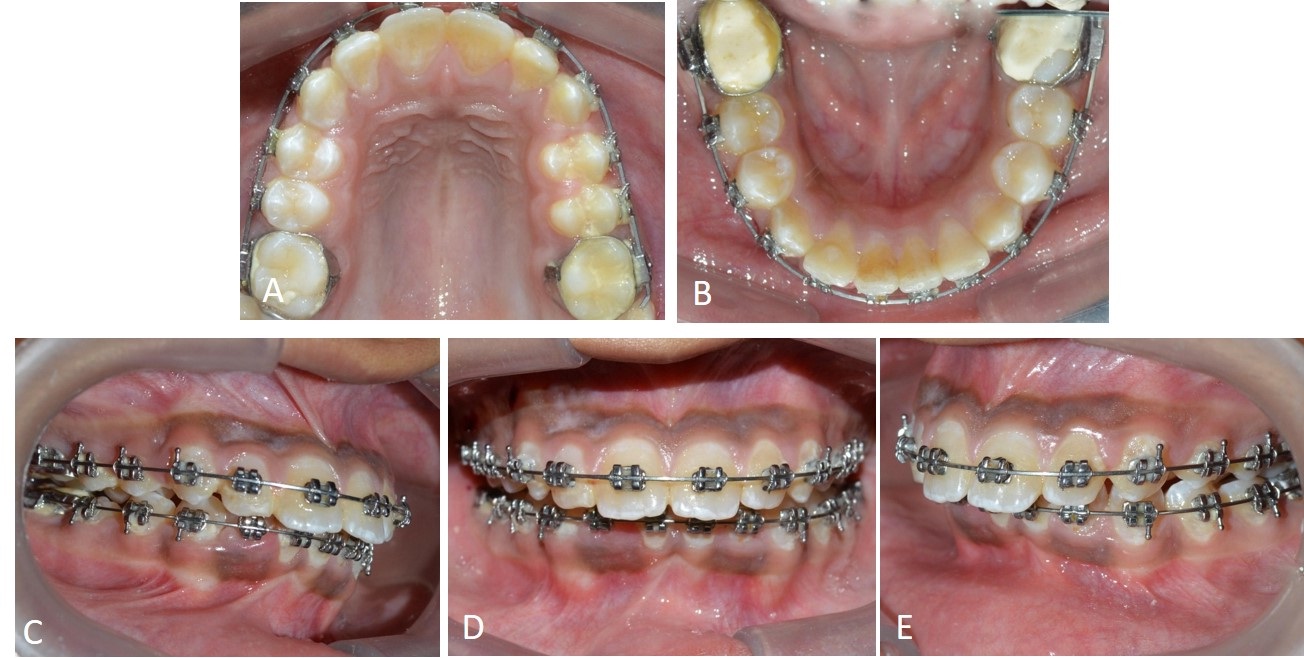
Post alignment intraoral photographs of lingually placed right lateral incisor in lower arch.
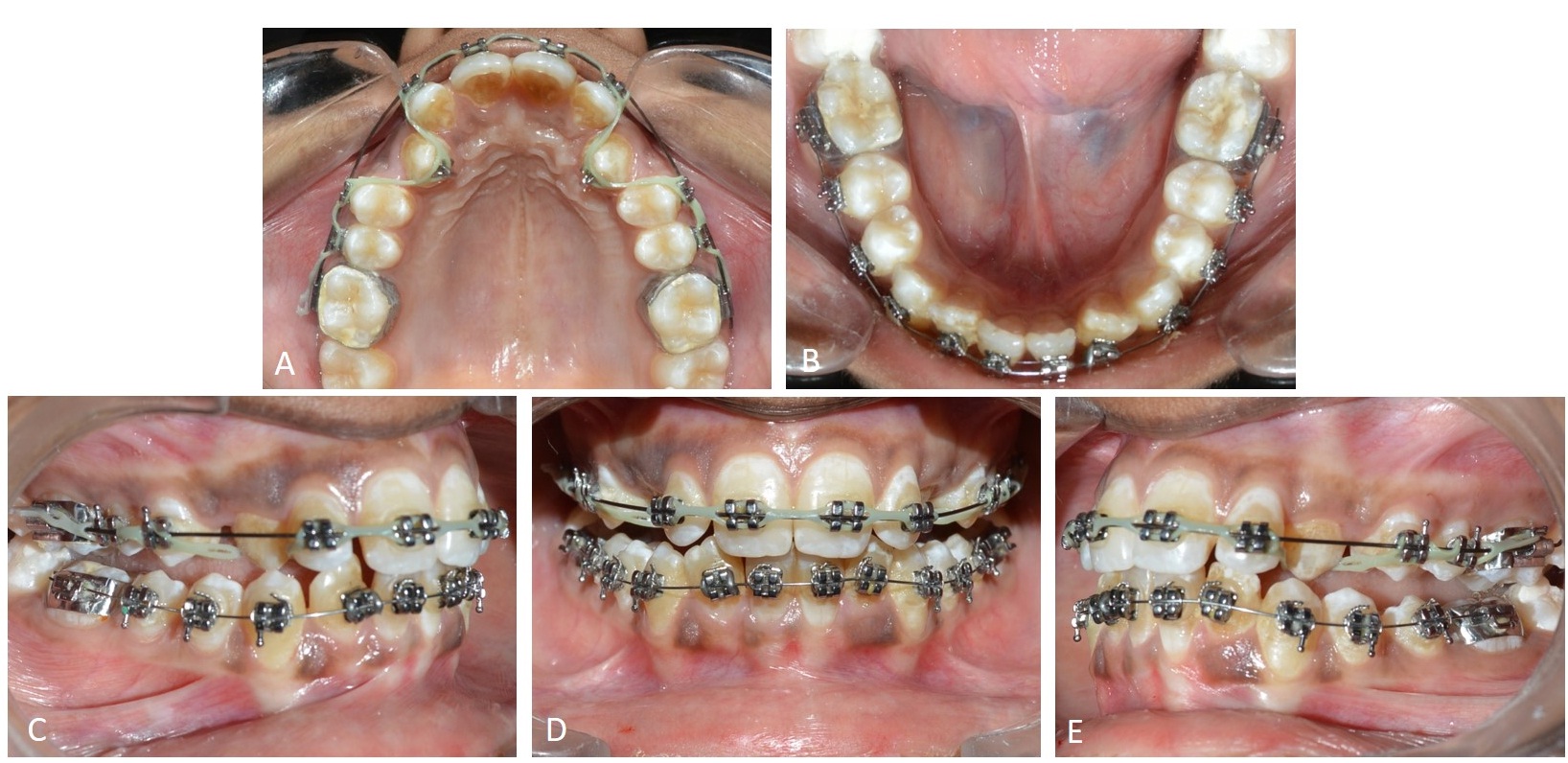
Pretreatment intraoral photographs showing bilaterally palatally placed canines (in crossbite) in upper arch.

Power chain placed for alignment after reaching 0.018” stainless steel wire in a slingshot technique.
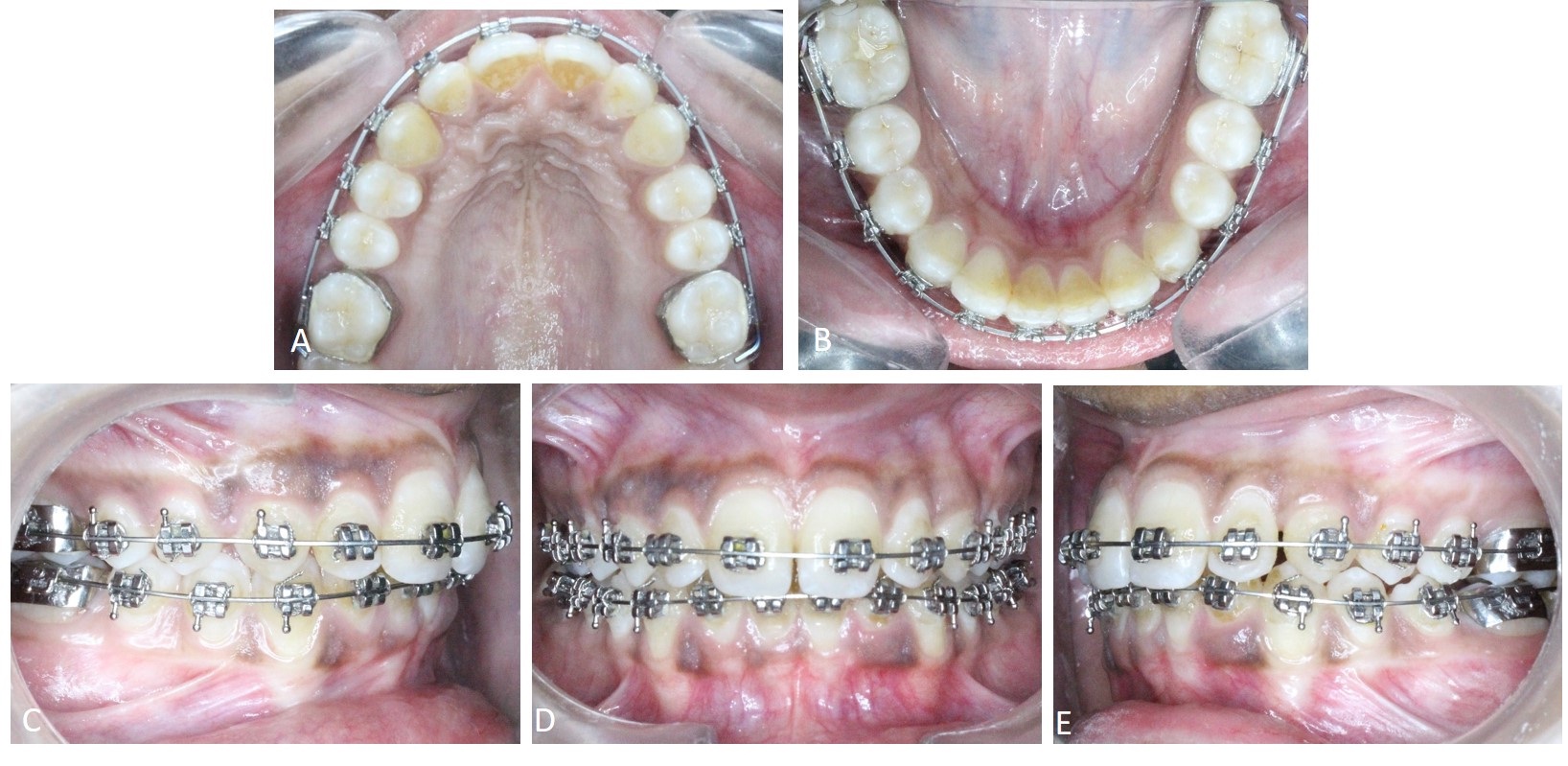
Post alignment intraoral photographs of bilaterally palatally placed canines in upper arch.
Discussion
The ‘slingshot’ method for palatally or lingually placed canines and lateral incisor alignment presented here requires the ectopic teeth to be in a position with a realistic prognosis for alignment.
Elastomeric chain can be used in the way described above to deliver differential forces that create traction directly into the line of the arch. By applying power chain in two segments: one to the distal wings of the bracket and the other to the mesial wings, the force vectors can be modified to produce the desired direction of movement. Khoshkhouejad G et al., have described the similar technique of slingshot for alignment of palatally impacted canines [1]. However, the technique described in the present article describes a relatively simple approach for completely erupted teeth which are ectopically placed. While using this