Introduction of dental implants for replacement of missing tooth changed the phase of prosthetic dentistry, where a missing tooth can receive a restoration more analogous to natural tooth without the hassle of crown and bridge. Implants are becoming a predictable alternative for routine replacements in edentulism. Beginning of the era of implant prosthesis, two stage procedures were followed with waiting period of three to six months from implant insertion to loading. Meanwhile, patients had to deal with functional concerns until osseointegration and the fabrication of a new prosthesis. Not only the functional concerns, but also the psychosocial impact of missing teeth can be overwhelming to patients [1].
Over the time, with improved manufacturing technology, understanding of the healing cascade changed the concept of delayed to immediate loading. In recent years, immediate loading of implants became a reality, not only in a partially edentulous patient but also in completely edentulous patient. Immediate loading with provisional restoration shortens the time to return to function, that result in a definitive restorative solution immediately following surgery [1]. So, the study was aimed to evaluate and compare the clinical outcome of immediate and delayed loading of implant supported prosthesis for the replacement of missing mandibular first molar. The evaluation was carried out using following observations; bleeding on probing, probing depth, implant mobility, marginal bone level and peri-implant radiolucency.
Materials and Methods
The randomized prospective study was carried out at the Department of Oral and Maxillofacial surgery, Sibar Institute of Dental Sciences, Andhra Pradesh, India and our Advanced Dental Care Centre during the year December 2009-November 2016. Twenty patients who were in the need of implant supported prosthesis for missing mandibular first molar with good oral hygiene and willing to participate in the study protocol were included over a period of one year from December 2009. The progressive sampling was considered with 95% confidence level for statistical significance. The edentulous sites for implant insertion were grouped into two after randomization using computer generated random table numbers. In Group I- implants were loaded immediately (within two days) after implant insertion and Group II- implants were loaded after three months of implant insertion. The procedure was explained, followed by informed written consent according to the Declaration of Helsinki. All the implants were evaluated clinically and radiographically immediately after insertion and during follow up visits at 6th, 12th, 36th and 72nd months after loading. The study was approved by the Institutional Ethics Committee with a number- IEC/2009-8.
Inclusion and Exclusion criteria for Patient Selection
The patients having edentulous space in the region of the mandibular first molar with sufficient bone quality and quantity (>5 mm width buccolingually, minimum of 10 mm of space anterio-posteriorly and >12 mm of height) reluctance to have a removable or fixed partial denture with a history of extraction not less than three months before planning for implantation were included in the study. The patients with systemic conditions (American Society of Anaesthesiology Class III and IV) [2] that could place the patient at risk during minor oral surgical procedure, drug and alcohol abuse, current or past sessions of radiation therapy in the head and neck region, association of psychological problems and habits like bruxism, smoking and tobacco chewing were excluded from the study.
Preoperative Evaluation
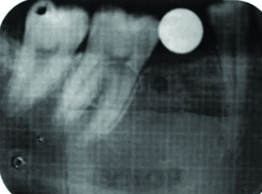
Patients were evaluated following a thorough history, clinical [Table/Fig-1,2] and radiographic assessment with routine blood investigations. The intra-arch relationship was evaluated using diagnostic casts. Standardized Intra Oral Periapical Radiographs (IOPA) was taken to assess bone architecture and surrounding structures. Distortion factor for panoramic radiograph and IOPA were assessed using a steel ball of 6 mm diameter placed at predetermined implant location [Table/Fig-3]. The available bone height above the mandibular canal was evaluated for selection of the implant. Ridge mapping was done using bone calipers to determine the alveolar ridge width for the selection of implant diameter. An individualized acrylic resin surgical guide was fabricated for each patient to obtain an ideal position for implant placement. After initial planning, all patients underwent oral prophylaxis and received oral hygiene instructions.
Preoperative oral clinical photo showing interocclusal space while tooth in occlusion and edentulous area-Group I.

Preoperative oral clinical photo showing interocclusal space while tooth in occlusion and edentulous area-Group II.

Preoperative radiograph showing evaluation of magnification error with metal ball in place-Group I;
Surgical Procedure
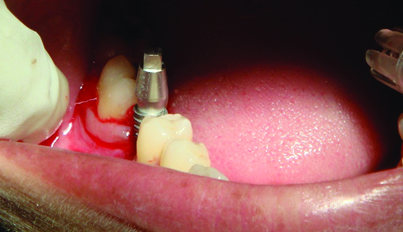
Standard operating procedures were followed during surgery. Soft tissue was removed from the crest using biopsy punch under local anaesthesia (2% lignocaine with 1:80,000 adrenaline) in Group-I and a crestal incision was given, followed by complete mucoperiosteal flap reflection. In Group-II point of entry was gained through the guiding hole made in the surgical guide using a round bur. These implants bed preparation were done with a standard pilot drill under copious internal and external irrigation with chilled saline as per the manufacturer’s instructions. Paralleling tool was used to check the angulation of the osteotomy. Standard drills were used for sequential drilling. The pre selected implants were threaded using a ratchet into the prepared site in both groups [Table/Fig-4] and in Group-II cover screw placed after removal of the implant mount with the help of hex tool [Table/Fig-5].
