Dental caries still has high prevalence although there have been various advances in the field of dentistry with primary focus shifting on to preventive dentistry [1]. The demineralization – remineralization cycles occur throughout the life time, which attributes to the limited reparability of the enamel by mineral gain. Thus, this may result in either control of the lesion or reversal of caries [2].
Rather than surgical approach, biological approach is the basic principle of remineralization of initial carious lesions. The reversal of initial enamel lesions can occur by use of remineralizing agents which is the key element of biological approach. According to Backer-Dirks, half of the white spot lesions in young individuals remineralized due to the electrically charged hydration layer present around the enamel crystals [3].
Among the remineralization techniques available, the relatively newer products, CPP-ACP and Bioactive Glass (BAG) are commercially available as GC Tooth Mousse and Vantej respectively. Latest among these is the resin–infiltration technique, commercially available as, Icon. With the advent of all these systems there is great need to quantitatively evaluate the amount of remineralization and one of the techniques to assess the changes in tooth’s mineral content is Scanning Electron Microscope (SEM) equipped with EDAX micro-analyser.
Hence, a study was designed to evaluate the remineralizing potential of CPP-ACP, Vantej and Icon, and to quantitatively measure the amount of mineral gain.
Materials and Methods
This is in vitro study was carried out in Vishnu Dental College, Bhimavaram, Andhra Pradesh, India. Seventy eight maxillary premolars indicated for orthodontic extraction satisfied the inclusion criteria of the study were collected. Ethical Committee clearance was obtained for the use of extracted natural teeth in the study.
Inclusion Criteria: Morphologically, intact non-carious maxillary premolars which are extracted for orthodontic reasons were included in the present study.
Exclusion Criteria: Teeth with morphological variations, fractured crowns, fluorosed teeth, hypoplastic lesions were excluded from the study.
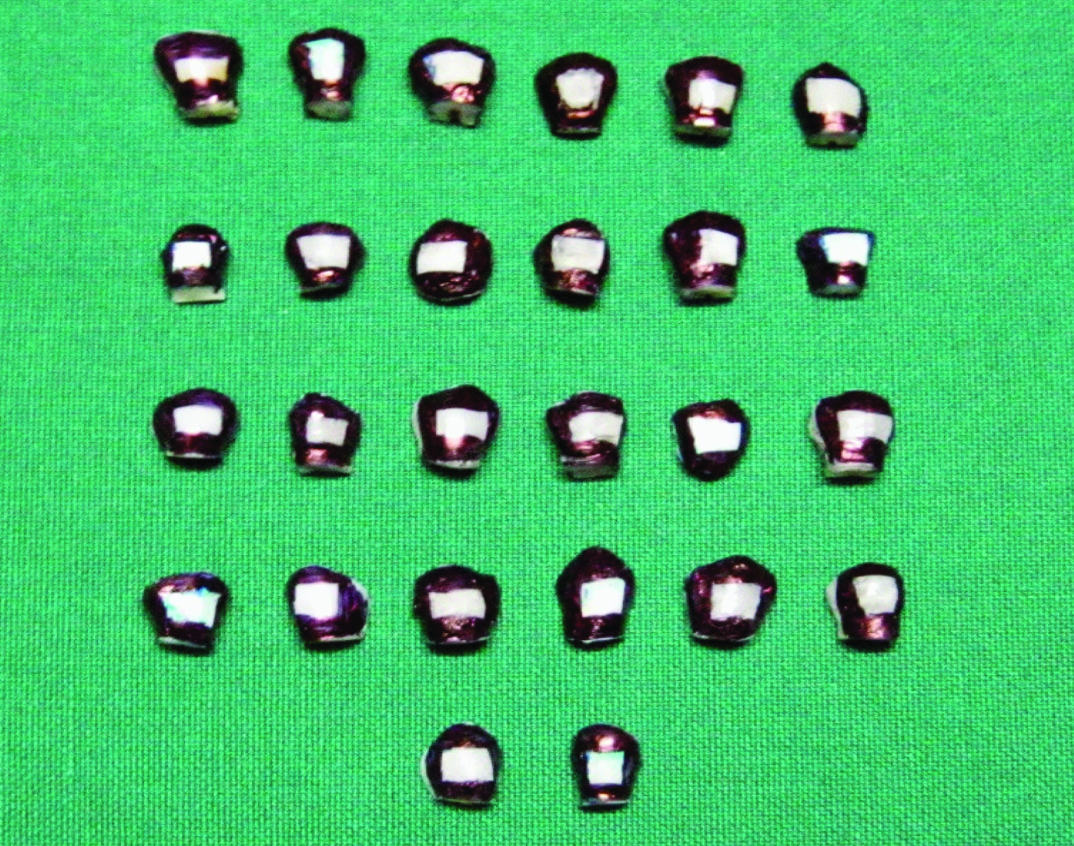
The teeth were cleaned to remove blood or any tissue debris and stored in 0.1% wt/vol thymol solution till demineralization. The tooth buccal surfaces were polished with pumice slurry with the help of a low speed hand piece and a rubber cup followed by washing in distilled water and drying in oil free air with the help of three way syringe. The teeth were decoronated at CEJ [Table/Fig-1] and sectioned mesiodistally into two halves to obtain a flat palatal surface for stabilization of the sample during mounting procedure.
Sectioned enamel samples with exposed area for remineralization.
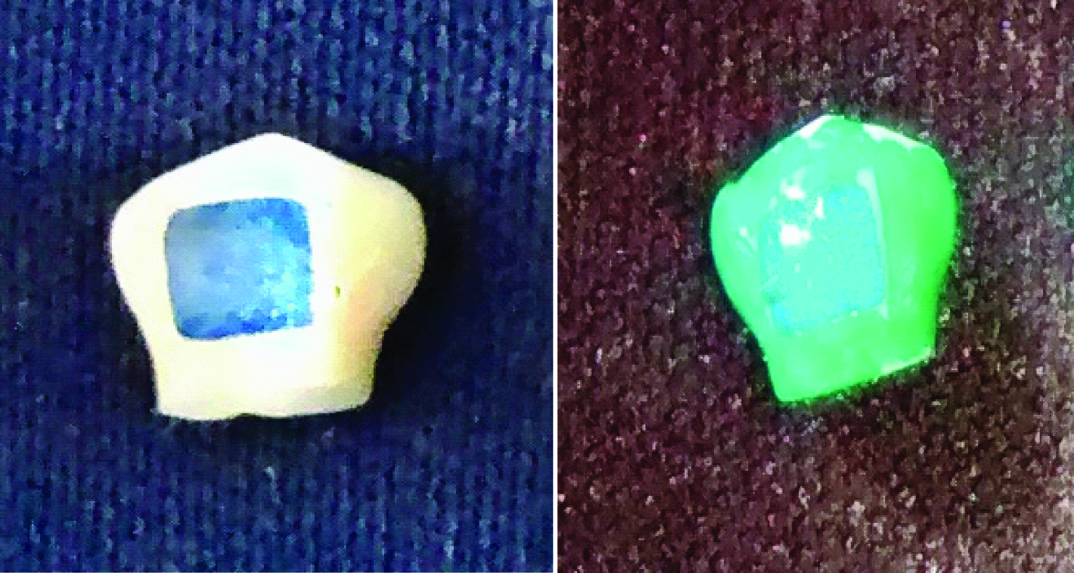
On the centre of the buccal surface a 4 x 4 mm label sticker was placed and the remaining surface was covered with a coloured varnish using applicator brush [Table/Fig-2]. The specimens were divided into three groups of 26 each randomly. They were labeled as: group 1: Vantej (1-26), group 2: CPP-ACP (27-52), group 3: Icon (53-78). The 4 x 4 mm label on buccal surface was removed and all the enamel samples were sputter coated and subjected to SEM- EDX analysis. Mineral content (wt %) of the sound specimens were measured using EDAX, and recorded.
