Fraternal Twin Tumours of the Oesophagus and Stomach Presenting in the Advanced Stage – A Rare Case with a Fatal End
Saraswathy Sreeram1, Chaithra Gowthuvalli Venkataramana2, Jyoti Ramanath Kini3, Ranjitha Rao4, Nirupama Murali5
1 Assistant Professor, Department of Pathology, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
2 Assistant Professor, Dapartment of Pathology, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
3 Associate Professor, Department of Pathology, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
4 Assistant Professor, Department of Pathology, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
5 Associate Professor, Department of Pathology, Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Saraswathy Sreeram, Assistant Professor, Department of Pathology, Kasturba Medical College, Lighthouse Hill Road, Hampankatta - 575001, Mangaluru, Karnataka, India.
E-mail: swameeram@gmail.com
Synchronous primary tumours of the aerodigestive tract presenting with different histologies is a very rare event. A case with such an association is presented here. A 50-year-old lady presented with symptoms of abdominal obstruction like abdominal pain, distention and vomiting since one month. Her radiological imaging and biopsies revealed a primary oesophageal squamous cell carcinoma and primary gastric adenocarcinoma. Western medical literature has shown the occurrence of multiple synchronous cancers; however, cases from India have seldom been reported. Early screening, correct diagnosis and appropriate plans of management are crucial to reduce the morbidity and mortality of such patients who bear the burden of not just one, but multiple primary cancers.
Gastric adenocarcinoma, Oesophageal carcinoma, Synchronous multiple tumours
Case Report
A 50-year-old housewife was admitted to the hospital with main complaints being abdominal pain, distention and vomiting of one month duration. Pain in abdomen increased on taking food. She was a non-smoker and non-alcoholic. On physical examination, the patient was cachectic with no palpable lymphadenopathy. Respiratory and cardiovascular systems were normal. Abdominal palpation revealed a diffuse indurated mass in epigastrium with presence of succussion splash and shifting dullness.
Laboratory tests showed anemia (Hemoglobin-8.9 g/dl). Other biochemical and hematological parameters like total leukocyte count, liver function tests and renal function tests were within normal limits.
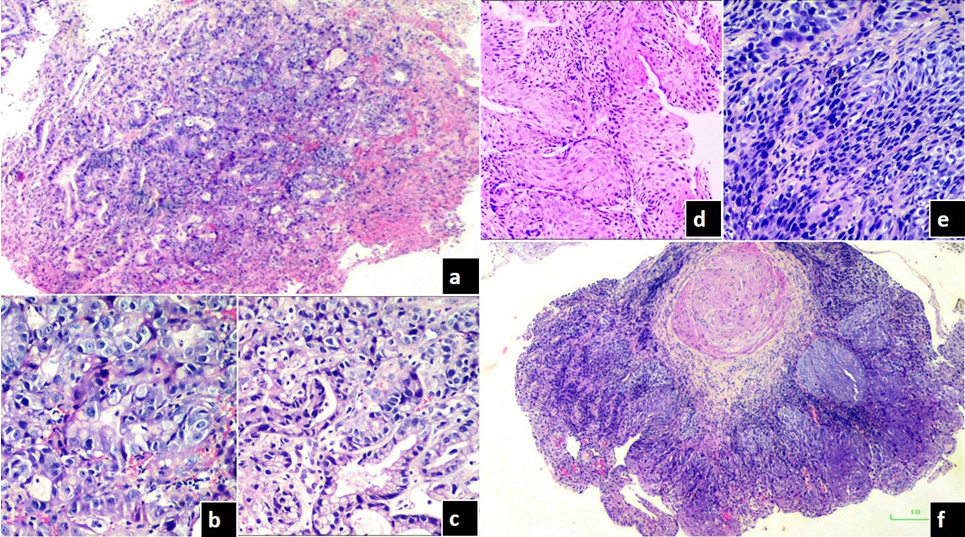
Endoscopy disclosed a proliferative lesion measuring 3x2 cm in the oesophagus, 30 cm from upper incisors and another proliferative lesion in the gastric antrum, circumferential to the pylorus, without stenosis, at a distance of 60 cm from upper incisors measuring 4x4 cm. The histological analysis of biopsies revealed gastric poorly differentiated adenocarcinoma [Table/Fig-1a-c] and oesophageal moderately differentiated squamous cell carcinoma [Table/Fig-1d-f].
a) Malignant cells arranged in ill-defined glandular pattern (H&E, 4X); b) Markedly pleomorphic cells with enlarged nuclei and prominent nucleoli (H&E, 40X); c) A better differentiated area in the same biopsy showing glandular formation (H&E, 20X); d) Hyperplastic squamous epithelium with nests and sheets of malignant squamous cells (H&E, 20X); e) Pleomorphic malignant cells showing high N/C ratio, irregular hyperchromatic nuclei (H&E, 40X); f) Central keratin pearl formation surrounded by invasive squamous cell carcinoma (H&E, 4X).
Ultrasonography of the abdomen showed an irregular circumferential wall thickening with luminal narrowing in pylorus of stomach measuring 4.4x3.8 cm. Liver was normal in size and contour, without signs of focal lesions. Computed tomography scan confirmed the endoscopy and ultrasonography findings and did not show any evidence of metastasis.
Exploratory laparotomy was done and the tumour was found to be inoperable. Hence, jejunostomy was performed. The patient had a fateful postoperative period until the second day after surgery, when she developed complications of sepsis and pneumonia and succumbed to death.
