A thickened GB wall measures more than 3 mm and typically has a layered appearance at sonography [1]. The thickened GB wall may or may not have layered appearance. Systemic diseases such as heart, renal or hepatic failure cause diffuse and less marked thickening, in contrast to tumour lesions that cause focal and more marked thickening, usually more than 10 mm [2]. GB wall thickening can be due to inflammatory, neoplastic or systemic causes. Inflammatory causes include the acute cholecystitis, chronic cholecystitis, acalculus cholecystitis etc. Neoplastic causes include GB carcinoma and metastasis to GB. Systemic causes include acute pancreatitis, viral hepatitis, hepatic dysfunctions such as cirrhosis etc., [2]. The incidence of incidental GB carcinoma is 5–10 times more in thick walled GBs than in those with normal wall thickness [3].
USG is initially used as a screening tool for evaluation of GBT and the biliary system because it is safe, non expensive and non invasive study [4].
However, CT has become popular for evaluating the acute abdomen because of its high spatial resolution which helps in detailed evaluation of GWT and for staging of the disease [5].
Various GWT enhancement patterns were seen on CECT. Type 1 was a one layer pattern, and Types 2-5 were two layer patterns. The Type 1, pattern was a heterogeneously enhancing one layer GB wall or indistinguishable layering of the GB wall; Type 2, strongly enhancing thick inner layer and weakly enhancing or non enhancing outer layer; Type 3, borderline enhancement and thickness of the inner layer with small cystic spaces and non enhancing outer layer; Type 4, weakly enhancing thin inner layer and non-enhancing thin outer layer; and Type 5, weakly enhancing thin inner layer and non enhancing thick outer layer [6].
Types 1 and 2 patterns are considered to be malignant GWT, although few cases of chronic granulomatous cholecystitis, such as xanthogranulomatous cholecystitis, shows a Type 1 enhancement pattern. Type 3 is considered to be a borderline enhancement pattern including adenomyomatosis; Type 4 as chronic cholecystitis; and Type 5 as acute cholecystitis [6].
The enhancement characteristics of GB wall will be used to characterize GWT into various patterns. Aim of the study was to differentiate benign from malignant lesions on the basis of enhancement characteristics.
Materials and Methods
The present study was a hospital based prospective study conducted in Rajindra Hospital Patiala, Punjab, India on patients who presented with clinical symptoms of suspected GB disease. Patients of all the age groups irrespective of gender were included. Patients who presented with trauma were excluded. The study sample was limited to 60 patients and was done over a period of three years from 2014-2016. Institutional review board approval for conducting this study was obtained and informed consent for study from patients was taken.
USG was performed with Philips Envisor ultrasound machine and Philips HD 11E 3D and 4D machine with 7.5 MHz linear array transducer. The sonographic examination of the GB wall thickness included sagittal, transverse and subcostal oblique views.
CT scan was performed with Siemens- Somatom Emotion 6 slice third generation spiral CT. Slice thickness of 8x8 mm collimation was used. Plain CT scan was performed initially followed by the postcontrast study that included arterial, venous and delayed phase images. CT scan was routinely obtained from the patient during full inspiration in supine position of the patient. Scanning routinely began at the level of the lung bases and proceeded in a craniocaudal direction up to the lower pole of the kidney.
Contrast material: Nonionic iodine contrast 300 mg was used in our study. A 100 ml of contrast was injected intravenously by the peripheral intravenous route at the rate of 2-3 ml/sec. Continuous monitoring of the vital parameters was done during contrast injection.
Histology: Cholecystectomy specimens were received in the Department of Pathology, Govt. Medical College, Patiala from Department of Surgery Rajindra Hospital, Patiala, India. The biopsy material included resected specimen for histopathological diagnosis. All the specimens received were placed in 10% formalin and allowed to fix for atleast four hours. Then after grossing and processing, thin sections were made from suspicious area and the adjoining area. Tissue sections were stained with routine Haematoxylin and Eosin stain (H&E stain).
