Prosthetic rehabilitation of endodontically treated teeth has been a challenge to dental practitioners. Following endodontic therapy, substantial amount of tooth structure is lost due to caries, trauma and endodontic procedures and it becomes a hollow calcified laminated structure with deficient collagen cross linking and reduced modulus of resiliency with increased fracture susceptibility. Survival of such teeth is directly related to the quality as well as quantity of the remaining tooth structure [1]. Conservation of sound coronal dentin permits placement of margin on remaining tooth structure which influences the fracture resistance of crowned endodontically treated teeth [2]. Reinforcement of fiber posts in endodontically treated teeth with insufficient coronal tooth structure produces a stress field similar to that of natural teeth because of same elastic modulus as that of dentine, thus restoring the tooth to function [3].
Incorporation of a ferrule when restoring an endodontically treated tooth with a post-core and a crown always enhance the prognosis of the tooth. A ferrule has been defined as a circumferential metal collar of the crown surrounding the parallel walls of the dentine extending coronal to the margin of the preparation [4]. The ferrule improves biomechanical stability of the tooth by improving resistance to dynamic occlusal loading and integrity of the cement seal of the prosthesis. Studies have validated the use of atleast 1.5 mm ferrule as most effective in resisting fracture under load [5-7]. Many studies investigating the ferrule effect have used cast post and core and generally on anterior teeth [8-12], but there is little information as to whether ferrule length has an added advantage along with fiber post and composite core in premolar tooth.
Therefore, the aim of this study was to evaluate and compare the effect of ferrule length on fracture resistance of endodontically treated mandibular premolar teeth restored with prefabricated glass fiber post luted with resin cement, composite core and a full coverage metal crown.
Materials and Methods
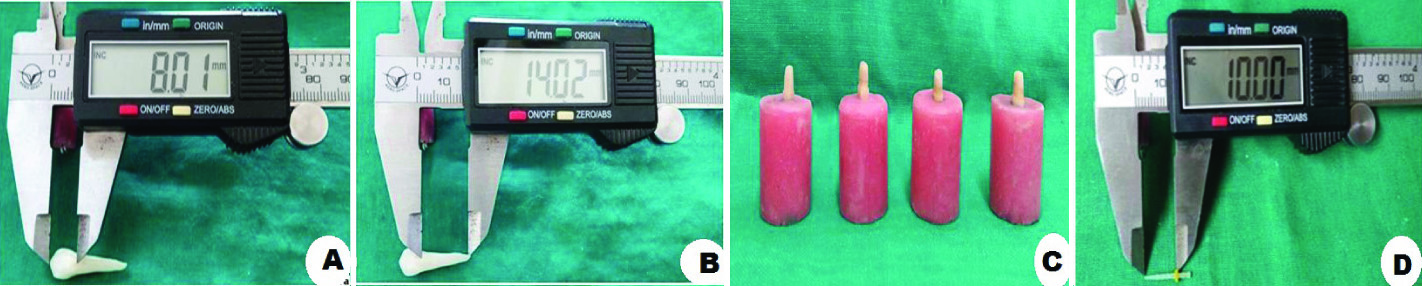
The present in vitro study was conducted in Department of Prosthodontics, Saraswati Dental College and Hospital, Lucknow, Uttar Pradesh, India in collaboration with Central Institute of Plastic Engineering and Technology, Lucknow. Forty extracted, human permanent mandibular premolars of approximately same dimensions were selected for the study which was measured using an electronic digital Vernier’s calliper (Mitutoyo/Digimatic, Japan) to make sure that they satisfy the following inclusion criterias: Mesio-Distal (M-D) dimensions: 5 mm±1, Bucco-Lingual (B-L) dimensions: 7 mm±1, root length atleast 15 mm [Table/Fig-1a,b]. Additionally, periapical B-L and M-D radiographic views were taken to ensure the presence of straight, single canal orifice, and completely formed apices. The teeth were inspected to exclude any defects or cracks, restorations or caries and previous endodontic restorations. Disinfection of the specimens was done using 0.5% chloramine T aqueous solution at 4°C for one week. Subsequently the selected teeth were stored in normal saline throughout the procedure to prevent desiccation.
a) Dimension of crown measured using an electronic digital Vernier’s caliper; b) Dimension of root measured using an electronic digital Vernier’s caliper; c) Specimens mounted into resin filled moulds; d) Length of the post (standardized) using an electronic digital Vernier’s caliper.
