Surgical Management of a Rare Case of Massive Compound Odontome Associated with Missing Primary Tooth
Elengkumaran Sankaran1, Sangeetha Narasimhan2, KS Sabitha3, Punit Chitlangia4
1 Reader, Department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, Sri Ramachandra University, Porur, Tamil Nadu, India.
2 Lecturer, Department of Oral and Craniofacial Health Sciences, College of Dental Medicine, University of Sharjah, Sharjah-U.A.E.
3 Professor and Head, Department of Oncology, Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka, India.
4 Reader, Department of Oral and Maxillofacial Surgery, Mahatma Gandhi Dental College and Hostipal, Jaipur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sangeetha Narasimhan, M28-211, Department of Oral and Craniofacial Health Sciences, College of Dental Medicine, University of Sharjah, Sharjah-U.A.E.
E-mail: sangeetha_narashiman@yahoo.co.in
Odontomes are considered to be the most common odontogenic tumours of the jaws. They are benign, mixed tumours arising from the remnants of both odontogenic epithelium and the ectomesenchyme resulting in the deposition of varied propotions of enamel, dentin, cementum and pulp tissues. As these lesions show deficiency only in structural arrangement, some authors consider odontomes as hamartomas or tumour like malformations. Though these lesions are more common in children, very few cases have been reported in less than five years age group. Blood loss is a major issue in paediatric surgery. Careful and safe surgery is the primary goal of the surgeon. The external carorid artery which is the only feeder of blood to the face and oral cavity can be ligated to control bleeding in extensive maxillofacial injuries and orofacial malignancies. Herewith, we report a massive odontome in a three and half-year-old child which was treated by surgical excision along with carotid control to prevent excess bleeding.
Children, External carotid artery ligation, Odontogenic tumour
Case Report
A three and half-year-old female child reported to the Department of Oral and Maxillofacial Surgery with a chief complaint of slow growing asymptomatic swelling on the left side of the face for the past one year. On examination, a diffuse swelling measuring 3x3 cm extending anteroposteriorly from the corner of the mouth to 1 cm anterior to the tragus of the ear and superioinferiorly from infraorbital rim to the lower border of the mandible was noted. [Table/Fig-1]. The skin over the swelling was normal, the nasolabial fold was obliterated and the lower eyelid was pushed upward. On palpation the swelling was non tender and bony hard in consistency. Intraoral examination revealed a swelling in the left maxilla extending from canine to the tuberosity. The maxillary left lateral incisor was missing and the maxillary first and second primary molars were displaced but present within the tumour mass.
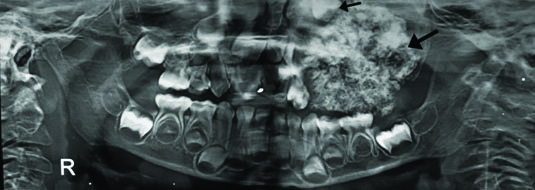
Orthopantomogram of the jaws showed a conglomerate mass of mixed radiodensity extending from the distal aspect of 63 to the maxillary tuberosity obliterating the left maxillary sinus. The upper first permanent molar was displaced and pushed up to the superior border of the sinus however the tooth follicles of the premolars were absent [Table/Fig-2]. A computed tomogram revealed mixed density lesion seen in the region of left maxilla with foci of calcifications occupying the maxillary sinus extending to the subcutaneous plane. However, no breach in cortex was noted in the medial aspect of the lesion. Impacted left upper first permanent molar was seen within the maxillary sinus [Table/Fig-3]. With a radiological differential diagnosis of fibrous dysplasia, odontome and odontoameloblastoma surgical excision was planned for the patient. Considering the age of the patient, in an aid to prevent excessive blood loss during the surgery, external carotid artery control was considered in addition to the excision.