Statistical Analysis
In present study, all malignant causes of GWT were labelled as true positives and all the benign causes were true negatives. On the basis of these results, final statistical analysis was made. Differences in CT findings between benign and malignant cases were calculated on the basis of Chi-square test and p-value by using SPSS 16 version. A p-value <0.05 was considered significant and p-value <0.001 was considered highly significant.
Results
In present study, 39 patients (65%) were females and 21 (35%) were males. Mean age in present study was 52.13 years. Mean female age in present study was 50.23 and mean male age was 57.57.
Various CT enhancement patterns observed in our patients are described in [Table/Fig-1], provisional radiological diagnosis was made on the basis of these patterns.
Types of CT enhancement patterns in determining various pathologies.
| Radiologiocal diagnosis | Type 1 | Type 2 | Type 3 | Type 4 | Type 5 |
|---|
| Acute acalculus cholecystitis | 0 | 0 | 0 | 0 | 4 |
| Acute calculus cholecystitis | 0 | 0 | 0 | 0 | 2 |
| Complicated cholecystitis | 0 | 0 | 0 | 0 | 4 |
| Chronic cholecystitis | 0 | 0 | 0 | 13 | 0 |
| Xanthogranulomatous cholecystitis | 1 | 0 | 0 | 0 | 0 |
| Non-specific GB wall thickening (Dengue serology positive cases, viral hepatitis and cirrhosis cases) | 0 | 0 | 0 | 2 | 10 |
| Adenomyomatosis | 0 | 0 | 4 | 0 | 0 |
| Mass like diffuse GWT | 8 | 0 | 0 | 0 | 0 |
| Mass like focal GWT | 12 | 0 | 0 | 0 | 0 |
| Total | 21 | 0 | 4 | 15 | 20 |
Patients with mass like focal or diffuse GWT (n=21) suspected malignant on the basis of CT enhancement patterns, underwent open cholecystectomy. Rest of the GWT patients underwent open cholecystectomy (n=10) or laparoscopic cholecystectomy (n=17). No cholecystectomy was done in cases of non specific GWT (n=12) in which the diagnosis was confirmed by patient’s serological records. Histopathology reports were collected in patients who underwent cholecystectomies. On histopathological correlation, out of the 60 cases of GWT, 21 were malignant GWT (adenocarcinoma GB). Out of these 21 cases, 19 cases were true positives and two cases were false negatives. Two false negative cases in which diagnosis of chronic cholecystitis was made on the basis of CT enhancement pattern were later diagnosed as adenocarcinoma GB after final histopathological results.
Thirty nine cases resulted from benign diseases out of which 12 did not undergo cholecystectomy. The other cases in which cholecystectomy was done one case was false negative, which was diagnosed as mass like GWT on the basis of CT enhancement pattern which was diagnosed as adenomyomatosis after final histopathological correlation.
Discussion
Worldwide, GB cancer is the fifth most common malignancy affecting the biliary tract [7]. GB cancers can present as a mass replacing the GB, GWT, or an intraluminal polyp on USG or CT and GWT is the least common presentation and the most difficult to diagnose [7,8]. The presentation of the tumour as diffuse or focal wall thickening is problematic as acute and chronic cholecystitis are included in the differential diagnosis [9,10].
In present study, evaluation of the enhancement features of GWT was done, which had often been considered benign inflammation. Very few studies on GWT enhancement patterns were published in literature. To our knowledge, three studies were there, by Kim SJ et al., and Tongdee R et al., on GWT focusing on layered enhancement patterns using MDCT images [6,11] and other was MRI study of GWT by Jung SE et al., [9].
Our results regarding the enhancement patterns of thickened GB wall are mostly similar to a previous report by Jung SE et al., regarding the layered patterns of GB wall on MRI. Jung SE et al., classified thickened GB wall into four patterns on T2-weighted images on the basis of the features of the inner and outer layer, the presence of striation and the signal intensity of each layer. As per them, acute and chronic cholecystitis showed two layers with an ill-defined or a discrete margin, whereas GB cancer showed diffuse nodular wall thickening without layering. In addition, adenomyomatosis showed multiple cystic spaces of high signal intensity in the thickened wall [9].
