Morel-Lavallee lesion is a post-traumatic soft tissue degloving injury. This is commonly associated with sports injury caused by a shearing force resulting in separation of the hypodermis from the deeper fascia. Most common at the greater trochanter, these injuries also occur at flank, buttock, lumbar spine, scapula and the knee. Separation of the tissue planes result in a complex serosanguinous fluid collection with areas of fat within it. The imaging appearance is variable and non specific, potentially mimicking simple soft tissue haematoma, superficial bursitis or necrotic soft tissue neoplasms. If not treated in the acute or early sub acute settings, these collections are at risk for superinfection, overlying tissue necrosis and continued expansion.
In this review article, we discuss the clinical presentation, pathophysiology, imaging features and differential diagnostic considerations of Morel-Lavallee lesions. Role of imaging in guiding prompt and appropriate treatment has also been discussed.
Introduction
Morel-Lavallee lesion, initially described by French surgeon Maurice Morel-Lavallee in 1853, is a post-traumatic closed degloving injury where skin and superficial fascia get separated from deep fascia, creating a potential space [1]. Injury to rich vascular and lymphatic supply leads to accumulation of blood and lymph in this potential space generated by separation of the superficial and deep fascia. Blood products and necrotic material inturn invokes chronic inflammatory reaction. As the time progress, a capsulated lesion lined by fibrous capsule develops, which is filled with blood products, necrotic fatty tissue, debris and fibrin [2]. Morel-Lavallee lesions usually present as painful fluctuant swelling in the involved sites. Many of these may be missed at initial evaluation and present weeks to month after initial trauma.