technique, care should be taken to control the torque. As torque is best expressed at rectangular wire stage, we can expect to correct the root torque after reaching heavy stainless steel wire. Invert bracket position also helps to correct torque from beginning of the alignment phase. In our cases, torque was incorporated in the 0.019 x 0.025 inch stainless steel wire.
Kornhauser S et al., advocated that the use of power chain passing from the top produces an extrusive force as used in our first case for infraoccluded lower right lateral incisor [2].
Using elastomeric chain is relatively simple, and cost-effective in terms of time and materials. Good treatment outcomes can be achieved with any technique, if appliances and auxiliaries are used appropriately, whereas inappropriate direction of force application or inappropriate technique can cause unwanted side effects such as movement of adjacent teeth in the opposite direction in sagittal, transverse or vertical plane [1]. This can be avoided by consolidating the arch in two segments mesial and distal to the tooth to be moved as done in our presented cases.
Excessive force application can lead to formation of large areas of hyalinization, and therefore, it should be avoided. Anchorage must be assessed in all three dimensions and managed carefully to ensure that undesirable tooth movements are avoided [3].
Once the tooth is out of crossbite or aligned, one can bracket the tooth and finish any additional movement needed to complete the case. Typically, an anterior tooth takes four weeks to align and a posterior tooth takes eight weeks to align [4].
Conclusion
The ‘slingshot method’ described in this article to align palatally or lingually placed canines or lateral incisors is an operator friendly, efficient technique that is easily tolerated by patients. Also, it is a rapid technique for aligning the ectopically placed teeth into arch (three to six weeks) and is effective, predictable and can be easily incorporated into straight wire fixed appliance treatment.
[1]. G Khoshkhounejad, A Ulhaq, D Bister, The ‘slingshot’ technique to align palatally impacted canines with elastomeric chainJ Orthod 2015 42:153-58. [Google Scholar]
[2]. S Kornhauser, Y Abed, D Harari, A Becker, The resolution of palatally impacted canines using palatal-occlusal force from a buccal auxiliaryAm J Orthod Dentofacial Orthop 1996 110:528-34. [Google Scholar]
[3]. AJ Ireland, F McDonald, The orthodontic patient: Treatment and biomechanics 2003 Oxford, New YorkOxford University Press [Google Scholar]
[4]. DePaul Richard J, The Slingshot. Clinical pearls Aug 2012. Available from http://www.orthodonticproductsonline.com/2012/09/clinical-pearls/ [accessed on-19/1/17] [Google Scholar]