The inclusion criteria of present study was similar to the study done by Kim SJ et al., in which the inclusion criteria consisted of flat GWT of more than 3 mm with exclusion of gross GB mass or intrapolypoidal mass [6]. MDCT and USG were the imaging modalities used for evaluation of GWT in our study because MRI was not present in our institute at the time of start of study, so we used MDCT and USG for study of GWT.
Based on the results of present study, the enhancement patterns with a high prevalence of GB cancer was the Type 1 pattern—that is, one layered wall thickening showing heterogeneous enhancement (p-value <0.001). [Table/Fig-2] shows the comparison in enhancement pattern observed in our study with the other studies [6,10,11]. The sensitivity and specificity of Type 1 enhancement pattern on computed tomography for predicting the GB malignancy were 90.476% and 97.43% respectively. The positive and negative predictive values were 95% and 95%, respectively.
Comparison of most common CT enhancement pattern of malignant GB wall thickening in present study with previous published studies.
| Author and year of study | Most common CT enhancement pattern of malignant GB wall thickening | p-value |
|---|
| Yun EJ et al., [10] | Type 2 | NA |
| Kim SJ et al., [6] | Type 2 | <0.001 |
| Tongdee R et al., [11] | Type 1 | 0.001 |
| Present study | Type 1 | <0.001 |
In a study done by Kim SJ et al., Type 2 pattern was most commonly seen followed by Type 1 pattern [6]. These patterns were significantly associated with GB cancer (p-value <0.05) and by using these two enhancing patterns as a sign of malignancy, the diagnostic accuracy of MDCT was 89.1% and 87.6% as observed by two observers respectively. But in our study no case of Type 2 pattern was noted. Our study result was similar to the study done by Tongdee R et al., in which the thickened GB wall with one layer heterogeneous enhancement (Type 1) was significantly associated with malignancy [11].
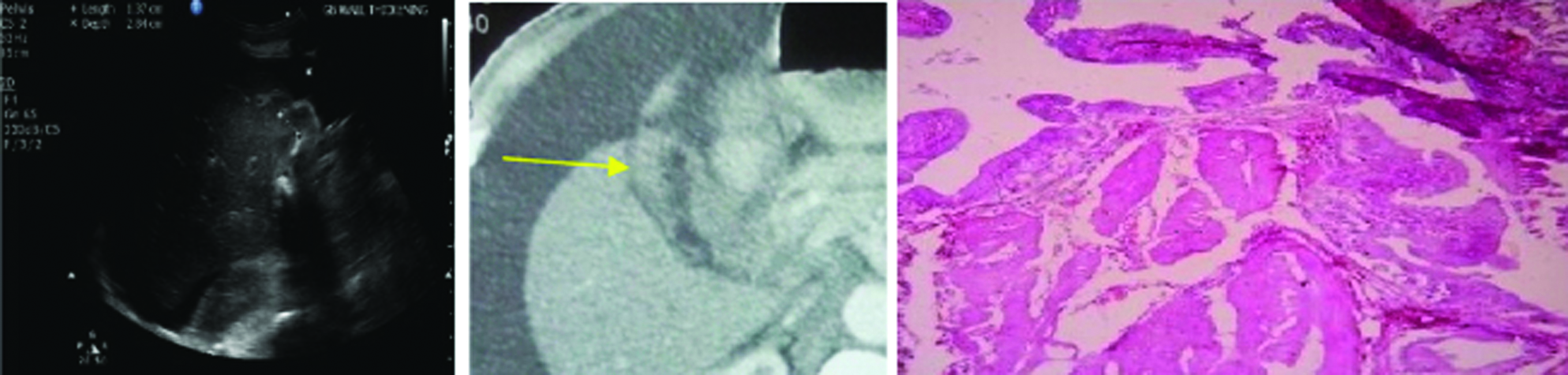
The result of present study is in consistency with those of a previous study done by Yun EJ et al., on GB cancer on biphasic helical CT. The inclusion criteria were different in which all morphologic types of GB cancer (i.e., mass forming, flat GB wall thickening, and polypoid types) were included [10]. However, in present study only flat GB wall thickening cases were included. The most common enhancement patterns of GB cancer in Yun EJ et al., study was a highly enhanced thick inner wall layer seen during the arterial phase (Type 2 pattern), but the most common pattern in present study was thick hetergenously enhancing single layered pattern (Type 1 pattern) [Table/Fig-3] [10].
