The anatomy and physiologic characteristics of the tongue and its environment should be evaluated thoroughly before the fabrication of complete dentures. The tongue must engage in the normal physiologic acts of speech, mastication and deglutition and at the same time helps to stabilize the complete denture. Any abnormalities jeopardize the success of such dentures [1,2]. The functional abilities of the tongue are its size, strength, state of health, movement patterns and resting position. The prosthodontic rehabilitation of the edentulous mandibular jaw can lead to poor denture retention and stability due to the presence of an unfavourable resting tongue position [3]. This retracted position results in a broad lingual sulcus displacing the tissues overlying the sublingual gland posteriorly; as a result the seal between the mucosa and the denture periphery is broken. Wright CR et al., were the first to publish on tongue position and its relation to denture stability and researchers have classified tongue position into normal and abnormal tongue position with the relevant distinguishing criteria [2-4]. It has been concluded that, the abnormal tongue position develops as a reflex and relates to certain functional or even parafunctional habits. At birth, all possess a normal tongue position and the abnormal is the one which is developed due to aging, abnormal swallowing habits and missing teeth [2,3]. It is evident from literature that, the prevalence of retracted tongue position is common in completely edentulous condition irrespective of duration of edentulousness [4]. The present study was undertaken to evaluate resting tongue position among recently extracted (<1 year) and long term completely edentulous subjects (>1-10 year) based on the duration of edentulousness and also to assess the efficacy of a simple modification of complete denture along with certain tongue exercises to reorient retracted tongue position to normal position.
Materials and Methods
This was a Prospective interventional study carried out in the Department of Prosthodontics, College of Dental Sciences, Davangere, Karnataka over a period of 12 months from 2009 to 2010. A total of 62 study subjects participated in the study. In this study, alpha error was set to 5% and beta error to 20% and the power of the study was 80%. Hence, the study considered minimum of 30 subjects in each group and as well as depending on number of eligible patients that could be recruited during the study period, the sample size 30 was in Group A and 32 in Group B.
Group A (n=30): Recently extracted completely edentulous subjects (<1 year).
Group B (n=32): Long term completely edentulous subjects (>1-10 year).
Forty male and 22 female patients were selected between the ages of 50-75 years. A proforma was obtained for each subject to note down study related information (age, sex, duration of edentulouness, reasons for loss of teeth etc.,). The resting tongue position was observed while the patient was unaware of what the dentist was examining [3]. During the present study, the resting tongue position was recorded at the beginning of the examination. Additionally, the position was checked at the end of the examination, after the patient had opened the mouth a number of times and felt somewhat more relaxed. During each examination, the patients were instructed to stay calm and advised to open the mouth slowly so that the dentist could observe tongue position. In the cases, where the tongue appeared abnormal, the patients were instructed to close, swallow and open again. The whole organ had to appear relaxed and free of muscular contractions when the recording was performed.
The tongue position was categorized by:
The extent by which the floor of the mouth is visible.
The lateral borders, in relation to the lingual surfaces of teeth or lingual side of the ridge.
The apex, in relation to the lingual surface of the teeth or lingual anterior side of the ridge.
Using the above criteria, the tongue resting position was grouped as follows [2-4].
Normal upper: Floor not visible; lateral borders over the occlusal surface, or on the ridge; apex behind or over the lingual surfaces of anteriors, or on the ridge.
Normal lower: Floor not visible, lateral borders next to lingual surfaces, or inside the ridge; apex behind the lingual surfaces of the anteriors or behind the ridge anteriorly.
Abnormal upper: Floor visible, lateral borders over the occlusal surfaces, or behind the end of the ridge, apex withdrawn into the body.
Abnormal lower: Floor visible, lateral borders behind the posterior teeth, or next to the end of the ridge; apex pointing (lowered) to the floor of mouth.
The patients who had retracted tongue position, a simple modification was done in their complete denture to reorient to normal resting tongue position. At wax try in appointment, a bleb or bead of modelling wax of 3 mm-4 mm was added inferior and lingual to incisal edge of lower central incisors. Bleb of wax was in configuration of half sphere and slightly over waxed to compensate for final polish [Table/Fig-1].
Bleb of wax placed behind the lower central incisors.

Following which the dentures were processed, finished and polished. Later, the bleb area was roughened with sandpaper to give matty finish for the tongue to detect and feel it easily [5,6].
The patients were instructed to feel the bleb of acrylic resin with tip of tongue and train themselves to keep the tongue in normal position for a period of eight months. Also, a simple series of tongue exercises were explained to the patients such as thrusting tongue out and in, swinging the tongue sideways and raising tongue to its highest position [4]. Patients were advised to practice tongue exercises twice daily initially for a period of 5-10 minutes and more frequently later. Patients were followed up and recalled intermittently (once a month) to check whether they were following the given instructions. At the end of eight months, patients were evaluated for resting tongue position.
Statistical Analysis
The data was entered and analysed in SPSS 16.0 using statistical tests like mean, standard deviation, proportion, Chi-square test and McNemar Test.
Results
For the total subjects (n=62), it was observed that the resting tongue position was found normal in 28 patients (45.1%) and abnormal in 34 patients (54.9%). However, in Group A (n=30), the normal position encountered was 60% and the abnormal in 40%. Among Group B study subjects (n = 32), normal position encountered was 31.2% and the abnormal in 68.8%. The study subjects of Group B presented abnormal position in high percentage when compared to Group A. The difference was found to be significant between the two groups [Table/Fig-2]. The variables such as age, sex, duration of edentulousness were considered. The relationship between age, sex and resting tongue position was found to be not significant [Table/Fig-3,4].