Pathophysiology
Though motor vehicle accidents are the most common aetiology, low grade blunt force trauma including falls and sport related injuries account for a significant minority of cases [2]. Postoperative cases have also been reported, especially following liposuction [2]. The greater trochanter is the most commonly involved region, accounting for over 60% of the cases. Predisposing factors include the superficial position of the femoral cortex, relative mobility of the subdermal soft tissues and strength of the underlying tensor fascia lata [3]. Secondary risk factors include female gender and a body mass index of 25 or greater. With disruption of the subdermal capillaries and lymphatics, haemorrhage, lymphatic fluid and locules of subdermal fat pool in the suprafascial tissue plane. Over time, there is resorption of the haemorrhagic elements, increasing serosanguinous fluid and progressive fibrous encapsulation, hindering resorption and thus leading to slow continued expansion [2].
Clinical Presentation
Clinical presentation of Morel-Lavallee lesions is usually in close proximity to the inciting traumatic event, though upto one third of the patients may have a delayed presentation with gradually increasing swelling, months or years after the initial injury. Pain and swelling are the most frequent clinical complaints, with a compressible, fluctuant area typically detectable on physical examination. Clinical findings may mimic a regional contusion or even deep venous thrombosis. Cutaneous hypothesia or anaesthesia may be observed due to disruption of the subdermal afferent nerves [2]. Overlying secondary dermal changes including drying and cracking, discolouration and even frank necrosis may also occur.
Role of Imaging
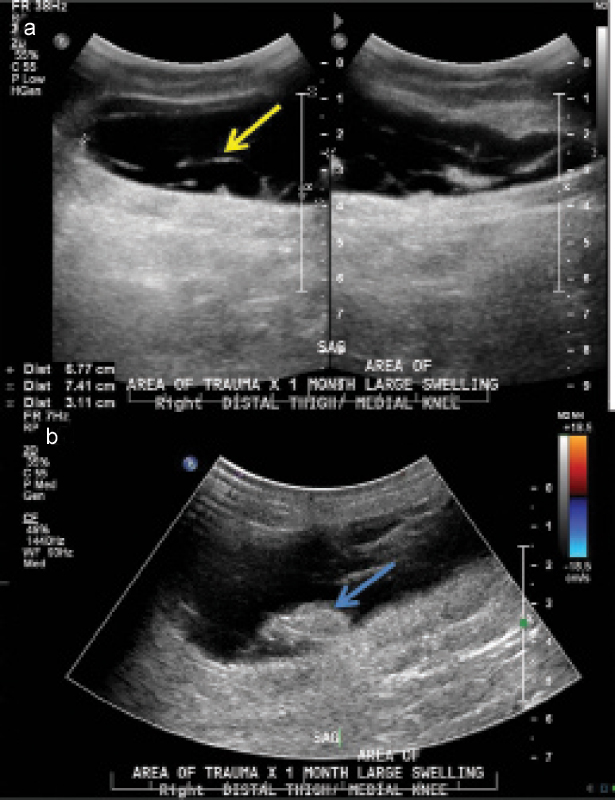