(a) Ultrasound image shows the diffusely thickened wall with intraluminal calculi; (b) CECT shows Type 1 enhancement pattern with heterogenously enhancing one layered pattern (arrow); (c) Photomicrograph shows scanty fibrous stroma with nests of neoplastic and keratinizing squamous cells that infiltrate the gallbladder wall 4X (H&E stained section) (Images left to right).
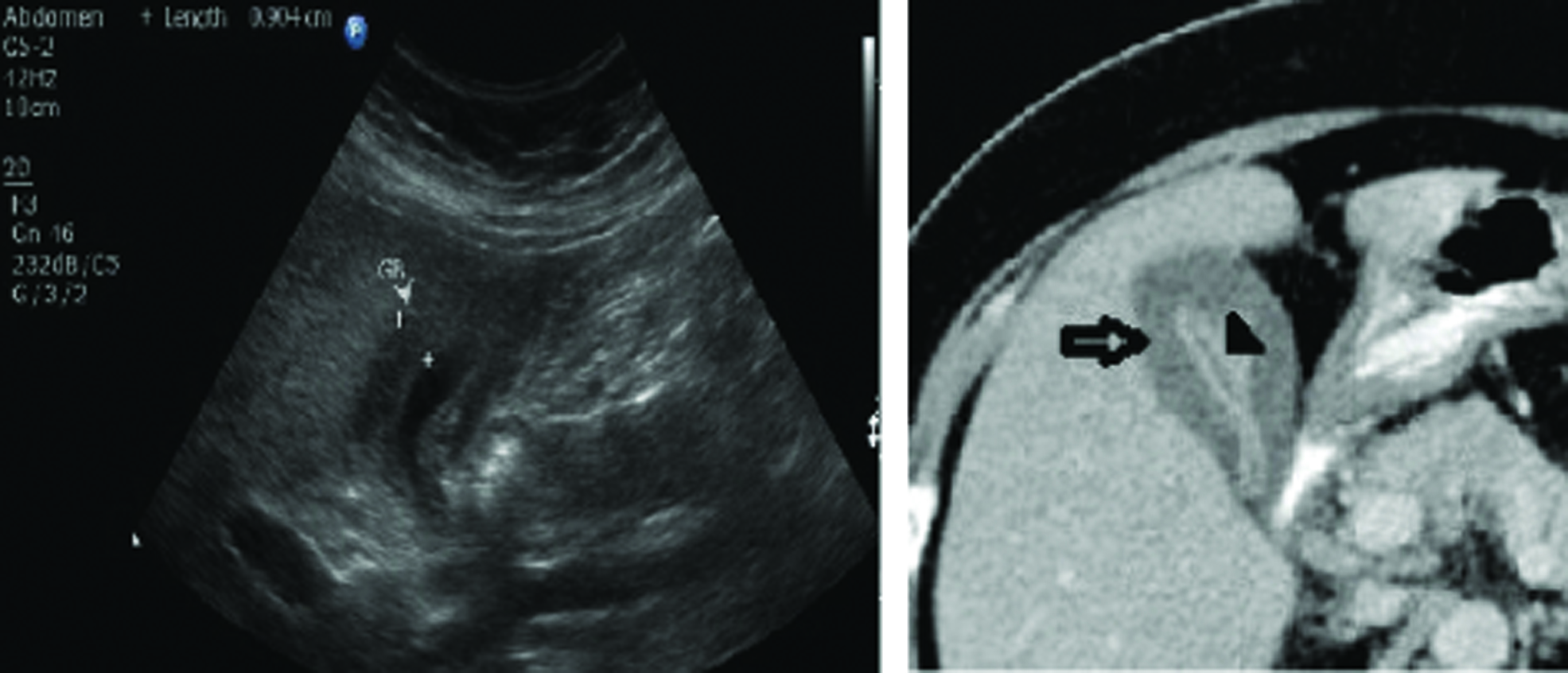
Also we had included the Non-Specific GB Wall Thickening (NSGWT) cases due to cirrhosis, dengue and viral hepatitis. Final confirmation in these cases was done by USG and serology findings. Dengue serology positive cases showed Type 5 enhancement pattern [Table/Fig-4]. Cirrhotic and viral hepatitis patients showed Type 4 pattern.
