Metastatic Renal Cell Carcinoma Causing Small Intestinal Polyps with Intussusception: A Report of Two Cases
M Vani1, Ajit Nambiar2, K Geetha3, Byju Kundil4
1 Associate Professor, Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
2 Associate Professor, Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
3 Professor and Head of Deparment, Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
4 Associate Professor, Department of Gastrosurgery, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M Vani, Associate Professor, Department of Pathology, Academy of Medical Sciences, Pariyaram Medical College, Aavani, Trichambaram, Taliparamba Post, Kannur, Kerala, India.
E-mail: vanim250180@gmail.com
Renal cell carcinomas have diverse clinical presentations. Patients may present with metastatic symptoms at the time of diagnosis or years after resection of primary tumour. Small intestine is a rare site for metastatic renal cell carcinoma. Presentation as polypoid metastasis with intussusception is extremely rare. Here, we report two cases with this rare presentation. Case 1 was a 65-year-old male with multiple polypoid metastasis causing intussusception while on palliative chemotherapy for renal cell carcinoma. Case 2 was a 68-year-old female with history of nephrectomy presenting with single polypoid metastasis causing intussusception.
Immunohistochemistry, Jejunal intussusceptum, Malignancy
Case Report
Case-1
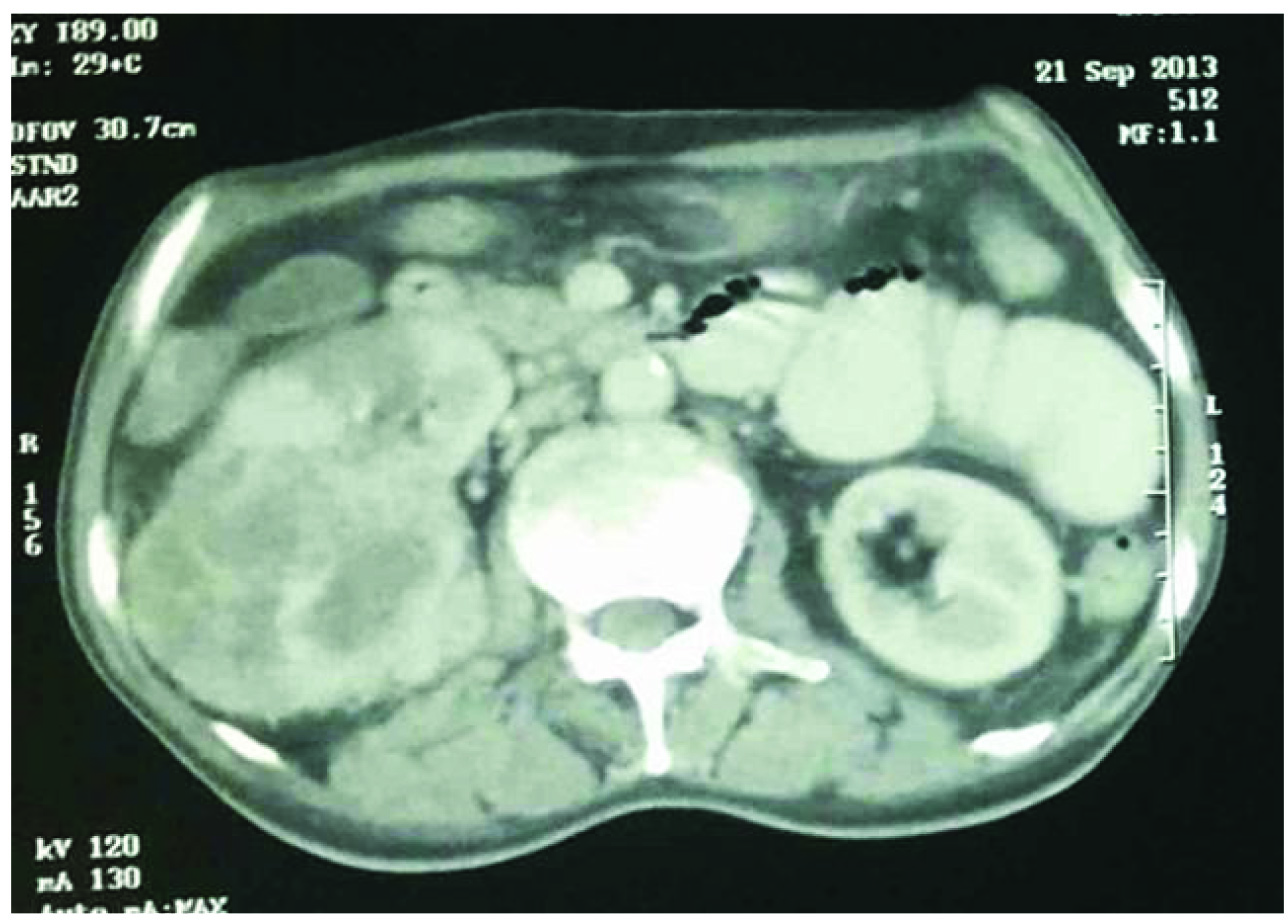