Various imaging modalities including Ultrasonography (USG), Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) can be used to diagnose and characterize Morel-Lavallee lesions [2]. USG is a rapid, readily available, inexpensive modality which allows real time evaluation, including dynamic imaging. However, it is non specific, operator dependent and cannot be performed optimally in the areas with open wounds and dressings. USG demonstrates a variable appearance of Morel-Lavallee lesions with diagnosis being in part, both history and location driven. Acute lesions are usually ill defined and demonstrate heterogeneous echogenicity [Table/Fig-1]. They can mimic abscesses, simple haematomas, fat necrosis and neoplasms. Chronic lesions are better defined, homogeneous and smoothly marginated, which is due to tendency of these lesions to form pseudocapsules [2]. Chronic collections may demonstrate variable flow within the surrounding fibrous capsule on colour Doppler imaging [Table/Fig-1]. Differential diagnoses for chronic lesions include seromas, bursitis, lymphoceles and neoplasms. Thus, USG can be very non specific in the diagnosis of Morel-Lavallee lesions and its main role lies in USG guided percutaneous drainage of the Morel-Lavallee lesions [2].
A 57-year-old man with medial thigh swelling status post fall. Ultrasound images of right medial thigh a) and b) demonstrates heterogeneous collection with internal septations (yellow arrow) and echogenic focus (blue arrow). Please note that there is no internal vascularity within the echogenic focus (blue arrow).
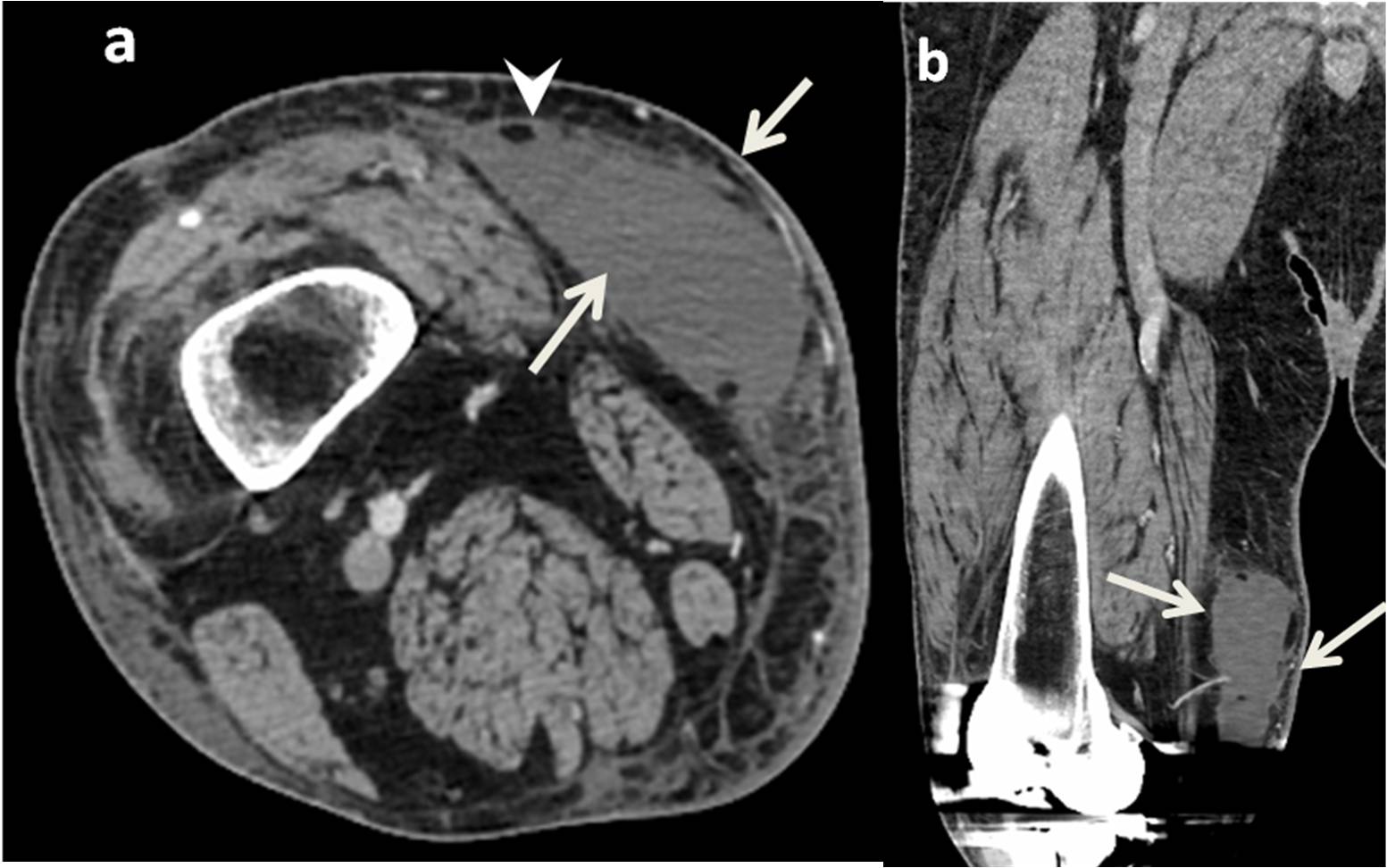