Buccal surface of the enamel slab with 4 x 4 mm label and the remaining surface covered with colour varnish.
Specimens were placed in demineralizing solution incubated at 37° C for 96 hours, to produce artificial caries like lesions. Modified Ten Cate’s solution was prepared in biochemistry laboratory according to the composition specified by John Hicks which consist of 2.2 mmol calcium, 2.2 mmol phosphate, 5.0 mmol fluoride, pH 3.75 and used to demineralize the enamel structure [2]. Followed by this, remineralization procedure was carried out using three different remineralizing agents.
a) Group 1 – Remineralization by Vantej
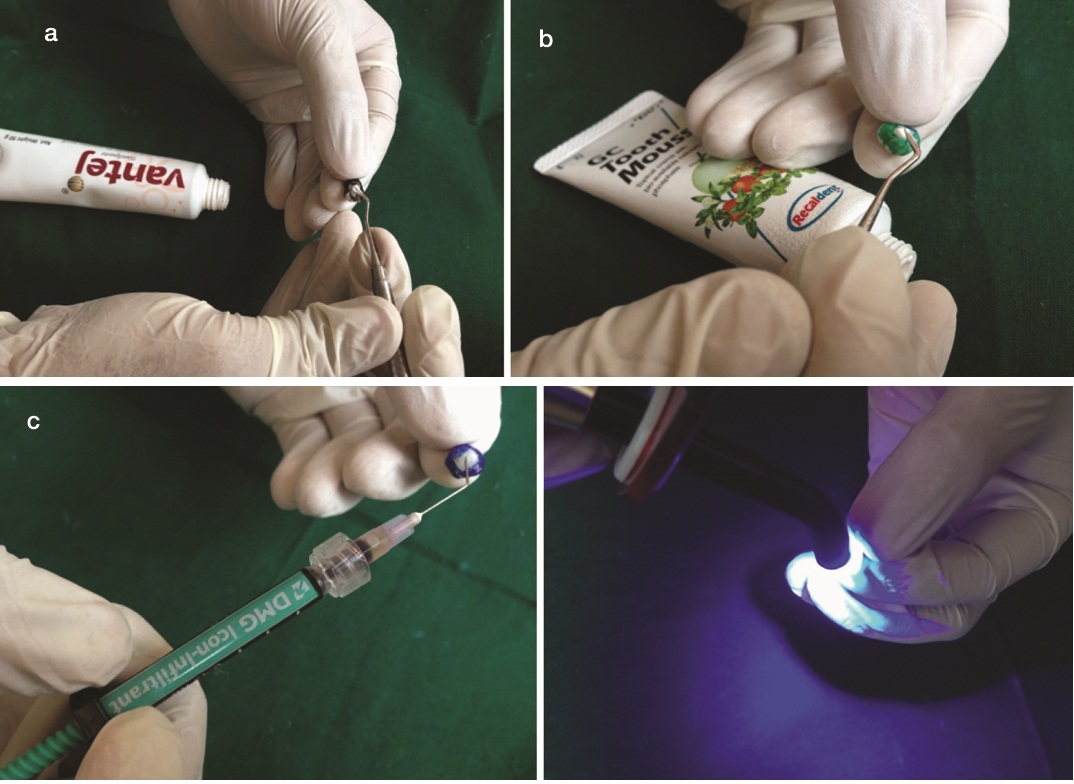
After demineralization, the group I samples were treated with Vantej paste with a soft brush for five minutes and stored in artificial saliva(Glandsone, Synthetic Saliva, UKMi). The procedure was repeated for 28 days and the storage solution was changed every day. [Table/Fig-3a]. After 28 days the samples were cleaned with running distilled water and dried using oil free air from a three-way syringe for five minutes and then subjected to SEM-EDX analysis and the values of mineral content (wt%) were recorded.