(a) Ultrasound image shows thickened oedematous gallbladder wall; (b) CECT shows Type 5 enhancement pattern with non enhancing outer layer and weakly enhancing thin inner layer (arrows) (Images left to right).
These were the new findings which were not included in the study done by Kim SJ et al., [6]. In present study, out of nine dengue positive cases, all nine patients had pleural effusion and splenomegaly. Our results are consistent with study conducted by Santhosh VR et al., in which sonographic features of thickened GB wall such as ascites, hepatomegaly, splenomegaly and pleural effusion (bilateral or right side) should strongly favour the diagnosis of dengue fever [12].
The results of present study revealed several imaging features with a high Chi-square value for the diagnosis of GB cancer. These results were comparable with those of a previous study done by Kim SJ et al., regarding the enhancing features of flat GWT [6]. Heterogenously enhancing one layered pattern, focal wall thickening, irregular wall thickening/margins, lymph node enlargement and liver infiltration by the GWT were the features that favour malignant cause of GB wall thickening and were statistically significant [Table/Fig-5]. These five findings involving GWT showed high chi-square value and were statistically significant (p-value <0.05).
MDCT findings that indicate GWT.
| Author and year of study | Findings that indicate malignant GB wall thickening | Chi-square | p-value |
|---|
| Kim SJ et al., [6] | Enhancing inner wall is ≥ 2.6 mm thick | 48.02074 | 0.001 |
| Inner wall is hyperenhancing on portal phase images | 17.60038 | 0.001 |
| Outer wall is ≤ 3.4 mm thick | 16.47201 | 0.001 |
| Outer wall is weakly enhancing or nonenhancing | 6.641802 | 0.001 |
| Wall thickening character is irregular | 13.74092 | 0.001 |
| Wall thickening extent is focal | 12.08907 | 0.001 |
| Present study | Thick heterogenously enhancing one layered pattern | 24.00 | <0.001 |
| Irregular Wall thickening/Margin character | 19.806 | <0.001 |
| Liver infiltration by GWT | 19.806 | <0.001 |
| Focal GWT | 12.089 | 0.001 |
| Lymph node enlargement | 4.9 | 0.027 |
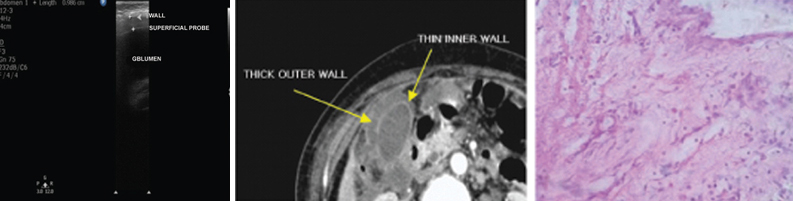
The CT features of acute cholecystitis include gall stones, thickening of the GB wall, pericholecystic fluid, stranding of pericholecystic fat, high-attenuation bile, blurring of the interface between the GB and the liver and transient increase in attenuation of the portion of the liver adjacent to the GB [13]. In our study, we observed that acute cholecystitis showed the Type 5 enhancement pattern [Table/Fig-6], which consists of a smooth weakly enhancing thin inner layer and a non enhancing thick outer layer. The weakly enhancing thin inner layer is consistent with inflamed or sloughed mucosa, and the non enhancing thick outer layer is compatible with an oedematous loose connective tissue layer.