CT is readily available and fast in image acquisition; it poses significant radiation risk and does not readily allow soft tissue characterization [4]. CT has been the initial modality of choice, especially in acute trauma cases [4]. CT imaging findings include internal complexity and a fluid/fluid layer reflecting of internal settling of serosanguinous elements admixed with lymphatic fluid [Table/Fig-2]. CT density is usually lower than simple haematomas due to mixing of low density lymphatic fluid and averages from 15-40 Hounsfield units [4]. Presence of classical subdermal location and the detection of fat globules help characterization [Table/Fig-2]. Acute Morel-Lavallee lesions are usually ill defined with surrounding fat stranding, while subacute or chronic lesions are well defined [Table/Fig-3]. Detection of a well defined capsule has prognostic implications reflecting the necessity for percutaneous drainage with sclerotherapy or surgical excision [Table/Fig-4] [5].
CT scan of the same patient as in [Table/Fig-1]. CT right thigh a) axial and b) coronal section demonstrate hypodense collection in medial thigh subcutaneous planes. Foci of fat attenuation within the collection (white arrowhead).
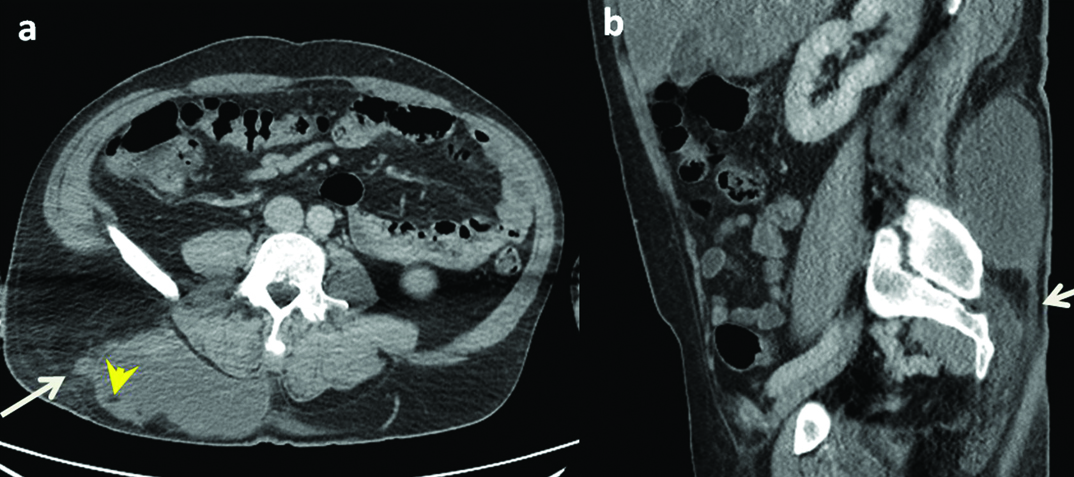
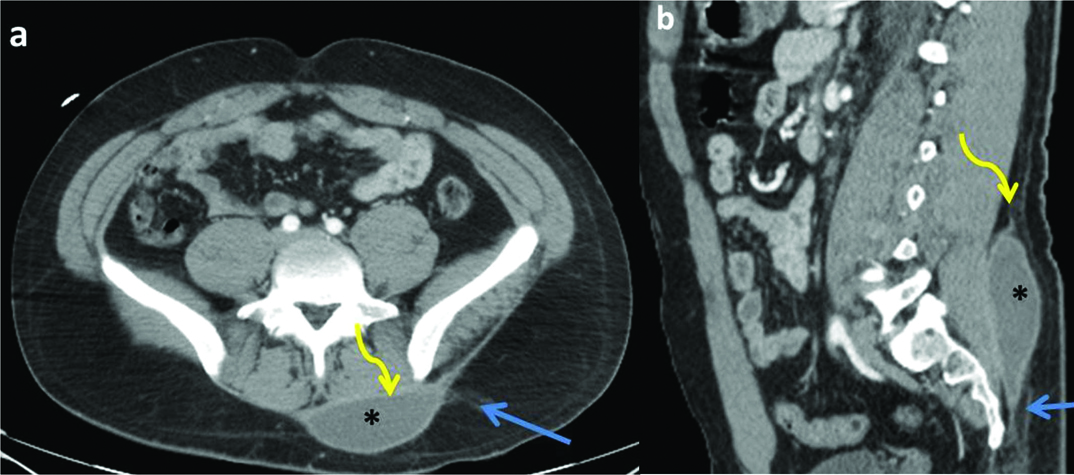
A 50-year-old man with back swelling status post-trauma. CT abdomen, a) axial and b) sagittal images demonstrate a large heterogeneous collection with fluid, fat (yellow arrowhead) and blood attenuation areas in the subcutaneous planes of right posterior lower back consistent with Morel Lavallee lesion (sub-acute haematoma). There is fat infiltration in adjacent soft tissue (white arrows).
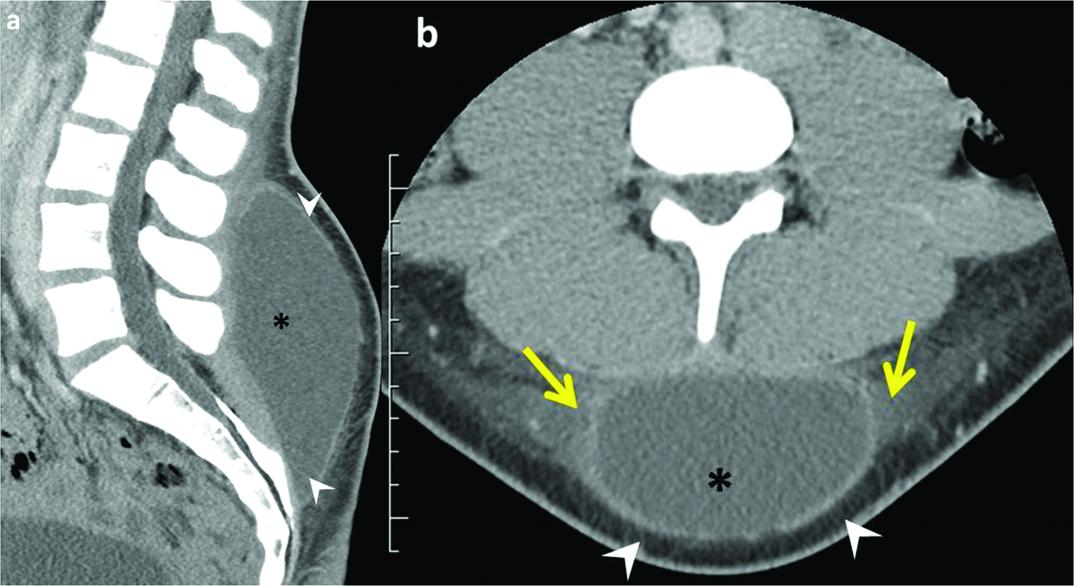
A 17-year-old man, status post-trauma with lower back swelling. CT lumbar spine, a) sagittal and b) axial images demonstrate a large well circumscribed thick walled hypodense collection (black asterix) in the subcutaneous plane overlying the thoracolumbar fascia. There is mild wall enhancement (white arrowheads) and adjacent subcutaneous fat infiltration (yellow arrows).