Carotid Control
A shoulder bag was placed and the neck was extended. A 1.5 cm incision was placed to expose the carotid triangle, subplatysma flap was elevated and the sternocleidomastoid muscle was raised from the investing layer of deep cervical fascia. Posterior belly of digastric and superior belly of omohyoid were identified and raised. Carotid sheath was exposed to visualise internal jugular vein, vagus nerve and the common carotid artery. The common carotid artery was traced up to the bifurcation of internal carotid artery and external carotid artery. The external carotid artery was identified and confirmed. Superior thyroid artery and facial artery were identified and traced up to their main trunk from the external carotid artery. The hypoglossal nerve was preserved. After establishing clearance of vital structures the external carotid artery was tied with 3.0 vicryl to arrest bleeding [Table/Fig-4].
Primary Surgery
A Weber–Fergusson’s incision was made to establish maximum exposure to the tumour. Multiple teeth like structures with soft tissue were excised in toto [Table/Fig-5]. A surgical obturator was placed and the wound was closed. Postoperative recovery was uneventful [Table/Fig-6] and no recurrence was noted one year after surgery.
Histopathology
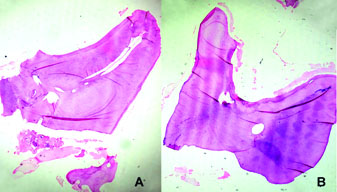
The excised lesional mass measured 7x7 cm in dimension; hard in consistency with an irregular surface containing multiple white areas admixed with reddish brown areas [Table/Fig-7]. The histopathology sections of the decalcified tumour bits showed multiple areas of enamel spaces, dentin, pulp and cemental tissues that resembled miniature tooth structures [Table/Fig-8].
Image showing the patient with a diffuse swelling on the left side of the face.

Orthopantomogram depicting mixed radiolucent and radio-opaque lesion of the left maxilla obliterating the maxillary sinus.
Computed tomographic image of the patient depicting mixed density lesion along with foci of calcifications.
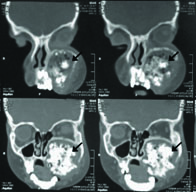
Image showing the ligation of the left external carotid artery.

Intraoperative image showing the large tumour mass.
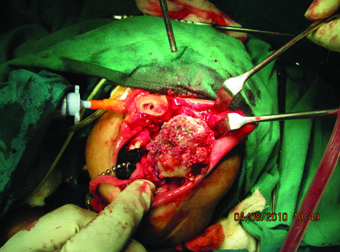
Image showing the postoperative extraoral view of the patient after a week.

Image showing the excised tumour mass consisting of a conglomerate of dental hard tissues.

A and B-Photomicrograph showing the histopathology section of the surgical specimen depicting tooth like structures (H and E 20X).
Discussion
Odontomes are defined as “tumours formed by the overgrowth of transitory or complete dental tissues” [1]. Odontomes account to about 22% of all the odontogenic tumours and can either be solitary or multiple in number [2,3]. The aetiology of these lesions is unknown. However, trauma, infection and loss in genetic control of tooth development have been quoted as possible causative factors [1,2,4]. Their association with syndromes like gardner’s syndrome, hermann’s syndrome and basal cell nevoid syndrome prove its genetic predisposition [5].
Odontomes manifest as asymptomatic swellings and are usually smaller than the size of the normal tooth [2,5]. Our case exhibited a massive swelling causing the expansion of the maxillary cortex which is very unusual.
Odontomes are associated with impacted teeth and at times missing tooth [2]. In our case the primary left lateral incisor and the permanent premolars were missing. The first permanent molar was impacted. The probable origin of this lesion could be attributed to the tooth germs which were missing in this patient. A large odontome in this case might have resulted due to uncontrolled proliferation of the terminally differentiated ameloblasts, odontoblasts and cementoblasts thereby secreting enamel, dentin and cementum, due to loss of genetic control in the alignment of the these hard tissues as proposed by Iatrou I et al., [5].
Odontomes are usually intrabony lesions, but occasional cases in the gingiva have been reported in the literature [5]. Compound odontomes are common in the anterior maxilla and complex odontomes are prevalent in the posterior part of the jaws [6]. Occasionally, odontomes erupt into the oral cavity like normal teeth. So far about 22 cases of erupted odontomes have been reported in literature [7,8]. Our case was peculiar that it involved almost the entire left quadrant of the maxilla with multiple teeth like structures embedded within.
