Unicystic Ameloblastoma of Mandible with an Unusual Diverse Histopathology: A Rare Case Report
Kanu Jain1, Gaurav Sharma2, Priyanka Kardam3, Monica Mehendiratta4
1 Reader, Department of Oral Pathology, Maharaja Ganga Singh College of Dental Sciences and Research, Sri Ganganagar, Rajasthan, India.
2 Reader, Department of Oral Medicine, Sudha Rustagi College of Dental Sciences and Research, Faridabad, Haryana, India.
3 Senior Lecturer, Department of Oral Pathology, Sudha Rustagi College of Dental Sciences and Research, Faridabad, Haryana, India.
4 Reader, Department of Oral Pathology, ITS Dental College, Greater Noida, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kanu Jain, Reader, Department of Oral Pathology, Maharaja Ganga Singh College of Dental Sciences and Research, Sri Ganganagar-335001, Rajasthan, India.
E-mail: kanu_priya99@rediffmail.com
Ameloblastomas of jaws are benign odontogenic tumours with four clinical variants being solid multicystic type, unicystic type, extra osseous type and desmoplastic type. Unicystic ameloblastoma accounts for only 13% of all the known cases in the scientific literature. Follicular and plexiform patterns are the commonly seen histopathological patterns in unicystic ameloblastoma. Though rare in itself, presence of granular cells along with acanthomatous changes occurring in unicystic ameloblastoma is a rare phenomenon. We present a rare case report of unicystic ameloblastoma of right mandible with an unusual histopathology. It exhibited both luminal and mural types as well as both acanthomatous and granular cell changes found together. As occurrence of unicystic ameloblastoma of jaws with such varied histopathology is rare, their course, clinical outcome, prognosis and recurrence rate are not clear. Documentation of more such cases in literature may make pathogenesis and nature of these lesions more insightful.
Acanthomatous, Granular, Odontogenic keratocyst
Case Report
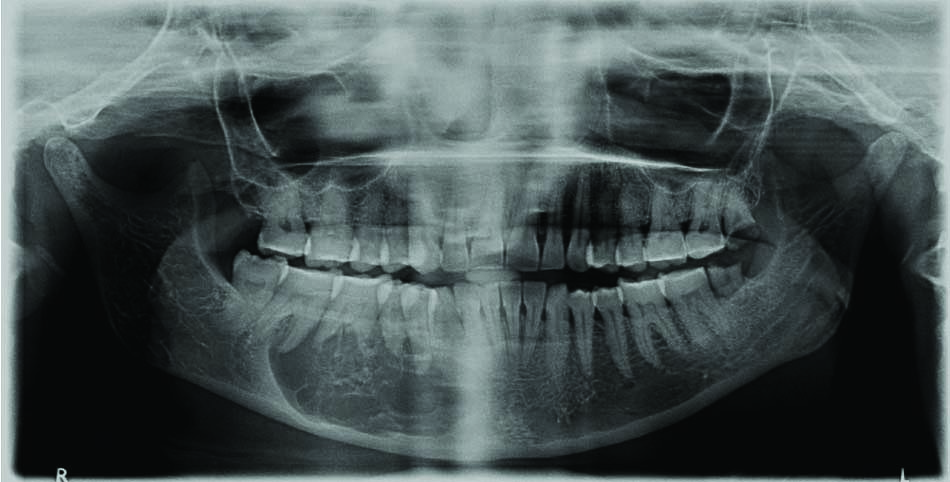