MRI is the imaging modality of choice for Morel-Lavallee lesions, due to high contrast resolution, multiplanar acquisition and greater anatomic details [6,7]. MRI in general is the imaging modality of choice for soft tissue musculoskeletal tumours, injuries as well as spinal trauma [7-9]. Similarly, MRI is the imaging modality of choice with its greatest utility in characterizing Morel-Lavallee lesions based on composition characteristics and chronicity [Table/Fig-5]. Acute lesions have heterogeneous signal intensity with surrounding muscle and soft tissue oedema, which is best identified on the STIR images. Chronic lesions may demonstrate internal simple fluid signal intensity, hypointense to soft tissue on T1 imaging and homogeneously hyperintense on T2 due to complete resorption of internal clot. Internal areas of heterogeneous T1 hyperintensity can also be seen corresponding to intra and extracellular methaemoglobin [Table/Fig-5] [7]. Over time, a peripheral enhancing low T1/T2 capsule may form. Internal areas of lipomatous signal intensity, when present, aid in characterization [Table/Fig-6].
Same patient as in [Table/Fig-4]. MRI lumbar spine sagittal a) T1, b) T2 and; c) and d) axial T1 & T2 images demonstrate a lenticular shaped collection between the thoracolumbar fascia and overlying subcutaneous fat and superficial fascia consistent with Morel-Lavallée. There is mild T1 hyperintensity relative to muscles with an internal area of T1 and T2 hypointensity (yellow arrowheads) representing retracted clot. There is hypointense capsule (blue arrow) and internal septations. Ultrasound images of the same region e) and f) demonstrate hypoechoic collection with septations (white arrowheads).
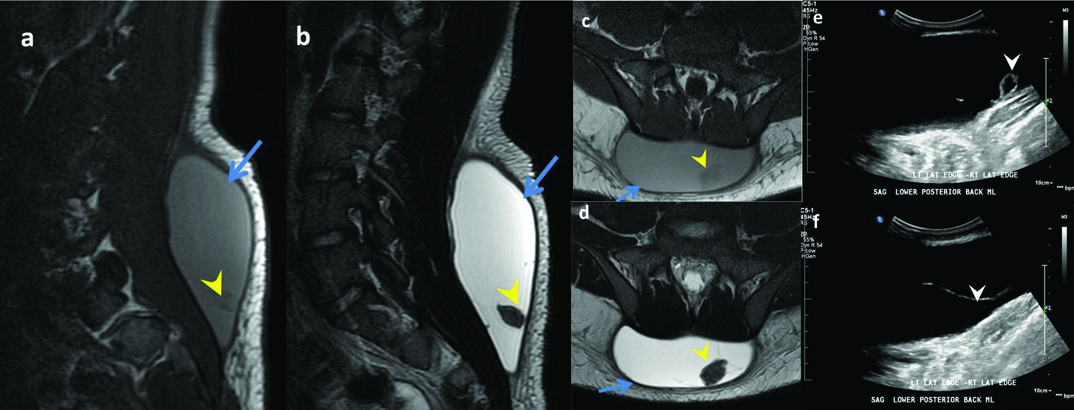
A 16-year-old man, post fall with marked tenderness at lumbosacral region and right leg numbness. MRI lumbar spine a) sagittal T1 weighted, b) T2 and c) STIR images demonstrate a small T1 hypointense (white asterix) and T2 and STIR hyperintense homogeneous collection (black asterix). The collection is between the thoracolumbar fascia (yellow arrows) and overlying subcutaneous fat and superficial fascia (blue arrows) consistent with Morel-Lavallée lesion.
In 2005, Mellado JM and Bencardino JT proposed an extensive six stage imaging based classification based on the shape of lesion, signal intensity on T1 and T2 weighted images, presence of fibrous capsule, contrast enhancement and sinus tract formation capsule [7].
Type I Morel-Lavallee lesion-Seroma appearing as a homogeneously hypointense on T1 Weighted Image (T1WI) and hyperintense collection on T2 Weighted Images (T2W2), without evidence of outer capsule formation.
Type II Morel-Lavallée lesion-Subacute haematoma appearing as homogeneously hyperintense on both T1WI and T2WI due to the presence of methaemoglobin, a characteristic of subacute haematomas.
Type III Morel-Lavallee lesion-Chronic organizing haematomas demonstrating hypointensity on T1WI and heterogeneous hypointensity/isointensity on T2WI with capsular formation. On post contrast sequences, Type III lesions may show capsular and internal enhancement secondary to neovascularization and granulation tissue in the organizing haematoma. This can even lead to growth over time.