Discussion
Good screening programs and increased cancer survival have led to detection of synchronous and metachronous tumours at increased rates than before. Warren and Gates set criteria for the diagnosis of multiple cancers, which are as follows: 1) all cancers should be malignant by histology; 2) each cancer has to be geographically separate and distinct with presence of intervening normal-appearing mucosa; 3) metastatic cancer should be differentiated from multiple primary cancers and ruled out [1]. Synchronous Multiple Primary Cancers (SMPCs) are defined as those cancers which are diagnosed within six months of each other [2].
Multiple primary cancers in the upper aero-digestive tract have been reported previously as occurring due to “field cancerization” [2]. Squamous Cell Carcinoma (SCC) of the oesophagus is uncommonly associated with other malignancies, particularly of the respiratory tract and the head and neck [3]. Isolated reports of synchronous cancers of the head and neck and oesophagus have been published from India, however, an association as in our case has not been reported to the best of our knowledge from our country [4].
The occurrence of a primary oesophageal SCC and a gastric adenocarcinoma is infrequent, especially when both present in the advanced stage [2]. Oesophageal and gastric cancer share same risk factors, including diet, low socioeconomic status, age, alcohol and tobacco use, nitrites and nitrates. Ichiishi E et al., in Japan proposed the possibility of an autocrine growth-promoting loop involving Granulocyte Colony Stimulating Factor (G-CSF) to be the cause for gastric adenocarcinoma with an oesophageal carcinoma [5].
The incidence of such an event has been reported previously in the world [3,6]. The first association of SCC oesophagus with gastric adenocarcinoma was reported in Japan in 1980. According to the Japanese Committee for Diseases of the Oesophagus data, 1.6% of all the resected oesophageal tumours were associated with stomach tumours. In Rio Grande do Sul, Brazil, a case series of patients with oesophageal SCC showed that 7.28% had a second primary tumour. Among the synchronous tumours, 1.5% were gastric adenocarcinomas [3].
A study conducted in China on SMPCs of upper gastrointestinal tract showed that synchronous oesophageal and gastric cancers were the most common. The male: female ratio was 5.6:1 and the mean age was 59.4 years. The most common histological types were SCC in oesophagus and adenocarcinoma in stomach. Nearly 59% of patients had the history of simultaneous exposure to tobacco and alcohol [1]. In India, however, reports of such an association are scant to our knowledge and therefore, our case is unique.
Synchronous primary squamous cell and adenocarcinomas have also been reported in other sites like anal canal and colon, lung and stomach as well as elsewhere in the digestive system [7-9]. In addition to the squamous and adenocarcinoma components, a concurrent gastrointestinal stromal tumour of the stomach has also been reported recently [10].
Conclusion
In conclusion, the occurrence of synchronous tumours of oesophagus and stomach of different histological appearances is a rare event and has not been reported in this country to the best of our knowledge. Their correct diagnosis is crucial for appropriate radical surgical planning. This synchronous presentation of oesophageal and gastric tumours is important to be evaluated because stomach is the main organ used for digestive tract reconstruction after oesophageal resections.
[1]. Wang R, Wang MJ, Yang JL, Tang CW, Upper gastrointestinal endoscopy detection of synchronous multiple primary cancers in oesophagus and stomach: single center experience from ChinaGastroenterol Res Practice 2012 2012:432367 [Google Scholar]
[2]. Park SJ, Ahn JY, Jung HY, Na S, Park SE, Kim MY, Endoscopic resection for synchronous oesophageal squamous cell carcinoma and gastric adenocarcinoma in early stage is a possible alternative to surgeryGut and Liver 2015 9(1):59-65. [Google Scholar]
[3]. Huguenin JFL, Azevedo VVZ, Almeida HIB, Oliveira IM, Pinto CE, Synchronous oesophageal squamous cell carcinoma and gastric adenocarcinomaArq Bras Cir Dig 2013 26(3):246-47. [Google Scholar]
[4]. Krishnatreya M, Rahman T, Kataki AC, Das A, Das AK, Lahkar K, Synchronous primary cancers of the head and neck region and upper aero digestive tract: Defining high-risk patientsIndian J Cancer 2013 50:322-26. [Google Scholar]
[5]. Ichiishi E, Yoshikawa T, Kogawa T, Yoshida N, Kondo M, Possible paracrine growth of adenocarcinoma of the stomach induced by granulocyte colony stimulating factor produced by squamous cell carcinoma of the oesophagusGut 2000 46:432-34. [Google Scholar]
[6]. Herbella FAM, Lourenco LG, Grande JCD, Possik R, Haddad CM, Synchronous advanced gastric adenocarcinoma and advanced oesophageal squamous cell carcinomaSao Paulo Med J Rev Paul Med 2002 120(1):28-29. [Google Scholar]
[7]. ElGendy K, AlSuwailem M, Salem A, Synchronous anal squamous carcinoma and sigmoid adenocarcinomaBMJ Case Rep 2014 2014:pii:bcr2014206364 [Google Scholar]
[8]. Sato T, Tomaru K, Koide T, Masuda M, Yamamoto M, Miyazawa N, Synchronous lung and gastric cancers successfully treated with carboplatin and pemetrexed: a case reportJ Med Case Rep 2012 6:266-69. [Google Scholar]
[9]. Rajan R, Baqar A, Menon T, An interesting case of primary squamous cell carcinoma of the colon with synchronous metastatic adenocarcinomaClin Case Rep 2014 2(6):323-25. [Google Scholar]
[10]. Zhou Y, Wu XD, Shi Q, Jia J, Coexistence of gastrointestinal stromal tumour, oesophageal and gastric cardia carcinomasWorld J Gastroenterol 2013 19(12):2005-08. [Google Scholar]