A reference line was marked with graphite pencil at the Cemento-Enamel Junction (CEJ) of the experimental group specimens. The marking was based on digital vernier calliper measurements. Sectioning the coronal tooth structure, at the reference lines, was done perpendicular to the long axis of the teeth using a diamond disc with low speed straight handpiece. The resultant coronal tooth surface was flat, rather than following the undulations of the CEJ under constant water irrigation. To standardize the specimen’s length, the crowns of the selected teeth were removed according to ferrule heights; Group A: no ferrule; Group B: 1 mm ferrule; Group C: 2 mm ferrule; Group D: 3 mm ferrule.
Standardized endodontic procedure was carried out on all specimens using Protaper® (Dentsply Maillefer, Ballaigues), canals were irrigated with 3% NaOCl and obturated with F2 ProTaper guttapercha cones (Dentsply Maillefer, Ballaigues) using AH Plus Sealer (Dentsply Maillefer, Switzerland). Finally to ensure full setting of the seal, the teeth were stored in a 100% humid environment at 37°C for 24 hours.
Guttapercha removal was performed with Gates Glidden drills (3#) taking care to preserve 4 mm apical seal. Radiographs were taken to evaluate the adequacy of the remaining dentine structure around the post space preparation. For standardized orientation of all specimens into resin filled moulds, dental surveyor was used [Table/Fig-1c]. Root surfaces were marked 3 mm below the CEJ. To simulate the periodontal ligament, the root surfaces were covered with two layers of 0.075 mm thick heat-resistant polytetrafluoroethylene adhesive tape and coated with petroleum jelly. Silicone impression material (Alphasil®, Germany) was mixed and injected around tooth to produce a standardized silicone layer of 0.15 mm to simulate periodontal ligament.
Prefabricated glass fiber post (Reforpost, Angelus) of 0.9 mm diameter at their apical section and 1.3 mm diameter at their coronal section were selected for the study [Table/Fig-1d]. The dual-cure resin cement RelyXTM U200 was used for post cementation. The specimens were left undisturbed for 15 minutes prior to storage in 100% humidity environment at 37°C for 24 hours. Composite resin (for core build up) was placed in increments with 40 seconds of polymerization. Standardized preparation was done in each specimen using a high speed rotary handpiece [Table/Fig-2a]. Crowns were luted with glass ionomer cement.
a) Tooth was prepared using a high speed rotary handpiece mounted in a dental surveyor; b) Specimen placed on UTM (Instron 3382) for loading.
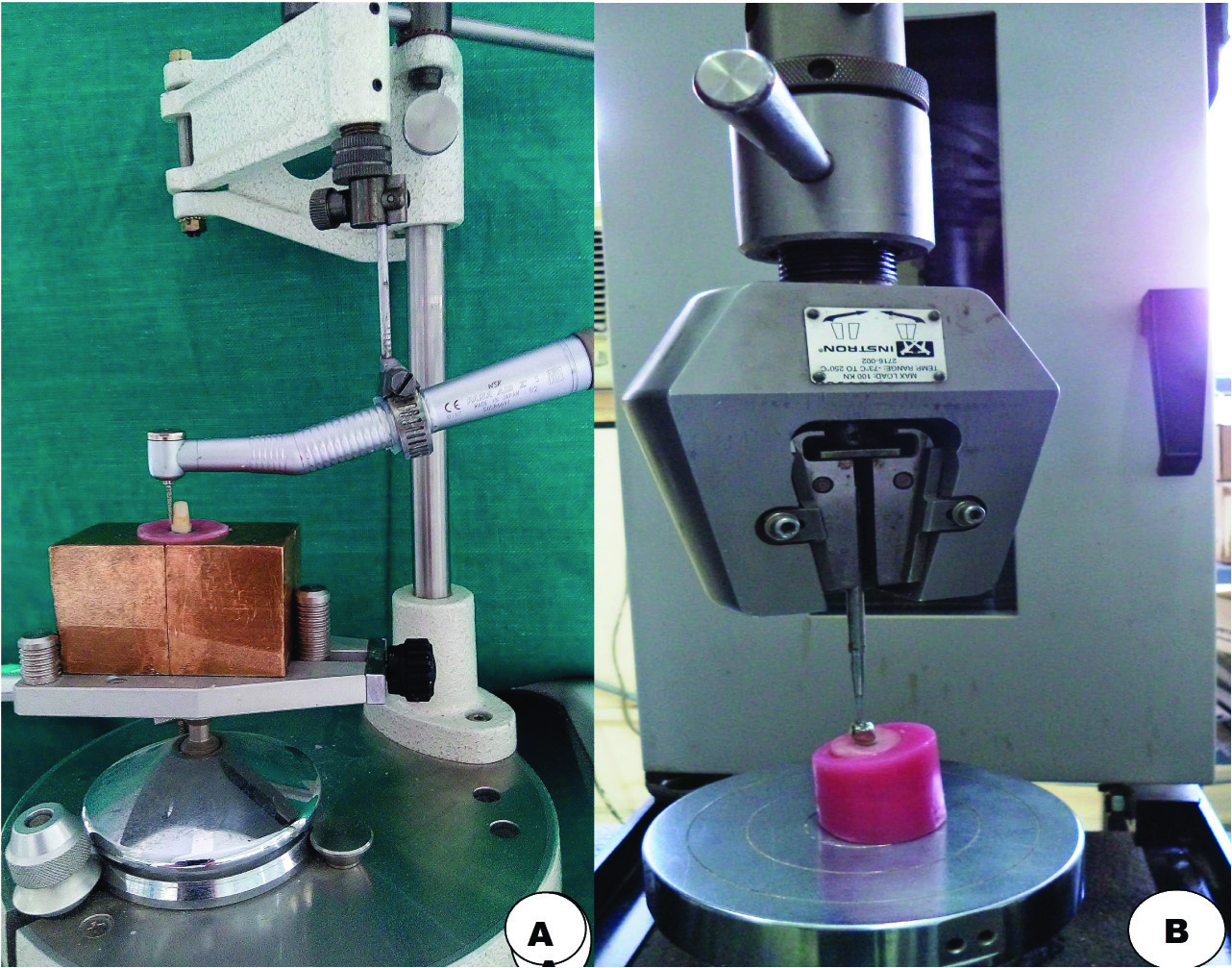
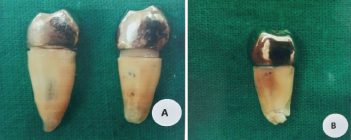