Type IV Morel-Lavallee lesion-Represents a closed laceration, with the absence of a capsule. It shows T1 hypointense and T2 hyperintense signal.
Type V Morel-Lavallee lesion-Demonstrates a small, rounded, pseudo nodular appearance and have variable T1 and T2 signal intensity.
Type VI Morel-Lavallee lesion-Represents superimposed infection, with a thick enhancing capsule and can be associated with sinus tract.
However, a classification of acute vs. chronic lesions based on the presence or absence of a detectable capsule is more commonly used for treatment purposes. Capsule formation warrants surgical treatment for complete cure and to avoid risk of infection [Table/Fig-7]. Diffusion weighted MRI is especially helpful in differentiating Morel-Lavallee lesions and necrotic tumours from the abscesses as well as infected Morel-Lavallee lesions by showing central restriction in the central portion in the later [10,11].
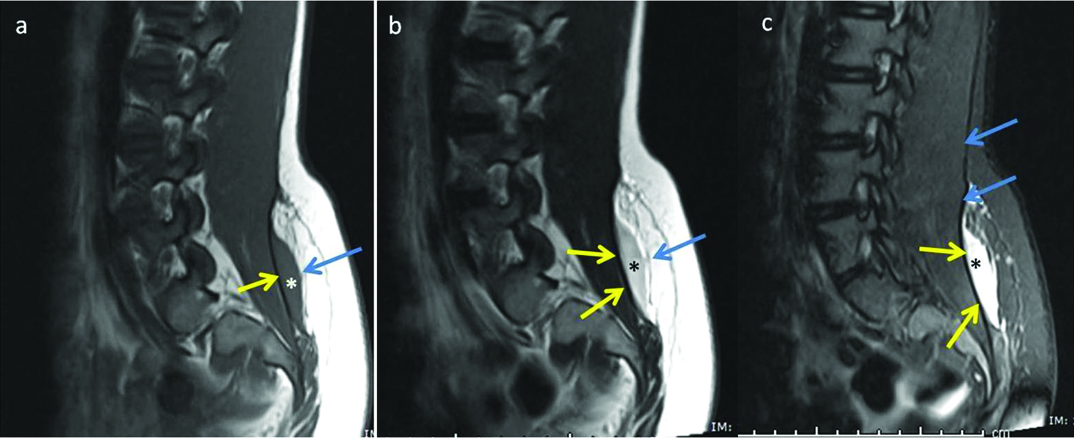
A 26-year-old man with motor vehicle crash. CT images of the pelvis a) axial and b) sagittal images shows a well circumscribed lenticular shaped hypodense collection (black asterix) with enhancing rim. Please note the preserved fat plane (yellow curved arrow) between the paraspinal muscles and the collection signifying the collection is external to the fascia. Blue arrow signifies the inflamed fascia.
Differential Diagnosis
The imaging characteristics of Morel-Lavallée lesions and alternative diagnoses, such as simple subcutaneous haematomas demonstrate significant overlap [Table/Fig-8]. In the acute settings, the diagnosis can be challenging as the appearances can be indistinguishable. However, in a patient with the appropriate clinical history and a fluid collection in a typical location, a diagnosis of Morel-Lavallée lesion is likely. In equivocal cases, follow up imaging may be useful to demonstrate the chronological changes described above. Necrotic soft tissue tumours can mimic Morel-Lavallée lesions; however, they can be differentiated from each other after contrast administration as described above [12]. Bursitis at locations similar to that of Morel-Lavallée lesions can also mimic this entity, but can be differentiated based on the extent as described above [7,10,11,13-15].