Application of remineralizing agents. (a) VANTEJ; (b) CPP-ACP; (c) ICON.
b) Group 2 – Remineralization by CPP-ACP
Similar demineralization-remineralization protocol was followed as in group 1 using CPP-ACP [Table/Fig-3b].
c) Group 3– Remineralization by Icon
After demineralization the group 3 samples were treated with resin infiltrant -Icon. The samples were etched with 10% hydrochloric acid then dried with ethanol followed by resin infiltrant application and visible light cured for 40 seconds [Table/Fig-3c]. Samples were stored in artificial saliva for 28 days which was changed every day. After 28 days the samples were cleaned with running distilled water and dried using oil free air from a three-way syringe for five minutes and then subjected to SEM-EDX analysis and the values of mineral content (wt%) were recorded.
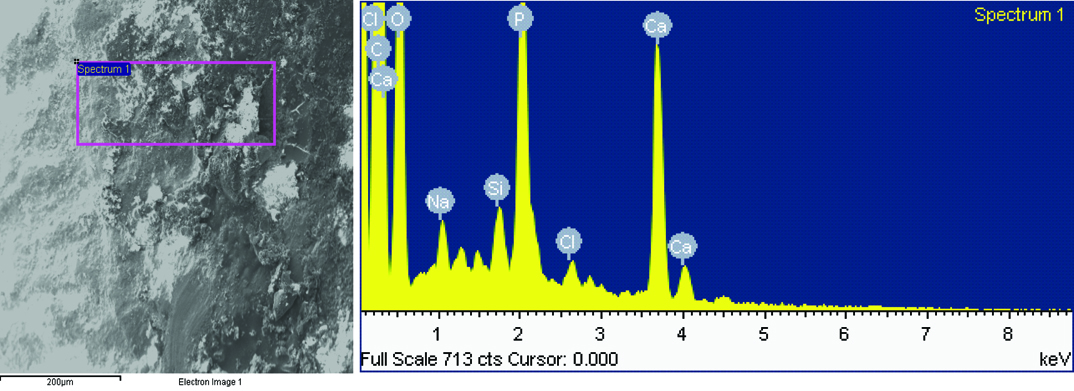
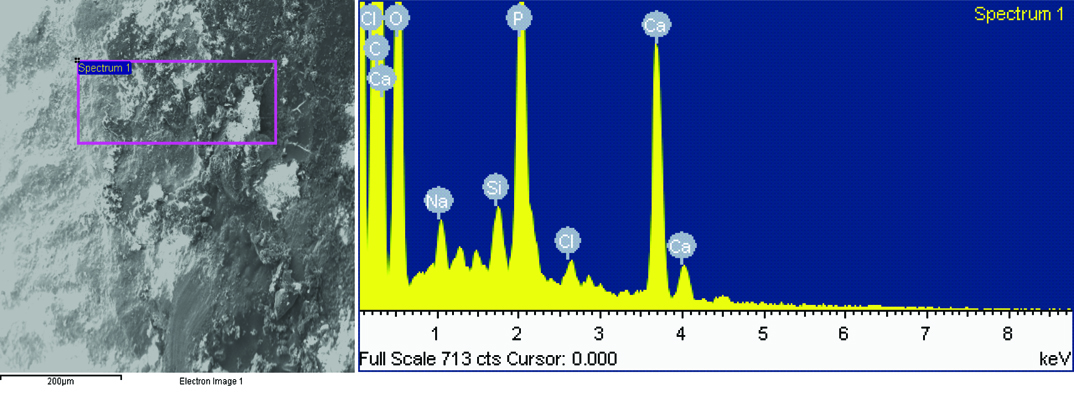
SEM-EDX analysis of the samples before demineralization [Table/Fig-4] and after remineralization [Table/Fig-5] were evaluated and showed deposition of mineral content after application of the remineralizing agent. But the deposited mineral content varied among groups and hence the remineralization potential.
SEM/EDX analysis of a sample before demineralization.
SEM/EDX analysis of a sample after demineralization.
Differences in mean Ca:P between the groups for sound enamel, and remineralized enamel was analysed by ANOVA [Table/Fig-6] followed by Post-Hoc Tukey pair-wise comparison test [Table/Fig-7] using statistical package for the social sciences, version 17.0.