(a) Ultrasound image shows the thickened GB wall with superficial probe (3-12MHz); (b) CECT shows Type 5 enhancement pattern (non enhancing outer layer and weakly enhancing thin inner layer); (c) Photomicrograph shows polymorphs and macrophages along with surface mucosal ulceration and oedema in acute cholecystitis 4x (H&E stained section). (Images left to right).
It is important to differentiate adenomyomatosis from gall bladder carcinoma as it usually presents as focal wall thickening (fundal or segmental type or both types) or as diffuse wall thickening of the GB (diffuse type) [14,15]. According to the results of a previous study by Ching BH et al., although CT is limited in diagnosing adenomyomatosis, this diagnosis can be made with reasonable accuracy when the thickened GB wall contains small cystic-appearing spaces [16]. In present study, there were total five cases of adenomyomatosis, four were true positive cases and one was false positive case. The degree of enhancement and the thickness of the enhancing wall were borderline between GB cancer and cholecystitis, diffuse wall thickening was seen in all of them. Comet tail artifacts were noted along the anterior wall of GB on USG in four cases. Comet tail artifacts are visualized as echogenic intramural foci from which emanate V-shaped comet tail reverberations and are highly specific for adenomyomatosis [Table/Fig-7] [17].
(a) Ultrasound images shows thickened GB wall along with comet tail artifacts and cystic areas; (b) CECT shows Type 3 border line enhancement pattern (GB wall enhancement is less than that of hepatic parenchyma); (c) Photomicrograph shows Rokitansky-aschoff sinuses with inflammatory infiltrate in adenomyomatosis 4x (H&E stained section). (Images left to right).

Sometimes differentiation between adenomyomatosis and chronic cholecystitis was difficult on imaging. Kim SJ et al., showed borderline enhancement pattern i.e., Type 3 in adenomyomatosis cases and Type 4 enhancement patterns in chronic cholecystitis cases [6]. In present study, we found similar results; borderline enhancement pattern [Table/Fig-8] was noted more commonly in adenomyomatosis (4/5 cases, 80%) and chronic cholecystitis showed Type 4 enhancement pattern (13/15, 86.67%) [Table/Fig-8].
(a) Ultrasound image shows thickened GB wall with multiple calculi; (b) CECT shows Type 4 enhancement pattern with weakly enhancing inner layer and non ehnhancing thin outer layer (arrows); (c) Photomicrograph shows gall bladder mucosa with chronic inflammatory infiltrate in the lamina propria 4x (H&E stained section). (Images left to right).
CT and USG helps in preoperative diagnosis of malignant GB wall thickening in most of the cases. However, differentiation between malignant GWT and complicated cholecystitis is often difficult. Focal mass, biliary obstruction at the level of the portahepatis, invasion with protrusion of the anterior surface of the liver and nodal metastases was the signs on MDCT that favour malignant GWT [18]. The CT signs we found most useful in supporting a diagnosis of complicated cholecystitis were a curvilinear low-attenuation band or halo surrounding the GB. This halo corresponds to the mural oedema or pericholecystic fluid collections. In present study, pericholecystic fluid/halo was seen in four patients of complicated cholecystitis and biliomas were seen in two patients of complicated cholecystitis. These features were not seen in case of malignant GWT. Lymph nodal (pericholedochal, peripancreatic and para-aortic) involvement were seen in nine patients of malignant GWT.