A 65-year-old male presented with acute onset abdominal pain to gastrosurgery casuality. He had a history of right hemiparesis four months prior for which he was investigated. Radiological investigations done during that admission showed intracranial space occupying lesion suggestive of metastasis. Further investigations showed right renal mass suggestive of renal cell carcinoma on abdominal Computerized Tomographic (CT) scan and metastatic lesions in both lungs on CT thorax. As the patient was not willing for surgery he was given supportive care and palliative radiotherapy. While on treatment, patient developed acute abdominal pain. CT abdomen showed jejunojejunal intussusception and right renal mass [Table/Fig-1]. An emergency laparotomy was done and a segment of jejunum, 42 cm long was received for histopathological study. The intussusceptum was 8 cm in length with two polyps at the tip, each of which measured 2x1 cm. Rest of the mucosa showed two polyps of which the larger measured 3x3 cm and the smaller measured 0.75x0.5 cm. Cut section of all the polyps were brownish with grey white areas [Table/Fig-2]. Three mesenteric lymph nodes were identified and the largest measured 1x0.5 cm.
Computed tomographic scan showing right renal mass and jejunojejunal intussusception in Case 1.
Resected segment of small intestine with multiple polyps in Case 1. Polyps at tip of intussusceptum (red arrows) and other polyps (blue arrows).

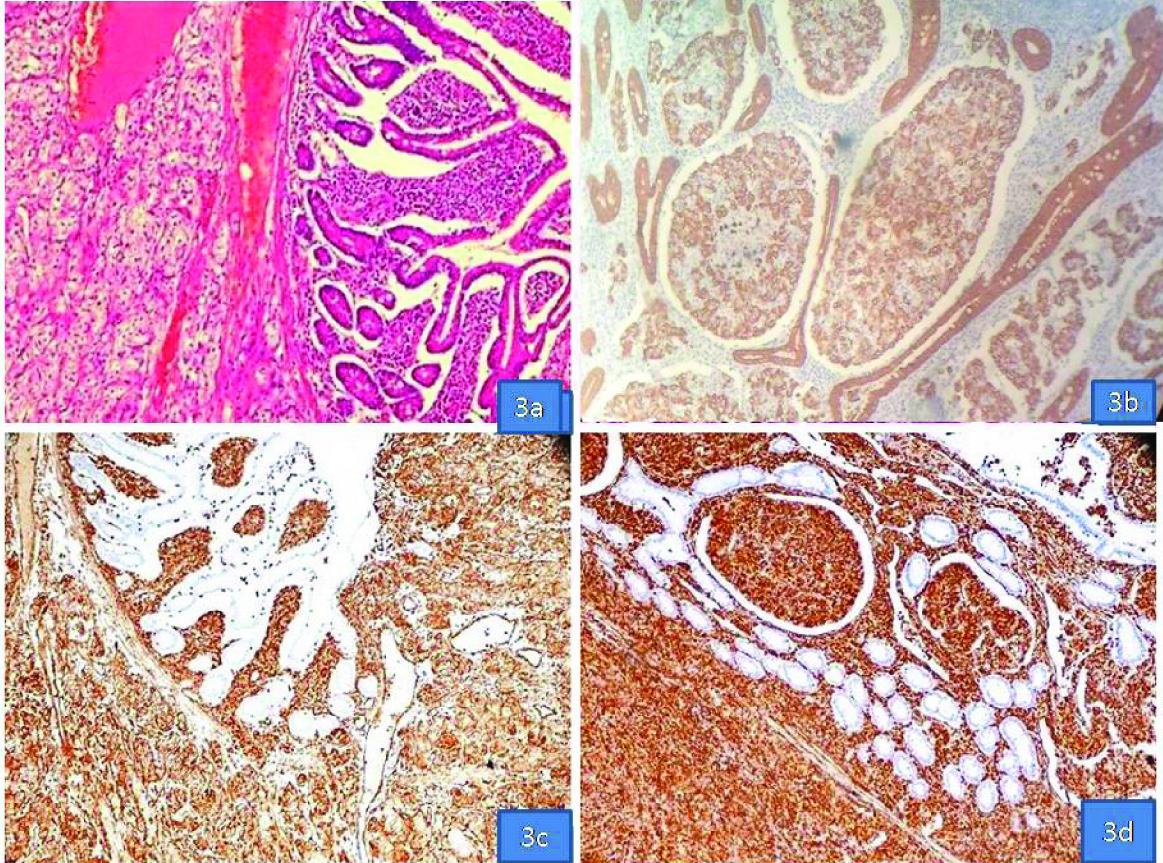
Polyps on microscopy showed jejunal mucosa with an underlying neoplasm composed of cells in trabecular and alveolar pattern with uniform small centrally placed vesicular nuclei, inconspicuous nucleoli and abundant clear cytoplasm separated by delicate fibrovascular septae [Table/Fig-3a]. Mesenteric lymph nodes also showed tumour deposits of similar morphology. Immunohistochemistry showed positivity for pancytokeratin [Table/Fig-3b], vimentin [Table/Fig-3c] and CD10 [Table/Fig-3d]. The final diagnosis was jejunojejunal intussusception with multiple polypoid metastasis of clear cell renal cell carcinoma.