A 37-year-old female patient reported pain and swelling in the mandibular right region since one year. The swelling was well circumscribed, hard, tender and fluctuant. It extended from right corner of lip to angle of mandible and measured 25 x 20 x 21 mm approximately. A panoramic radiograph revealed a multilocular radiolucency extending from distal aspect of mandibular right lateral incisor to distal root of mandibular second molar. Superoinferiorly, it extended from cervical margins of teeth to inferior border of mandible. There was a mixed honeycomb and soap bubble radiographic pattern [Table/Fig-1]. An aspiration of the swelling yielded straw coloured fluid. A provisional diagnosis of odontogenic keratocyst was given. Differential diagnoses of ameloblastoma were made. An incisional biopsy was performed and tissue specimen was sent to laboratory for histopathological examination. Haematoxylin and eosin stained soft tissue sections showed cystic lumen lined by ameloblastomatous epithelial lining of variable thickness [Table/Fig-2]. The epithelium showed proliferation at places within lining and also into connective tissue wall in the form of ameloblastomatous islands [Table/Fig-3]. The cystic lining was formed of basal layer of tall columnar ameloblast like cells displaying nuclear hyperchromatism, palisading and reverse polarity. The overlying layers were composed of stellate reticulum like cells showing granular cell change at places [Table/Fig-4]. A zone of juxtaepithelial hyalinisation was also seen. The islands in connective tissue wall exhibited peripheral tall columnar ameloblast like cells with areas of squamous metaplasia and cystic degeneration. The central cells in other islands showed granular cell change. These cells presented with eosinophilic cytoplasm containing coarse granules [Table/Fig-5,6]. The surrounding stroma was fibrous and showed reactive bone formation at periphery. Based on these histopathological features, a final diagnosis of mural unicystic ameloblastoma with diverse histopathology was given.
Orthopantamogram showing multilocular radiolucency with mixed radiographic pattern of honeycomb appearance interspersed with soap bubble pattern in right mandible.
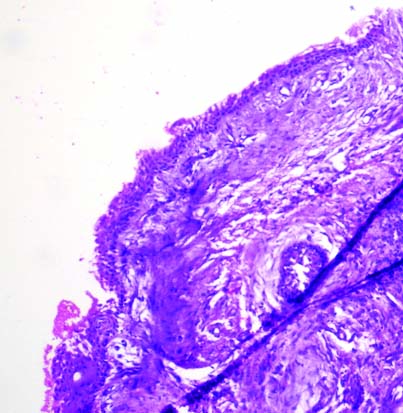
Photomicrograph showing cystic lumen lined ameloblastomatous epithelial lining. (Haematoxylin and eosin staining, 10X).
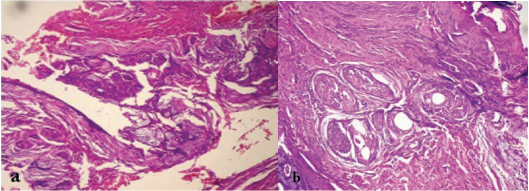
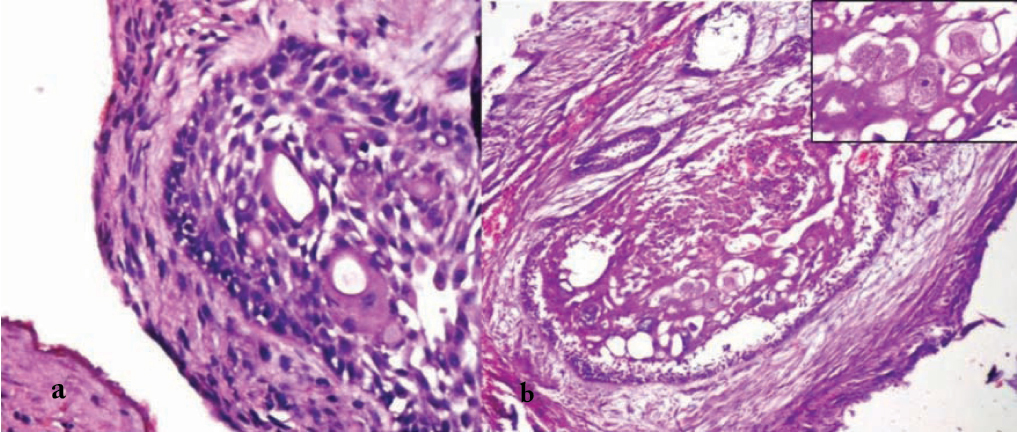
Photomicrograph showing lining with: a) luminal and; b) mural proliferation. (Haematoxylin and eosin staining, 10X).