Comparison of net increase in CA/P ratio after remineralization cycle between the groups.
| Groups | Number | Mean | Std. deviation | F value | p value |
|---|
| Vantej | 26 | .4677 | .34616 | | |
| ICON | 26 | .0077 | .21444 | 15.344 | .000* |
| CPP-ACP | 26 | .4235 | .42596 | | |
Pair wise comparison of net increase in ca/p ratio using post-hoc analysis (tukey’s test).
| Group 1 | Group 2 | Mean Difference (Group 1- Group 2) | Std. Error | Sig. | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Vantej | Icon | .47846* | .09436 | 0.106 | -0.0776 | 1.0345 |
| Cpp Acp | -.10000 | .09436 | 0.903 | -0.6560 | .4560 |
| Icon | Vantej | -.47846* | .09436 | 0,106 | -1.0345 | 0.0776 |
| Cpp Acp | -0.5184* | .09436 | 0.400 | -1.1345 | -0.0224 |
| Cpp Acp | Vantej | -.10000 | .09436 | 0.903 | -0.4560 | 0.6560 |
| Icon | .57846* | .09436 | 0.040 | 0.0224 | 1.1345 |
Results
After remineralization, the results showed significant difference between the groups with p-value less than 0.05, when Ca:P were compared, showing greater potential of remineralization for CPP-ACP (132.7%) followed by Vantej (109.8%) and then Icon (98.1%) group [Table/Fig-6].
This indicates increased remineralization potential of 32.7% with CPP-ACP and 9.8% with Vantej when compared to the base line values. On the contrary application of Icon resulted in 2.1% decrease in remineralization potential when compared to the sound enamel samples.
Discussion
Dental caries is a multi-factorial disease process caused by acids, from bacterial metabolism, dissolving the mineral content of enamel and dentine. It is defined as a “complex disease caused by an imbalance in physiologic equilibrium between tooth mineral content and biofilm fluid i.e., saliva” [4].
Demineralization is a process in which the inorganic content of the enamel structure is lost leading to occurrence of white spot lesions. In the present study, the demineralization solution used was similar to the solution use by Hicks MJ and Flaitz CM [5]. In natural condition, demineralization starts at a critical pH of hrdroxyapatite i.e., 5.5, when the oral environment is undersaturated with mineral ions, relative to mineral content of teeth [6]. Remineralization helps in regaining the lost calcium, phosphate, and fluoride ions of the tooth structure and is replaced in the form of fluorapatite crystals, which are more resistant to acidic dissolution and substantially larger than the original crystals [7]. As the severity of plaque acid attack increases, pH drops down to about 4.5, thus action of ‘F’ becomes ineffective in controlling the lesion progression [8]. Despite the presence of fluoride as a gold standard agent in toothpastes caries is still ubiquitous [9].
As the availability of calcium and phosphorous in the oral environment is a key requisite in the remineralization of enamel, it has led to the development of novel materials that can provide essential elements for remineralization.
BAG is a novel material, which acts as a biomimetic mineralizer, matching own body’s remineralizing traits [10]. Although previously it was used for treating sensitivity, recent studies are focussed on the remineralization potential [11] as it consists of ions like calcium, phosphorous, sodium, silica [12]. In the oral cavity, when BAG is applied to the carious lesion, sodium ions from BAG exchange with H+ ions in the saliva, and thus there is increased release of calcium and phosphorous ions [13]. A localized transient increase in pH occurs, which helps in the formation of calcium phosphate layer due to the precipitation of extra calcium and phosphate ions from BAG. As this reaction continues, this layer crystallizes into the hydroxyl carbonate apatite [14]. Hence, BAG has the potential to remineralize initial enamel lesions [10]. But further quantification techniques to achieve more conclusive results were suggested.