a) Jejunum with a submucosal tumour composed of clear cells in trabecular and alveolar pattern (H&E 10X); b) Pancytokeratin positivity in tumour cells (IHC10X); c) Vimentin positivity in tumour cells (IHC 10X); d) CD10 positivity in tumour cells (IHC 10X) {all in Case 1}.
Case-2
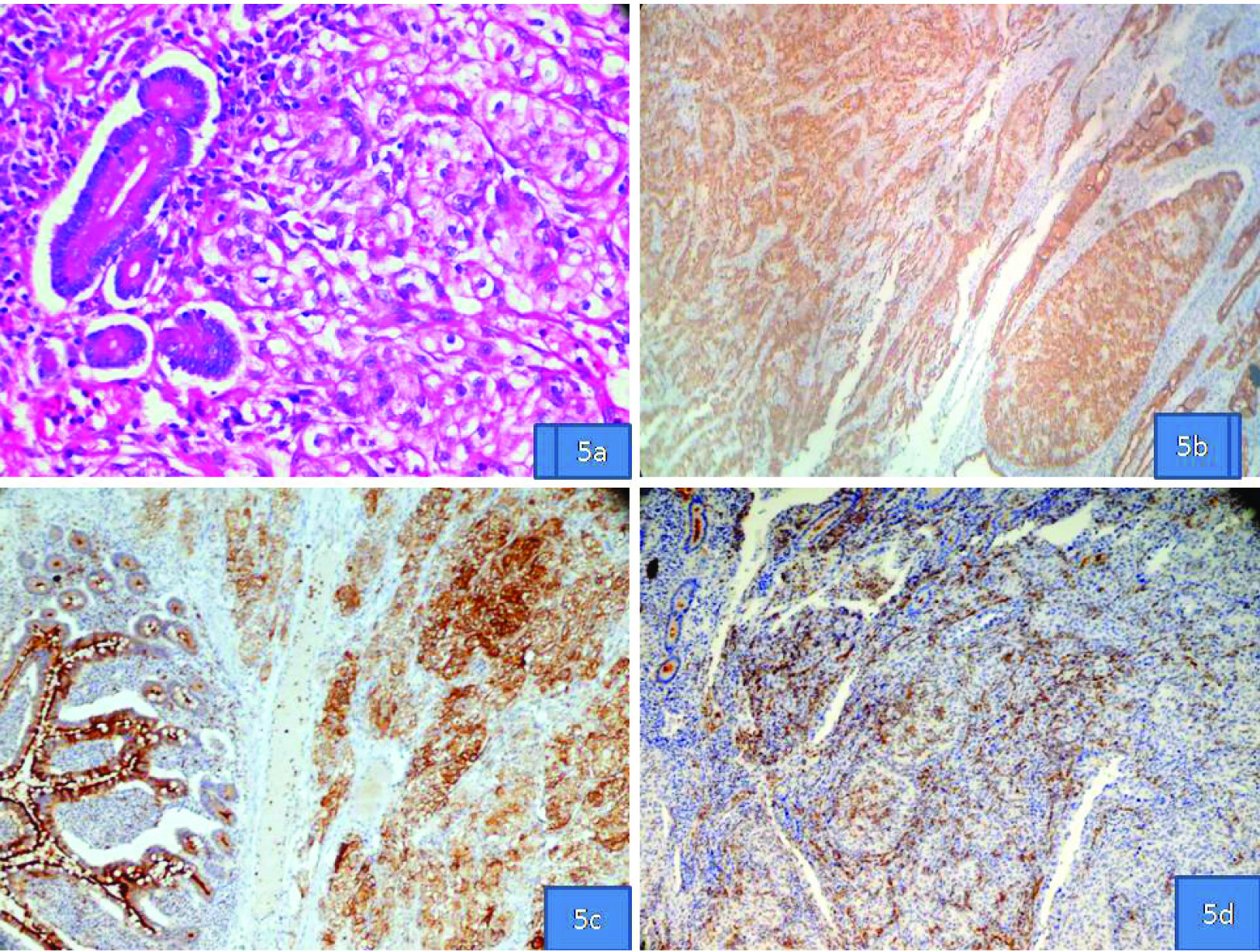
A 68-year-old female with history of right radical nephrectomy four years back diagnosed as clear cell renal cell carcinoma presented with acute abdominal pain. CT abdomen showed jejunal intussusception and an emergency laparotomy with jejunal resection was done. The resected segment of jejunum was 16 cm long with an intussusceptum 6 cm long and a polyp at its tip which measured 5x4.5 cm [Table/Fig-4]. Multiple matted mesenteric lymph nodes were also present. Jejunal polyp and lymph nodes on microscopy showed nests of clear cells with moderate atypia separated by fibrovascular septae [Table/Fig-5a]. Extensive lymphatic tumour emboli were also present. Immunohistochemistry showed vimentin [Table/Fig-5b], pancytokeratin [Table/Fig-5c] and CD10 [Table/Fig-5d] positivity. The final diagnosis was metastatic clear cell renal cell carcinoma with intussusception.
Resected segment of small intestine with polyp at the tip of intussusceptum (marked with arrow) in Case 2.

a) Jejunum with submucosal clear cell nests (H&E, 40x); b) Vimentin positivity in tumour cells (IHC 10X); c) Pancytokeratin positivity in tumour cells (IHC 10X); d) CD10 positivity in tumour cells (IHC 10X) {all in Case 2}.