Photomicrograph showing epithelial lining depicting basal cell layer of ameloblast like cells and upper layers resembling stellate reticulum with granular cell changes. (H&E staining, 20X).
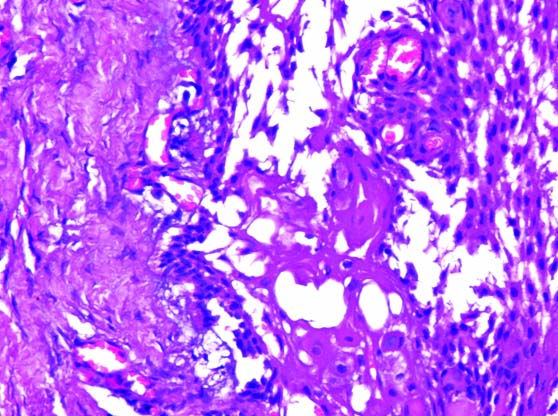
Photomicrograph showing ameloblastomatous islands in connective tissue with; a) squamous metaplasia and; b) granular cell change in central cells (H&E staining, 20X) Inset: showing granular cells with eosinophilic cytoplasm and coarse granules. (H&E staining, 40X)
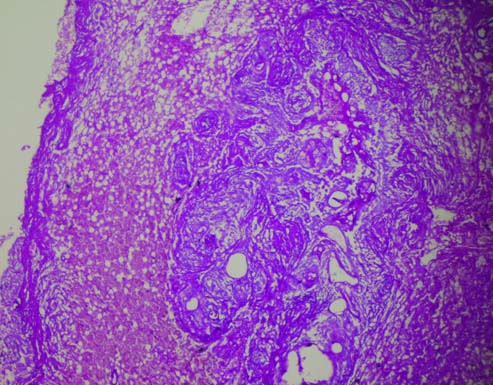
Photomicrograph showing ameloblastomatous islands in connective tissue with granular cell change in central cells in some islands. (PAS staining, 10X).
Discussion
Ameloblastomas are usually slow growing, persistent and locally invasive benign odontogenic tumours [1]. They can grow extensively with resultant bone deformities [2]. Solid multi cystic ameloblastoma is the commonest type with Unicystic Ameloblastoma (UA) accounting for only 5% to 15% of all intraosseous ameloblastomas [3]. Presence of two less common histopathological patterns, granular cell and acanthomatous together in a UA showing both luminal and mural proliferation is a rare occurrence. To our knowledge, only one such case of UA has been documented in literature [4].
Ameloblastomas are classified by World Health Organisation into four clinical categories, solid multicystic, unicystic, extraosseous and peripheral [5]. The majority present with classical histopathological features. However, they may sometimes present with interesting findings microscopically. In a study conducted on 108 ameloblastomas by Raubenheimer EJ et al., they found diverse clinicopathological findings in significant number of cases [6]. Such deviations from typical presentation seem to be more common with solid multi cystic type. UA, comprising of less number of cases, rarely presents with myriad of histopathological patterns. Ponce JB et al., presented a case of UA with multiple histopathological patterns, which they reported to be first such case in literature [4]. They observed all the three patterns of UA, along with acanthomatous, basal cells and granular cell variants and hyaline ring granulomas. In present case, an unexpected rare diverse histopathology in UA exhibiting luminal and mural types with acanthomatous and granular cell changes were observed. Although the occurrence of granular cells in conventional ameloblastomas has been reported by a number of authors, the granular cells in UA are not common [7,8]. These granular cells showed Periodic Acid Schiff (PAS) stain positivity giving a magenta colour. In the present case, the granular cell change was observed in both the lining as well as in the mural proliferations of ameloblastomatous epithelium whereas, acanthomatous changes were seen only in mural islands. The granular appearance is usually related to increased lysosomes within the cells. These may vary in size ranging from 1 μm to 30 μm in diameter. Many of them are small in size with rare presence of giant granules. The diverse shapes of these granules can also be seen depicting dif-ferent components and phases of digestion. They may appear as membranous structures, myelin figures, small particles, granules, vesicles, lattice structures, and crystalloids [9]. Formation of granules can be considered as an aging or degenerating process. With age, unnecessary components increase in the cytoplasm of some tumour cells with reduced ability of lysosomes to digest them with age, leading to their accumulation [10]. The authors suggest that granules can be due to the degenerative changes in the cytoplasm of tumour cells. That could be the one probable consideration. As the granular appearance can also be related to increased lysosomes which may result in lytic changes, so they could be an attribute to malignant behaviour.