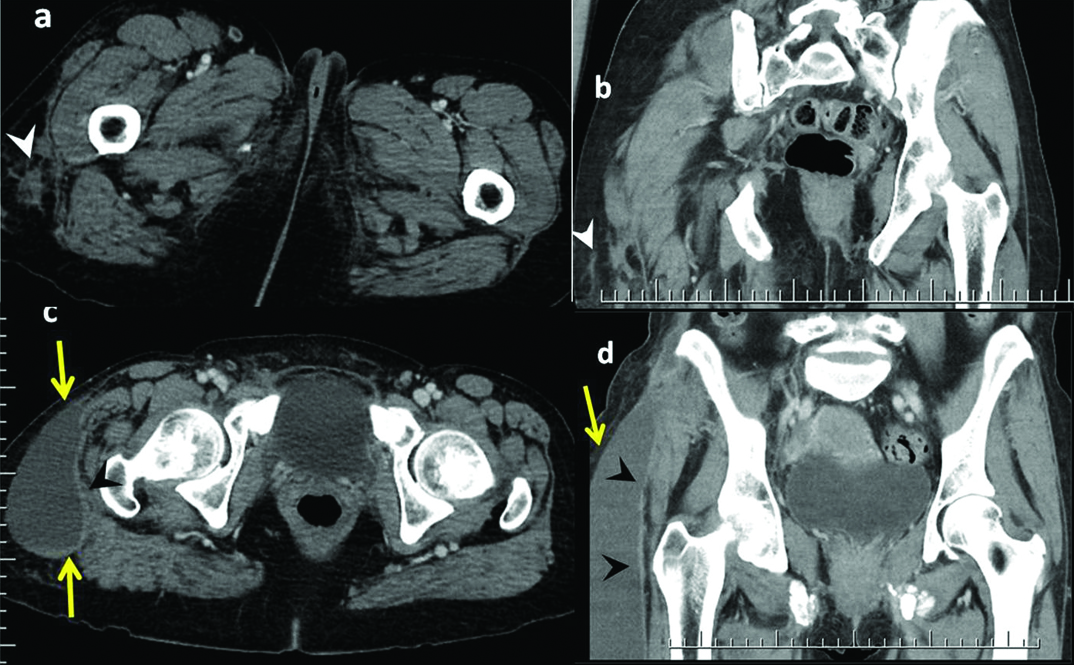
A 55-year-old woman, who had been in a motor vehicle accident with right hip pain. CT scan pelvis performed in 12 hours, a) axial and b) coronal images demonstrate heterogeneous irregular soft tissue attenuation posterolateral right thigh (white arrowhead), which can mimic a necrotic soft tissue tumour. Follow up CT pelvis after 12 days, c) axial and d) coronal images demonstrate a well defined organized fluid collection (yellow arrows) with a partially defined capsule superficial to tensor fascia lata/iliotibial band (black arrowheads). There is a mild peripheral enhancement.
Treatment Options
Treatment strategies are based on the stage of Morel-Lavallee lesion as per above classification pattern [2]. Many strategies for the treatment of Morel-Lavallee lesions have been reported and there are no established treatment modalities for patients with Morel-Lavallee lesions. First line therapies, in patients with acute, small lesions without underlying fractures usually include compression bandage application, NSAID medications, physiotherapy and absolute bed rest [16].
USG or CT guided percutaneous drainage can be used for larger acute lesions. It may also be attempted along with sclerotherapy in patients with chronic lesions [17]. Talc sclerotherapy and the use of alcohol and doxycycline, have also been reported [18,19]. Sclerotherapy can be used as a first line therapy in patients with acute lesions that are refractory to compression bandages and in patients with chronic lesions [5,20].
Open debridement as a first line therapy has been attempted in patients with acute lesions with underlying open fractures and chronic lesions with evidence of infection or tissue necrosis due to a local mass effect [12]. In patients who are refractory to percutaneous drainage with sclerotherapy, open debridement may also be considered as the final therapy. Surgical intervention is also indicated in patients with longstanding Morel-Lavallee lesions with pseudocapsule because they are unresponsive to percutaneous drainage and therefore vulnerable to recurrence [20]. MRI is thus helpful in characterizing the lesions stage and presence of pseudocapsule to decide surgical vs non surgical treatment.
Conclusion
Closed degloving injuries are an uncommon clinical entity, and are often misdiagnosed resulting in persistent symptoms and delay in appropriate management. Imaging plays an important role in the diagnosis and management. MRI is the imaging modality of choice in the diagnosis and characterization of Morel-Lavallee lesions, which helps in prompt and appropriate treatment planning. In equivocal cases follow up imaging may be useful to demonstrate the typical chronological changes seen on MRI and USG. It is very critical for the radiologists to be aware of the various imaging findings of Morel-Lavallée lesions and its mimics to help the referring clinician in proper management.