Distilled water was selected to store the specimens at a temperature of 37°C with 100% humidity for 24 hours. Subsequently the specimens were thermocycled for 500 times from 5° to 55°C using 30 second dwell times. The mounted specimens were aligned with the long axis of the tooth at 30° to the loading rod tip. This jig was secured to the lower compartment of a Universal Testing Machine (UTM) (Instron 3382). A flat steel tip with compressive head was used to apply the load on lingual incline of buccal cusp. It was fixed to the moving upper compartment of the testing machine [Table/Fig-2b]. The compressive load was applied at a crosshead speed of 1 mm/min until failure occurred. The failure mode was evaluated by visual examination of the specimens to classify its type [13]. Then a stereomicroscope (Olympus, U-CMAD3, Japan) was used for further evaluation of the mode of failure. The failure mode was classified as either favourable (restorable) or unfavourable (catastrophic) [Table/Fig-3a,b]. Favourable failure modes are those that take place above the level of acrylic resin which simulate the bone level. They include either partial or complete post-core-crown debonding or post-core-tooth complex fracture above acrylic resin block. Unfavourable failure occurs below the level of the acrylic resin. It includes fracture of the post-core-root complex, cracks in the roots or vertical root fractures.
a) Favourable fracture; b) Unfavourable fracture.
Statistical Analysis
The data was analysed using Statistical Package for Social Sciences, version 15.0, distributions were checked for normality using Kolmogorov Smirnov test and failure mode was recorded and statistically analysed with Kruskal Wallis test.
Results
The mean value of fracture resistance, standard deviation and intergroup comparison was recorded and statistically analysed using Kruskal Wallis test [Table/Fig-4]. The specimens (n=40) had a mean fracture resistance of (766.21±204.91 N) with values ranging from a minimum of 364.66 N to a maximum of 1253.67 N. Fracture resistance was found to be lowest for Group A (529.36±119.95 N) followed by Group B (714.64±133.89 N), Group C (848.84±109.60 N) and highest for Group D (971.99±133.07 N) [Table/Fig-4]. Difference in fracture resistance values among the groups was found to be statistically significant (p<0.001).
Inter groups comparison of compressive load (Kruskal Wallis test: Non-Parametric ANOVA).
| Group | No. of specimens | Minimum(Newton) | Maximum(Newton) | Mean(Newton) | S.D. | Median | Mean Rank | Statistical significance |
|---|
| H | p |
|---|
| Group A | 10 | 364.66 | 698.40 | 529.36 | 119.95 | 522.16 | 7.20 | 25.665 | <0.001 |
| Group B | 10 | 594.77 | 984.67 | 714.64 | 133.89 | 658.23 | 16.80 |
| Group C | 10 | 693.00 | 1018.14 | 848.84 | 109.60 | 810.01 | 26.20 |
| Group D | 10 | 854.74 | 1253.67 | 971.99 | 133.07 | 925.39 | 31.80 |
| Total | 40 | 364.66 | 1253.67 | 766.21 | 204.91 | 767.58 | | | |
Though fracture was found to be favourable in higher proportion of Group D (90.0%) as compared to Group B (80.0%), Group C (80.0%) and Group A (70.0%) [Table/Fig-5], they were not statistically significant.