UA’s with granular cell changes may exhibit rapid destructive growth, with higher incidence of malignancy and metastasis [9]. Ackermann classified UA into three groups that are, luminal (Group 1), Intraluminal or plexiform (Group 2) and Mural (Group 3). While Group 1 and 2 lesions may be treated by enucleation, Group 3 lesions should be treated aggressively [11]. Thus, histopathology plays a great role in correct histological diagnosis, categorization of this tumour and thus institution of appropriate therapy.
Conclusion
As UA’s with such varied histopathology are rare in literature, their course, clinical outcome, prognosis and recurrence rate are not clear. Documentation of more such cases may make pathogenesis and nature of these lesions more insightful. Research is required to correlate the prognosis of these lesions as compared to lesions with conventional histopathology.
[1]. R Thillaikarasi, J Balaji, B Gupta, V Ilayarja, NV Vani, B Saravanan, Cystic granular cell ameloblastomaJ Maxillofac Oral Surg 2010 9(3):310-13. [Google Scholar]
[2]. P Motahhary, A Etebarian, F Asareh, Granular cell type of a unicystic ameloblastoma: An unusual case and review of the literatureJ Oral Maxillofac Pathol 2014 18(2):331 [Google Scholar]
[3]. RS Ramesh, S Manjunath, TH Ustad, S Pais, K Shivakumar, Unicystic ameloblastoma of the mandible - an unusual case report and review of literatureHead Neck Oncol 2010 2:1 [Google Scholar]
[4]. JB Ponce, H Lima, M Rodrigues, F Souza, V Lara, Unusual histological patterns and hyaline ring granulomas in a unicystic ameloblastomaHippokratia 2014 18(1):83-85. [Google Scholar]
[5]. DG Gardner, K Heikinheimo, M Shear, HP Philipsen, H Coleman, Ameloblastomas. In: Barnes L, Eveson JW, Reichart P, Sidransky D (eds.). World Health Organization classification of tumour: pathology and genetics, head and neck tumoursTetracyclineTeratology 2005 Lyon, FranceIARC Press:296-300. [Google Scholar]
[6]. EJ Raubenheimer, WF van Heerden, CE Noffke, Infrequent clinicopathological findings in 108 ameloblastomasJ Oral Pathol Med 1995 24(5):227-32. [Google Scholar]
[7]. NA Abaza, L Gold, E Lally, Granular cell odontogenic cyst: a unicystic ameloblastoma with late recurrence as follicular ameloblastomaJ Oral Maxillofac Surg 1989 47(2):168-75. [Google Scholar]
[8]. SG Kim, HS Jang, Ameloblastoma: a clinical, radiographic, and histopathologic analysis of 71 casesOral Surg Oral Med Oral Pathol Oral Radiol Endod 2001 91(6):649-53. [Google Scholar]
[9]. TL Yogesh, SV Sowmya, Granules in granular cell lesions of the head and neck: a reviewInternational Scholarly Research Notes Pathology 2011 2011:215251 [Google Scholar]
[10]. M Nasu, M Takagi, H Yamamoto, Ultrastructural and histochemical studies of granular-cell ameloblastomaJ Oral Pathol 1984 13(4):448-56. [Google Scholar]
[11]. GL Ackermann, M Altini, M Shear, The unicystic ameloblastoma: a clinicopathological study of 57 casesJ Oral Pathol 1988 17(9-10):541-46. [Google Scholar]