Both patients were given supportive care and palliative radiotherapy. Our first patient died three months after surgery and the second patient died six months after surgery.
Discussion
Renal cell carcinomas constitute 3% of all adult malignancies and have diverse clinical presentations. Patients may present with classical symptoms like hematuria and loin pain or with features of metastatic disease. Less than half of the patients have metastatic disease at the time of diagnosis [1]. Metachronous disease has been reported in up to 50% of patients treated with nephrectomy for renal cell carcinomas and may be seen years after treatment of primary disease [2]. Our first patient presented with metastatic disease in brain and lungs before the detection of primary tumour and with multiple jejunal metastasis after four months. The second patient presented with jejunal metastasis two years after resection of primary tumour. Common sites of metastasis in renal cell carcinoma are lungs, lymph nodes, bone and liver. Secondary tumours of small intestine are more common than primary tumours and have been documented in 1% to 2% of malignancies. Of the metastatic tumours melanomas are the commonest [3]. Renal cell carcinomas make up 7.1% of tumours metastatic to small intestine. Most common presentation is gastrointestinal bleeding. Rare cases present with obstructive symptoms in the form of intussusception. Multiple polypoid metastasis as seen in one of our cases is extremely rare [4-6]. Intussusception unlike in children is not common in elderly and is usually associated with an underlying neoplasm [6]. A few cases of intussusception caused by small intestinal metastasis of renal cell carcinomas have been reported, but multiple polypoid metastasis causing intussusception is extremely rare [7].