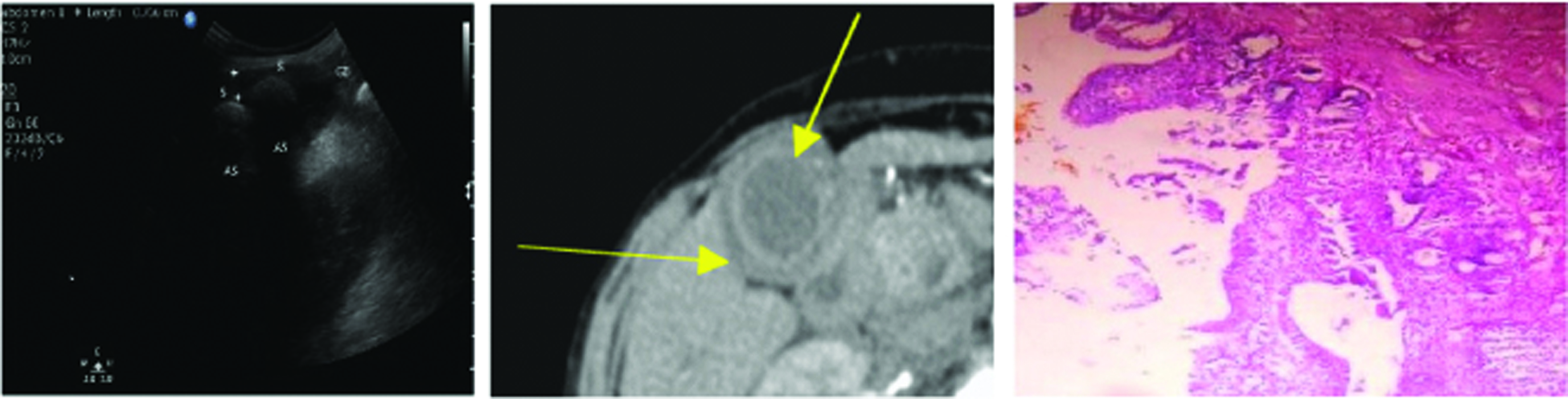
Both Xanthogranulomatous Cholecystitis (XGC) and malignant GWT show Type 1 enhancement pattern [Table/Fig-9], however diffuse GWT, hypoattenuated intramural nodule, gall stone and pericholecystic infiltration were the consistent, significant CT findings of XGC regardless of the cancer staging and focal GWT and distrupted mucosa was more in favour of early GB cancer patients. In present study, one case of XGC was seen and focal GWT was seen in 12 cases of malignant GWT [19].
(a) Ultrasound image shows the thickened GB wall with heterogenous area near the fundus of GB and intraluminal calculi; (b) CECT shows Type 1 enhancement pattern (heterogenously enhancing one layered pattern); (c) Photomicrograph shows degenerated neutrophils and foamy macrophages (arrows) in xanthogranulomatouscholecystitis 4x (H&E stained section). (Images left to right).

The results of the present study indicated that preoperative distinction between benign and malignant GWT is possible with MDCT. In addition, it was seen that MDCT also helped in metastatic workup of malignant GWT before doing any surgical intervention.
Limitation
Our CT scanner was 6 slice third generation spiral CT. So, CT data used in the present study was acquired at 8x8 mm sections thickness which then reformatted to sections ranging from 1.0 to 3.0 mm. As the GB is not perpendicular to the transverse plane, combined interpretation of axial and reformatted coronal and sagittal images would improve the diagnostic performance of CT for the evaluation of the extent of GB wall involvement. Also, during USG some patients had contracted GB status because these patients were not fasting which would interfere with the interpretation of the GWT.
Conclusion
In present study, the thickened GB wall with one layered heterogeneous enhancement pattern (i.e., Type 1) was significantly associated with malignant GWT. In addition, dengue positive serology cases which showed Type 5 pattern and hepatitis and cirrhosis cases showed Type 4 enhancement patterns were also included in present study which were not included in previous published studies on CT enhancement patterns. So, we can differentiate benign from malignant GWT by analysing the enhancement patterns of GB wall on MDCT.