Favourability of fracture among the groups.
| Group A(n = 10) | Group B(n = 10) | Group C(n = 10) | Group D(n = 10) |
|---|
| No. | % | No. | % | No. | % | No. | % |
|---|
| Favourable | 7 | 70.0 | 8 | 80.0 | 8 | 80.0 | 9 | 90.0 |
| Unfavourable | 3 | 30.0 | 2 | 20.0 | 2 | 20.0 | 1 | 10.0 |
Discussion
Advancements in the field of restorative dentistry have markedly increased the probabilities of successful restoration of severely damaged endodontically treated teeth. The preservation of tooth structure in endodontically treated tooth improves its prognosis because it provides protection against fracture under occlusal loads. A ferrule, in respect to the teeth, is a band that encircles the external dimension of residual tooth structure.
In the present study, influence of ferrule length on fracture resistance and failure pattern of endodontically treated crowned mandibular premolars reinforced with composite core and fiber post was investigated. The decision to place a post in endodontically treated tooth depends upon amount of loss of tooth structure and also the amount of functional forces on tooth [14,15]. Many investigators have reported that post placement affects fracture resistance and increases the potential risk of root fracture and root fracture was reported with the use of metallic posts [16,17]. Fiber posts were investigated to have modulus of elasticity which was similar to that of dentine, and thus producing a stress field similar to that of natural teeth. It was thought that fiber posts lowered the interfacial stress and reduced the chances of failure [18]. Since the physiological properties of a periodontal ligament in teeth under load potentially affects the results, periodontal ligament simulation was done to be as close as possible to the clinical situation. To mimic the clinical oral conditions mandibular premolars were stored in normal saline at 37°C and they were loaded at an angle in UTM which corresponded to the loading angulation of mandibular premolar in natural dentition.
In the present study, the fracture resistance of teeth was tested under static load to stimulate forceful clenching. The results confirmed that the endodontically treated teeth with the presence of a ferrule had superior fracture resistance under a static load than those that lacked ferrule and increasing the ferrule length significantly increased the fracture resistance of endodontically treated teeth restored with glass fiber posts, composite cores and crowns (p<0.001). In another study, Sorensen JA and Martinoff JT showed that 1 mm of remaining coronal tooth structure nearly doubled the fracture resistance of the endodontically treated teeth [19].
The results of the present study are in agreement with other studies [20,21]. The lowest mean failure load recorded from the subgroup having no ferrule was 529.36 N.
Additionally, the results indicated that the 3 mm ferrule length group presented significantly highest mean failure load (971.99 N) when compared with the 2 mm (848.84 N), 1 mm ferrule (714.64 N) and 0 mm (529.36 N) ferrule group. These variations of failure load between different ferrule height groups may be attributed to several mechanisms of action as explained by Tan PL et al., [22]. The most reasonable explanation was that the amount of remaining coronal dentin provided a more stable foundation which helps to redistribute and dissipate the applied forces. Subsequently, greater resistance to rotation was achieved and fracture resistance of endodontically treated tooth increased. Our results disagree with the study done by Al-Hazaimeh and Gutteridge DL [23]. They used prefabricated metal post (parapost) which were cemented with Panavia-ex and restored with a composite core and studied the effect of 2 mm of ferrule preparation on the fracture resistance of crowned central incisors. They concluded that the additional increase in ferrule heights has no benefit in terms of resistance to fracture. One explanation might be due to the fact that they evaluated the effect of different ferrule designs and configurations but at the same length. While in this study, effects of different ferrule lengths in the same design were evaluated. Though the fracture was found to be favourable in higher proportion of Group D (90.0%) as compared to Group B, Group C (80.0% each) and Group A (70.0%) but this difference was not found to be significant.
Although the design of the current study attempted to simulate clinical situations such as ferrule preparation, periodontal ligament and cast crown, it is difficult to implement these results directly for the clinical practice because it is an in vitro study which could not fully replicate oral conditions. Besides the type of test used, that is, a static load which does not represent the oral condition. The study also evaluated the mandibular premolar and therefore, the results can be applied only to that group of teeth.
Conclusion
Under the limitation of this study, the following conclusions were drawn: Increasing the ferrule length can significantly increase the fracture resistance of the endodontically treated mandibular premolars restored with a glass fibre post luted with RelyX™ U200 self adhesive resin cement, composite core and metal crown. All the intergroup differences, except between Group C and Group D were statistically significant. The following order of fracture resistance was observed among the different groups: Group A< Group B < Group C < Group D. Almost all the subgroups had favourable type of failures.