Frequency distribution of normal tongue position v/s retracted tongue position among Group A and B. * < 1 year, # > 1 year
| Edentulous duration | Normal TonguepositionN (%) | Retracted TonguepositionN (%) | Total | Chi-square | df | p-value |
|---|
| Group A* | 18 (60.0%) | 12 (40.0%) | 30 (100%) | 5.16 | 1 | 0.02 |
| Group B# | 10 (31.2%) | 22 (68.8%) | 32 (100%) |
| Total | 28 (45.1%) | 34 (54.9%) | 62 (100%) |
Age-wise distribution of normal tongue position v/s retracted tongue position among the study subjects.
| Age | Normal TonguepositionN (%) | Retracted TonguepositionN (%) | Total | Chi-square | df=1 | p-value |
|---|
| < 60 years | 9 (50.0%) | 9 (50.0%) | 18 (100%) | 0.24 | 1 | 0.62 |
| > 60 years | 19 (43.1%) | 25 (56.9%) | 44 (100%) |
| Total | 28 (45.1%) | 34 (54.9%) | 62 (100%) |
Sex-wise distribution of normal tongue position v/s retracted tongue position among the study subjects.
| Sex | Normal TonguepositionN (%) | Retracted TonguevpositionN (%) | Total | chi-square | df=1 | p-value |
|---|
| Male | 18 (45.0%) | 22 (55.0%) | 40 (100%) | 0.001 | 1 | 0.97 |
| Female | 10 (45.4%) | 12 (54.6%) | 22 (100%) |
| Total | 28 (45.1%) | 34 (54.9%) | 62 (100%) |
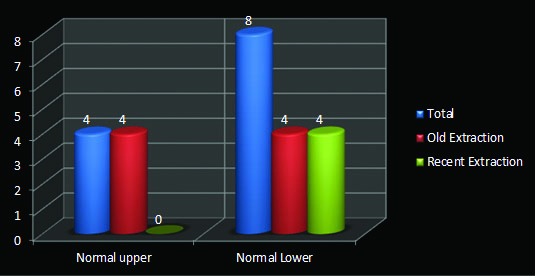
After the intervention, out of 34 retracted tongue position study subjects, 42.8% had achieved normal resting tongue position. Normal upper resting tongue position was observed in four patients and normal lower resting tongue position was observed in eight patients [Table/Fig-5]. A statistical test (McNemar) was done to find the significant difference of retracted tongue position before and after intervention and it was found to be significant.
Normal resting tongues position after intervention.
Binomial distribution followed, McNemar test was done to find the significance, p = 0.03 (significant)
Discussion
The development of the mandibular border seal depends on continuous contact of the tissues of the floor of mouth and the retromylohyoid region with the denture border and simultaneously constant contact of the tongue with the external surface of the lingual flange of the mandibular denture. This contact of tissues and denture must be maintained at rest and during normal range of function. Excessive tongue movements will break the border seal and create an unstable denture [1]. Normal resting and functional movements of the tongue, however, should maintain the border seal. If the tongue assumes a retracted position, the development and maintenance of border seal is prevented. Retraction of the tongue into the oropharynx prevents its contact with the lingual flange anteriorly and distorts the relationship of tissues of the floor of the mouth and the retromylohyoid region to the denture border. When this happens, the finished denture will have no border seal at rest and will float [1,7,8]. The retracted position is therefore an important diagnostic factor to be considered in relation to border seal, and mandibular denture stability [2,4,7,8]. The distinction between upper and lower position, was facilitated by the appearance of the floor, which seemed to acquire in some cases an upper and in others a lower position. Authors reported that the upper and lower normal position is usually influenced by the palatal vault [3]. When the natural teeth are missing, the tongue fills edentulous space and becomes enlarged. During function, the chewing and swallowing procedures may again need to be altered due to change in its apparent volume. According to above, this whole situation favours the development of habit [3,9,10].
Kotsiomiti E and Kapari D in their epidemiological study determined the incidence of abnormal tongue position among edentulous patients as opposed to dentate and revealed that, the prevalence of retracted tongue position was common in completely edentulous condition irrespective of duration of edentulousness [3]. The present study evaluated resting tongue position based on the duration of edentulousness. It showed that high percentage of abnormal tongue position was encountered in the groups of subjects who were edentulous for a long period. It would seem possible that this high percentage originates from the functional changes of stomatognathic system induced by the edentulousness and abnormal swallowing habits [1,3,4,11].
There is no doubt that the fabrication of complete denture becomes more complicated in the patient presented with retracted tongue position [1,12-17]. Likeman PR, had suggested a clinical method to improve stability of mandibular denture in patients with retracted tongue position by placing a bleb of wax behind the lower central incisors and encouraged to practice them [6]. The present study followed this clinical method to improve the tongue position along with certain tongue exercises [2].
The study revealed that, the sub classification between upper and lower positions did not seem to have any practical significance and the interventional method employed for the subjects with retracted tongue position, played a significant role in assuming normal resting tongue position and also showed improvement in their mandibular complete denture stability. Patients with retracted tongue position alter the dimensions of the sublingual space and disrupt the mandibular denture peripheral seal that is needed for optimal denture retention [18-20]. Careful evaluation of resting tongue position in all patients who wear dentures helps to create future denture retention and stability [19,20]. Hence, during the examination and diagnostic phase of treatment, the tongue must be considered not only as an entity in itself but also as it will relate to a planned complete denture [1,13,14,18-20].
Limitation
The sample size was small to represent the study population which was the limitation of this study, even though the findings help to take appropriate decision and thus, this study becomes base for conducting some more trials taking large sample size.
Conclusion
Long term completely edentulous subjects presented retracted tongue position in the high percentage when compared to the recently extracted completely edentulous subjects. The interventional method employed for the subjects with retracted tongue position, played a significant role to assume normal resting tongue position, also showed improvement in their mandibular complete denture stability.