Intraoperative photo showing implant insertion-Group I;
Intraoperative photo showing implant insertion and cover screw in place-Group II.

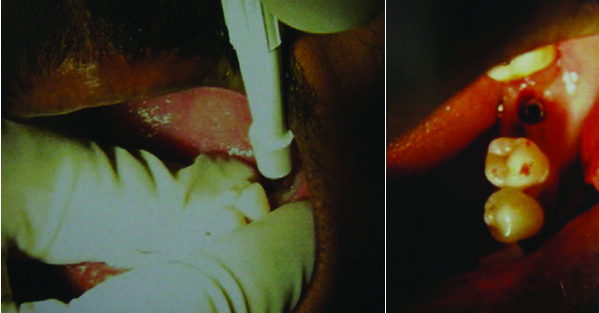
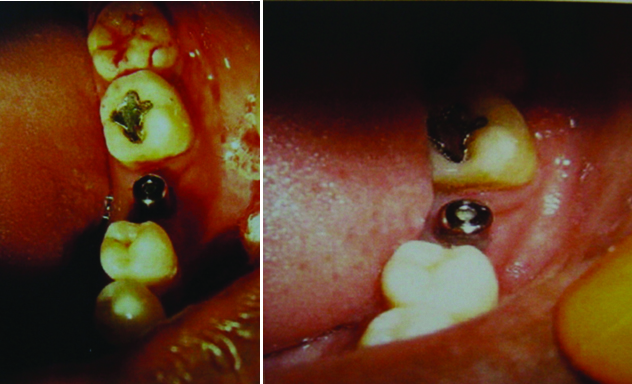
After the placement of implant with adequate stability, in Group I (single piece implant with abutment); which were left in place undisturbed until the prosthetic procedure. All implants had internal hex with length ranging from 10 mm to 13 mm and diameter 3.3 mm to 4.5 mm. Incision was closed using 3-0 mersilk suture, recalled after seven days for suture removal. In Group-I, acrylic provisional crown prosthesis was given within 48 hours of implant placement [Table/Fig-6] and was replaced by metal-ceramic single crown prosthesis after three months. In Group II, second stage surgical procedure was performed after three months of implant insertion. The implant was exposed using a biopsy punch and the cover screw removed [Table/Fig-7] for placement of healing caps [Table/Fig-8]. Two weeks after healing abutment placement, implant was restored with metal-ceramic single crown [Table/Fig-9].
Showing provisional crown placement with occluded teeth and from occlusal view-Group I;

Intraoperative photo showing use of punch to uncover implant with exposed implant-Group II.
Intraoperative photo showing placement of healing cap and gingival healing after two weeks-Group II;
Intra oral photo showing permanent crown placement with occluded teeth-Group II.

Patients were assessed for implant mobility, marginal bone level, peri-implant radiolucency, bleeding on probing and also probing depth at first and six months after loading and later at 12th, 36th and 72nd months time interval [Table/Fig-10,11]. The mobility of implant was assessed using Periotest (PT) after six months. The standard William’s periodontal probe was used to assess bleeding on probing and probing depth. The bleeding on probing was assessed at three different positions by walking the probe into the crevice at mesial, distal line angle and middle area of implant.
Radiograph immediately and at 6th,12th,36th,72nd months after implant insertion-Group I;

Radiograph immediately and at 6th,12th,36th,72nd months after implant insertion-Group II.

For all the patients antibiotics (Cap Amoxicillin 500 mg TID for five days) and anti-inflammatory medication (Tab Diclofenac BID for three days) was prescribed. Patients were instructed to use chlorhexidine mouthwash twice daily for four weeks and were reviewed on regular basis. Standardized IOPA radiographs were taken to assess the marginal bone levels and peri-implant radiolucency.
The follow up observations were done by a periodontist who was blinded for the follow up durations in both groups. The standardized IOPA were provided for assessment of bone level. The observations were tabulated separately. If any significant variation existed then one more periodontist examined the radiographs to prevent inter observer bias.