[1]. Kumar Y, Hooda K, Lo L, Karol I, Morel-Lavallée lesion: A case of an American football injuryConnecticut Medicine 2015 79(8):477-78. [Google Scholar]
[2]. Bonilla-Yoon I, Masih S, Patel DB, White EA, Levine BD, Chow K, The Morel-Lavallée lesion: Pathophysiology, clinical presentation, imaging features, and treatment optionsEmerg Radiol 2014 21(1):35-43. [Google Scholar]
[3]. Hak DJ, Olson SA, Matta JM, Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: The Morel-Lavallee lesionJ Trauma 1997 42(6):1046-51. [Google Scholar]
[4]. McKenzie GA, Niederhauser BD, Collins MS, Howe BM, CT characteristics of Morel-Lavallée lesions: An under-recognized but significant finding in acute trauma imagingSkeletal Radiol 2016 45(8):1053-60. [Google Scholar]
[5]. Isaacson AJ, Stavas JM, Image-guided drainage and sclerodesis of a Morel-Lavallee lesionJ Vasc Interv Radiol 2013 24(4):605-06. [Google Scholar]
[6]. Mellado JM, Perez del Palomar L, Diaz L, Ramos A, Sauri A, Long-standing Morel-Lavallee lesions of the trochanteric region and proximal thigh: MRI features in five patientsAJR Am J Roentgenol 2004 182(5):1289-94. [Google Scholar]
[7]. Mellado JM, Bencardino JT, Morel-Lavellee lesion: Review with emphasis on MR imagingMagn Reson Imaging Clin N Am 2005 13(4):775-82. [Google Scholar]
[8]. Kumar Y, Hayashi D, Role of magnetic resonance imaging in acute spinal trauma: A pictorial reviewBMC Musculoskelet Disord 2016 17:310 [Google Scholar]
[9]. Kumar Y, Hayashi D, Role of Imaging in musculoskeletal careCurr Phys Med Rehabil Rep 2016 4:28-36. [Google Scholar]
[10]. Kumar Y, Wadhwa V, Phillips L, Pezeshk P, Chhabra A, MR imaging of skeletal muscle signal alterations: Systematic approach to evaluationEur J Radiol 2016 85(5):922-35. [Google Scholar]
[11]. Kumar Y, Khaleel M, Boothe E, Awdeh H, Wadhwa V, Chhabra A, Role of diffusion weighted imaging in musculoskeletal infections: Current perspectivesEur Radiol 2017 27(1):414-23. [Google Scholar]
[12]. Kumar S, Hasan R, Kadavigere R, Maddukuri SB, Puppala R, Morel-Lavallee Lesion (MLL) Mimicking a soft tissue neoplasmJ Clin Diagn Res 2015 9(4):TD01-02. [Google Scholar]
[13]. Borrero CG, Maxwell N, Kavanagh E, MRI findings of prepatellar Morel-Lavallee effusionsSkelet Radiol 2008 37(5):451-55. [Google Scholar]
[14]. Tsai TS, Evans HA, Donnelly LF, Bisset GS 3rd, Emery KH, Fat necrosis after trauma: A benign cause of palpable lumps in childrenAJR Am J Roentgenol 1997 169(6):1623-26. [Google Scholar]
[15]. Donahue F, Turkel D, Mnaymneh W, Ghandur-Mnaymneh L, Haemorrhagic prepatellar bursitisSkelet Radiol 1996 25(3):298-301. [Google Scholar]
[16]. Tejwani SG, Cohen SB, Bradley JP, Management of Morel-Lavallee lesion of the knee: Twenty-seven cases in the national football leagueAm J Sports Med 2007 35(7):1162-67. [Google Scholar]
[17]. Tseng S, Tornetta P 3rd, Percutaneous management of Morel-Lavallee lesionsJ Bone Jt Surg Am 2006 88(1):92-96. [Google Scholar]
[18]. Luria S, Applbaum Y, Weil Y, Liebergall M, Peyser A, Talc sclerodhesis of persistent Morel-Lavallee lesions (posttraumatic pseudocysts): Case report of 4 patientsJ Orthop Trauma 2006 20(6):435-38. [Google Scholar]
[19]. Bansal A, Bhatia N, Singh A, Singh AK, Doxycycline sclerodesis as a treatment option for persistent Morel-Lavallee lesionsInjury 2013 44(1):66-69. [Google Scholar]
[20]. Demirel M, Dereboy F, Ozturk A, Turhan E, Yazar T, Morel-Lavallee lesion. Results of surgical drainage with the use of synthetic glueSaudi Med J 2007 28(1):65-67. [Google Scholar]