The most common gross presentation is that of a polypoid lesion as in our cases. Case1 had multiple polyps [4-7]. In most of the reported cases of small bowel metastasis the tumours had the morphology of clear cell carcinoma [4,6-8]. In our cases, the tumours had the characteristic histopathological features of clear cell carcinoma. Immunohistochemistry showed co-expression of pancytokeratin, vimentin and CD10 in tumour cells which along with a history of renal cell carcinoma confirmed the diagnosis of metastatic clear cell renal cell carcinoma in both cases and excluded the possibility of other metastatic clear cell tumours of small bowel [9]. An increasingly recognized primary tumour with clear cell morphology having predilection for small intestine is gastrointestinal clear cell sarcoma. These are aggressive tumours predominantly seen in young adults with strong diffuse expression of S-100 protein [10].
Treatment options in metastatic renal cell carcinoma depend on the extent and location of metastatic disease. Even with best available treatment prognosis is poor.
Conclusion
Metastatic tumours can involve the small intestine in the form of polypoid lesions causing obstructive symptoms. Though the most common primary tumours causing small intestinal metastases are malignant melanomas and carcinomas of lung, breast and ovary, the possibility of metastatic disease should also be thought of in patients with primary renal cell carcinoma presenting with features of intestinal obstruction. In our cases the patients presented with polypoid lesions causing intestinal obstruction.
[1]. Tiwari P, Tiwari A, Vijay M, Kumar S, Kundu AK, Upper gastrointestinal bleeding-rare presentation of renal cell carcinomaUrol Ann 2010 2:127-29. [Google Scholar]
[2]. Yuvaraja BT, Mahantshetty U, Chamarajanagar RS, Raibhattanavar SG, Tongaonkar HB, Management of renal cell carcinoma with solitary metastasisWorld J Surg Oncol 2005 3:48 [Google Scholar]
[3]. Willis RA, Secondary tumours of the intestinesThe Spread of Tumours in the Human Body 1973 3rd edLondon, EnglandButterworth & Co Ltd:209-15. [Google Scholar]
[4]. Vashi PG, Abboud E, Gupta D, Renal cell carcinoma with unusual metastasis to the small intestine manifesting as extensive polyposis: Successful management with intraoperative therapeutic endoscopyCase Rep Gastroenterol 2011 5:471-78. [Google Scholar]
[5]. Roviello F, Caruso S, Moscovita Falzarano S, Marrelli D, Neri A, Rampone B, Small bowel metastases from renal cell carcinoma: A rare cause of intestinal intussusceptionJ Nephrol 2006 19:234-85. [Google Scholar]
[6]. Hegde RG, Gowda HK, Agrawal RD, Yadav VK, Khadse GJ, Renal cell carcinoma presenting as small bowel obstruction secondary to a metastatic ileal intussusceptionJournal of Radiology Case Reports 2014 8:25-31. [Google Scholar]
[7]. Eo WK, Kim GY, Choi SI, A case of multiple intussusceptions in the small Intestine caused by metastatic renal cell carcinomaCancer Res Treat 2008 40:97-99. [Google Scholar]
[8]. Sridhar SS, Haider MA, Guindi M, Moore MJ, A case of small bowel obstruction due to intraluminal metastases from metastatic renal cell cancerThe Oncologist 2008 13:95-97. [Google Scholar]
[9]. Shen SS, Truong LD, Scarpelli M, Lopez-Beltran A, Role of immunohistochemistry in diagnosing renal neoplasmsArch Pathol Lab Med 2012 136:410-17. [Google Scholar]
[10]. Wang J, Thway K, Clear cell sarcoma-like tumour of the gastrointestinal tractArch Pathol Lab Med 2015 139:407-12. [Google Scholar]