Statistical Analysis
The results were tabulated using the Microsoft Excel and statistical analysis was carried out using SPSS (statistical package for social sciences) version 20.0. Wilcoxon matched pairs test, Mann-Whitney U test, Mean±SD and p-values were considered for comparison with p<0.05 considered as significant. The kappa correlation was taken into consideration to assess the degree of observer agreement for radiological assessment.
Results
The study consists of 14 (70%) male and 6 (30%) female patients with the age range of 19 to 31 years, and mean 23.1 years. The diameter of implants in Group I- ranged from 3.5 mm to 4.5 mm with a mean of 4.34 mm; whereas, in Group II ranged from 3.3 mm to 4.2 mm with a mean of 3.98 mm. The length of implants in Group I and II ranged from 10 mm to 13 mm with a mean of 11.65 mm.
None of the patients showed bleeding on probing except in one patient because of loose abutment, which stopped after tightening of the abutment. [Table/Fig-12]. Probing depth was within the normal range (1 mm to 3 mm) for all patients after 1st, 6th, 12th, 36th, and, 72nd months after loading [Table/Fig-13]. Mean value of probing depth after one month of loading in Group-I was 1.8±0.63 mm and after six months 1.2±0.42 mm which was statistically significant; whereas, in Group-II, 1.8±0.42 mm and remained 1.8±0.42 mm even at the end of last follow up was statistically not significant between the groups.
Comparison of bleeding on probing in immediate and delayed loaded implants after crown cementation by Mann-Whitney U test.
| Crowncementation | Groups | Mean | SD | U-value | Z-value | p-value |
|---|
| After 1st month | Immediate loading | 0.20 | 0.42 | 50.00 | 0.00 | 1.00 |
| Delayed loading | 0.20 | 0.42 | | | |
| After 6th month | Immediate loading | 0.00 | 0.00 | 50.00 | 0.00 | 1.00 |
| Delayed loading | 0.00 | 0.00 | | | |
| After 12th month | Immediate loading | 0.00 | 0.00 | 50.00 | 0.00 | 1.00 |
| Delayed loading | 0.00 | 0.00 | | | |
| After 36 month | Immediate loading | 0.00 | 0.00 | 50.00 | 0.00 | 1.00 |
| Delayed loading | 0.00 | 0.00 | | | |
| After 72 month | Immediate loading | 0.00 | 0.00 | 50.00 | 0.00 | 1.00 |
| Delayed loading | 0.00 | 0.00 | | | |
Comparison of probing depth after crown cementation of immediate and delayed loaded implant groups by Wilcoxon matched pairs test.
| Group | Time | Mean | Std.Dv. | Diff. | Diff. | U-value | Z-value | p-value |
|---|
| Immediate loading | 1st month | 1.80 | 0.6325 | 0.60 | 0.5164 | 0.00 | 2.2014 | 0.0277* |
| 6th month | 1.20 | 0.4216 |
| Delayed loading | 1st month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 6th month | 1.80 | 0.4216 |
| Immediate loading | 6th month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 12th month | 1.80 | 0.4216 |
| Delayed loading | 6th month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 12th month | 1.80 | 0.4216 |
| Immediate loading | 12th month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 36th month | 1.80 | 0.4216 |
| Delayed loading | 12th month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 36th month | 1.80 | 0.4216 |
| Immediate loading | 36th month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 72 month | 1.80 | 0.4216 |
| Delayed loading | 36th month | 1.80 | 0.4216 | 0.00 | 0.6667 | 5.00 | 0.00 | 1.00 |
| 72 month | 1.80 | 0.4216 |
*p<0.05-significant
Mobility was not seen throughout the follow up period and the PT values [Table/Fig-14] ranged from 0 to -4, with a mean value of -1.8 and SD of 1.2293 for Group-I, and 0 to -3 with a mean value of -1.6 and SD of 1.075 for Group-II [Table/Fig-15].
Implant mobility of immediate and delayed loaded implants according to clinical implant mobility scale at various stages.
| Intervals | Immediate loaded implants | Delayed loaded implants |
|---|
| Mobility Absent | Mobility Present | Mobility Absent | Mobility Present |
|---|
| At the time of implant placement | 10.00 | 0.00 | 10.00 | 0.00 |
| After 1st month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 6th month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 12th month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 36th month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 72nd month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
Comparison of implant mobility according to Periotest values of immediate and delayed loaded implants after six months of crown cementation by Mann-Whitney U test.
| Groups | Mean | SD | U-value | Z-value | p-value |
|---|
| Immediate Loading | -1.8000 | 1.2293 | 46.0000 | -0.3024 | 0.7624 |
| Delayed Loading | -1.6000 | 1.0750 | | | |
Marginal bone loss at the mesial and distal aspects were measured in both groups. The mean value of bone loss was 1.1 mm and 1.15 mm on mesial and distal aspects respectively, for Group I; whereas, 0.95 mm and 0.825 mm for Group II after one month of loading and 0.1 mm and 0.15 mm for Group I; whereas 0.15 mm and 0.15 mm for Group II after six months of loading [Table/Fig-16]. None of the implants (0%) showed peri-implant radiolucency during six months to six years of follow up period after loading the implant [Table/Fig-17].