Based on their structural composition and arrangement, odontomes are classified into compound and complex odontomes. A compound odontome results when the dental hard tissues deposition is in such a way that they anatomically resemble the normal tooth structure. The compound odontomes are in turn classified into three types namely denticular type, particular type and conglomerate masses. When the tissues are not arranged in an orderly fashion a complex odontome results. Some authors also suggest that odontomes are a type of supernumerary teeth [1,3]. The surgical specimen of our case showed multiple miniature teeth like structures favoring the diagnosis of compound odontome which in turn was confirmed by the histopathological examination of the same.
The differential diagnosis of odontomes includes odontoameloblastoma, ameloblastic fibroma and fibro-odontomas [5]. The absence of ameloblastic islands and marked fibrous connective tissue parenchyma in the histopathology ruled out the possible diagnosis of these lesions.
Blood supply to the head and neck is obtained from the left and right external carorid artery which is the branch of the common carotid artery. Carotid control has been practiced to prevent excessive bleeding during orofacial surgeries. Slooping of external carotid artery on the left side facilitated reduced blood supply and thus reduced blood loss during the surgery. This procedure is considered safe as it does not result in ischemia to the head and neck tissues [9,10]. Carotid control attempted in a very young patient for the excision of a massive odontome is the first of its kind and extensive literature survey has not shown any such attempt in the past for treating such a lesion.
Conclusion
Though odontomes are benign tumours occurring in the second decade of life, the dentist should be aware that they can occur in very small children and can grow to very large size. Extensive surgeries and severe morbidity in such patients can be avoided by early diagnosis of these lesions. Dental professionals should be aware that rarely odontomes can erupt into the oral cavity like normal tooth. Reporting such a case is to throw light to the surgeons that practicing carotid control during extensive oral and maxillofacial surgeries could prevent unnecessary blood loss in children.
[1]. P Zoremchhing, TB Joseph, BC Varma, JD Mungara, A compound composite odontome associated with unerupted permanent incisor – A case reportJ Indian Soc Prev Dent 2004 22(3):114-17. [Google Scholar]
[2]. UM Das, D Vishwanath, U Azher, A compound composite odontoma associated with unerupted permanent incisor – A case reportInt J Clin Pediatr Dent 2009 2(2):50-55. [Google Scholar]
[3]. G Yildirim-Oz, G Tosun, D Kiziloglu, E Durmus, Y Sener, An unusual association of odontomas with primary teethEur J Dent. 2007 1(1):45-49. [Google Scholar]
[4]. WG Shafer, MK Hine, BM Levy, A Textbook of Oral Pathology 1974 7th EditionPhiladelphiaSaunders:292 [Google Scholar]
[5]. I Iatrou, E Vardas, N Theologie-Lygidakis, M Leventis, A retrospective analysis of the characteristics, treatment and follow-up of 26 odontomas in Greek childrenJ Oral Sci 2010 52(3):439-47. [Google Scholar]
[6]. AR Peter, PP Hans, Odontogenic tumours and allied lesions 2003 1st EditionLondonQuintessence:143 [Google Scholar]
[7]. SB Sarojini, E Khosla, T Varghese, LJ Arakkal, Eruption of odontomas into the oral cavity: A report of @ casesCase reports in Dentistry 2014 :1-4. [Google Scholar]
[8]. C Bereket, N Cakir-Ozkan, I Sener, E Bulut, M Tek, Complex and compound odontomas: analysis of 69 cases and a rare case of erupted compound odontomaNiger J Clin Pract 2015 18:726-30. [Google Scholar]
[9]. T Kumar, V Yadav, K Ravi, K Ramaswamy, MH Patel, K Kothari, External carotid artery ligation in squamous cell carcinoma of the oral cavity and oropharynx: An oncological emergencyIndian J of surg 2015 77(3):850-52. [Google Scholar]
[10]. MM Nasr, Bilateral external carotid artery ligation: A life saving procedure in severe maxillofacial traumaInt J Surg Case Rep 2015 8:81-83. [Google Scholar]