Anticariogenic potential of CPP [15] has been attributed to the ability of CPP to localize ACP at the tooth surface. CPP maintains super saturation of calcium and phosphate ions thus modulating the bioavailability of calcium phosphate levels and finally leading to an increase in remineralization [16] Thus, CPP-ACP has shown to reduce demineralization and enhance remineralization of the enamel subsurface carious lesions. CPP-ACP has remineralizing effect on artificial subsurface enamel lesions and the remineralization effect increased with increase in the usage of the paste on 1st, 5th and 10th day respectively [17]. There are studies comparing the enamel remineralization potential of CPP-ACP and BAG [18] and it was clearly shown that samples of both the groups had plugs that sealed the fissures formed by demineralization and hence it was concluded that both BAG and CPP-ACP were capable of remineralizing early carious lesion and BAG had the potential to remineralize to a greater extent when compared to CPP-ACP. In another study it was considered that both the materials are effective in repair and prevention of demineralization and BAG showed better results initially, but eventually both had similar remineralizing potential [19]. As there are limited studies comparing the remineralization potential of these materials using the quantification techniques, they are included in the present study.
A recent approach, resin infiltration, has evolved in minimally invasive dentistry. It was developed at Charite Berlin, for the management of the smooth surface and proximal non-cavitated lesions [20]. It is a novel technology which is an intermediary treatment option between preventive and restorative dentistry [21]. It is marketed under the name Icon. A recent in vitro study showed superior aesthetic results of resin infiltration of artificial white spot lesions when compared with remineralization after the application of fluoride [22]. Icon was included in the present study to evaluate the remineralizing potential if present.
In the present study, evaluation of remineralizing effect of CPP-ACP, Vantej and Icon was done by using EDAX. EDAX is considered the gold standard for the evaluation of mineral loss or gain in experimentally induced initial caries lesions. It is a micro-analytical technique used in conjunction with SEM, which does the structural analysis [23].
Results of this study showed statistically significant difference on comparing the Ca:P wt% between the sound tooth and remineralized sample, with an increased remineralization potential of 32.7% with CPP-ACP. Similarly Vantej showed 9.8% increase in Ca:P wt% when compared to the baseline values.
This study showed that demineralized enamel would not only regain its original value but also showed an increase in mineral content after the remineralization procedure using both CPP-ACP and Vantej. Although CPP-ACP is advantageous than Vantej in terms of remineralization but the advantage of Vantej over another is its cost effectiveness and patients compliance as it is available in the form of dentifrice. However, in the present study remineralization with Icon showed 2.1% decrease when compared to the sound enamel samples. Resin infiltration technique has been considered as a promising micro-invasive approach to prevent demineralization or mechanically stabilize the demineralized enamel [24]. Further clinical trials are necessary to evaluate the protective effect of Icon prior to orthodontic band placement in order to avoid white spot lesions.
The limited degree of remineralization by resin infiltrant has been attributed to the presence of pseudo intact layer formed by obturation of microporosities of the demineralized enamel surface by low viscous resin and possibly by occluding the underlying pores in the carious lesion [24]. It could be hypothesised that, the limited remineralization that is shown by Icon is mainly due to incubation in artificial saliva after the application of remineralizing agent [25].
Till date, it was difficult to deal with the white spot lesions specifically in the aesthetic zones. It either included non-invasive treatment with fluorides or invasive approach with tooth coloured restorative materials. But considering the disadvantages with both the techniques use of micro-invasive approach has shown promising results in immediate masking of the demineralised areas, thus improving the aesthestics.
Limitation
As the study is limited to in vitro conditions, further clinical trials are necessary to assess the remineralization potential and longevity of Icon. As in vitro conditions may be different when compared to the in vivo with dynamic complex biological system, after further research and clinical trials, with proper case selection, Icon may be used as one of the methods to enhance the remineralization. However, in the present clinical scenario, Icon can be used as material to limit the demineralization, as it has the ability to revert back the demineralised enamel to sound enamel.
Conclusion
Within the limitations of the study it can be concluded that CPP-ACP has better remineralization potential than Vantej. Icon on the contrary, showed a decreased remineralization potential when compared to the other two.