Comparison of bone loss in mm in immediate and delayed loaded implants at mesial and distal sides by Mann-Whitney U test.
| Side | Groups | Mean | SD | U-value | Z-value | p-value |
|---|
| Mesial 6 months | Immediate loading | 1.1000 | 0.5676 | 45.5000 | -0.3402 | 0.7337 |
| Delayed loading | 0.9500 | 0.4972 | | | |
| Distal6 months | Immediate loading | 1.1500 | 0.4116 | 27.0000 | -1.7386 | 0.0821 |
| Delayed loading | 0.8250 | 0.3344 | | | |
| Mesial12 Months | Immediate loading | 0.1000 | 0.2108 | 45.0000 | -0.3780 | 0.7055 |
| Delayed loading | 0.1500 | 0.2415 | | | |
| Distal12 Months | Immediate loading | 0.1500 | 0.2415 | 46.5000 | -0.2646 | 0.7913 |
| Delayed loading | 0.1500 | 0.3375 | | | |
| Mesial36 Months | Immediate loading | 0.1000 | 0.2108 | 45.0000 | -0.3780 | 0.7055 |
| Delayed loading | 0.1500 | 0.2415 | | | |
| Distal36 Months | Immediate loading | 0.1500 | 0.2415 | 46.5000 | -0.2646 | 1.000 |
| Delayed loading | 0.1500 | 0.3375 | | | |
| Mesial72 Months | Immediate loading | 0.1500 | 0.2415 | 46.5000 | -0.2646 | 1.000 |
| Delayed loading | 0.1500 | 0.3375 | | | |
| Distal72 Months | Immediate loading | 0.1500 | 0.2415 | 46.5000 | -0.2646 | 1.000 |
| Delayed loading | 0.1500 | 0.3375 | | | |
Comparison of periimplant radiolucency of immediate and delayed loaded implants at various stages.
| Intervals | Immediate loaded implants | Delayed loaded implants |
|---|
| Absent | Present | Absent | Present |
|---|
| At the time of implant placement | 10.00 | 0.00 | 10.00 | 0.00 |
| After 1st month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 3rd month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 12th month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 36th month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
| After 72nd month of crown cementation | 10.00 | 0.00 | 10.00 | 0.00 |
Discussion
Mandibular first molar is the most common tooth being affected by dental caries and being lost due to its sequelae as it is the first permanent tooth to erupt and get exposed to the oral environment. Failure to replace a missing molar will cause the sequence of damages to stomatognathic system by affecting occlusion, arch form, gingival and periodontal health of surrounding teeth eventually leading to TMJ disorders. Branemark placed first dental implant with primary stability and a stress free healing period for successful osseointegration. This initial experience with dental implant leads to the two stage healing protocol that became the foundation for dental implantology [1].
Bleeding on probing is the most valid indicator of peri-implant breakdown. In the study of Salvi GE et al., bleeding on probing was observed in 9.7% and 8.3% in immediate and delayed loading groups, respectively with no statistical difference. Our study results are in accordance with the study done by Salvi GE et al [3]. None of the patients showed bleeding on probing after six months of crown cementation. But loosening of prosthesis in one patient in each group showed bleeding on probing after one month of loading which subsided after recementation of the crown. According to Jemt T et al., there is a positive correlation between bleeding on probing and histologic signs of inflammation at implant sites, indicating bleeding on probing may precede clinical signs of inflammation [4]. Bauman GR et al., determined that bleeding on probing occurred concurrently with other signs of implant failure, such as radiographic bone loss and increased probing depths [5].
Probing depth is a good indicator of peri-implant destruction. Degidi M et al., suggested probing depth and radiographic measurements together for a comprehensive assessment of implant success [6]. In the study conducted by Salvi GE et al., the mean probing depth after six months of crown placement was 2.6 mm and 2.7 mm for immediate and delayed loading group respectively with no statistical difference [3]. Heydenrijk K et al., found the decrease in mean probing depth in the immediate loading group after six months of crown placement to 3.3 mm, which was 3.6 mm at one month after crown placement. But no change was seen in the delayed loading group which remained 3.7 mm at both stages. In our study, the results showed similarity with the study done by Heydenrijk K et al., [7]. Decrease in mean probing depth in Group I was 1.8 mm at one month after crown placement; it was 1.2 mm after six months of crown placement which is statistically significant with p-value of 0.0277, the mean probing depth remained 1.8 mm for the delayed loading group at both stages. After one month of crown placement, there was no significant difference in probing depths between the groups. Our study results substantiates the hypothesis of Schincaglia GD et al., that positive effect of osteo deposition induced by mechanical strain in immediately loaded implants in comparison to conventional implants showed reduced probing depths and radiographic bone level changes [8].
Assessment of implant mobility is an important clinical parameter [2]. Lorenzoni M et al., reported 100% survival rate with no mobility after immediate loading [9]. Our study also showed 100% survival with no mobility. The PT values ranged from -8 to +50, and values above 20 are irrelevant in implantology. The smaller and negative PT values are generally good, which indicate the implant osseointegration [10]. Randow K et al., found the PT values of -3.9 in immediate loading group and -2.6 in the conventional group [11]. Our PT values were -1.8 and -1.6 for Group I and Group II, respectively, with no statistical significance and are in accordance with the above study.
Marginal bone loss assessment is an important criterion for evaluating implant success. Schincaglia GD et al., found bone loss of 0.77±0.38 mm in immediate loading and 1.2± 0.55 mm in delayed loading group. The average radiographic bone level change was correlated to the hypothesis that micromovements caused by immediate loading has a positive effect on osteo deposition [8], Vandamme K et al., showed significant increase of bone mineralization around implants loaded immediately when compared to unloaded implants in animal study [12]. Salvi GE et al., found the bone loss of 0.57±0.49 mm in immediate loading group and 0.72±0.50 mm in delayed loading group with no statistical significance between the two groups [3]. Kim JH et al., observed 0.29±0.19 mm the bone loss after six months of crown placement in immediately loaded implants [13].
The marginal bone loss of 1.1±0.56 mm and 1.15±0.41 mm seen at the mesial and distal aspects after one month of loading for Group I, and the mean value of bone loss was 0.95±0.49 mm and 0.82±0.33 mm on mesial and distal aspects respectively for Group II. After six months of loading, the Group I implants showed an average bone loss of 0.1±0.21 mm and 0.15±0.24 mm on mesial and distal aspects respectively, which are in accordance with the results of Kim JH et al., [13]. After six months of loading, the Group II implants showed an average bone loss of 0.15±0.24 mm and 0.15±0.33 mm on mesial and distal aspects respectively which correlates with the observations of Salvi GE et al., [3].
The comparison of bone loss at one and six month after loading in both groups showed a statistically significant result in this study. In Group I, the mean bone loss on mesial side improved from 1.1±0.56 mm to 0.1±0.21 mm at six months after loading with a p-value of 0.0051 and the mean bone loss on distal side improved from 1.15±0.41 mm to 0.15±0.24 mm at six months after loading with a p-value of 0.0051. In Group II, the mean bone loss of mesial side improved from 0.95±0.49 mm to 0.15±0.24 mm at six months after loading with a p-value of 0.0077 and the mean bone loss on distal side improved from 0.82±0.33 mm to 0.15±0.33 mm at six months after loading with a p-value of 0.0117 (p<0.05) which makes our study in accordance with the study of Hahn JA which showed improvement of bone level at follow up visits than at the time of placement [14].
The peri-implant radiolucency is defined as the radiographic evidence of progressive peri-implant bone loss. Degidi M et al., showed no peri-implant radiolucency in immediately loaded implants [6]. Our study, showed 100% survival rate after six and 72 months of loading with no peri-implant radiolucency.
All the implants placed for replacement of the mandibular first molar by immediate and delayed loading techniques, healed predictably in the present study. The results were obtained in a small sample size, but with six years of long term follow up; published literature shows only three and four years of follow up period [4,15]. So, our study suggests the further multi centric long term studies considering above mentioned factors for comparison.
Limitation
The implant used in this study was of different sizes. Size of implant also plays an important role in the success of the implant which was not considered in this study. The type of bone was not considered for success of implant analysis, which influences the long term success of the implant. The technique of flap and flapless placement plays an important role in crestal bone loss surrounding implant.
Conclusion
The single tooth implant restoration in mandibular first molar with immediate loading can be used as a successful treatment modality and as an alternative to the conventional delayed loading. Immediate loading reduces the time delay for functional rehabilitation. It prevents patient’s uneasiness and provides definitive prosthesis with early function. Our study showed 100% survival rate even after 72 months of follow up.
*p<0.05-significant