Depression is a common psychiatric disorder, with symptoms such as change in appetite or weight, sleep and psychomotor activities, fatigue and loss of energy, which may appear decreasing social, educational and job related performances, feeling of worthlessness or guilt, thinking, concentrating or decision making problems, and thinking about or trying to commit a suicide, are from among other depression symptoms which are present in people, particularly students with intellectual activity, leads to a deficiency in education and employment, difficulty in completing tasks and reducing motivation to accomplish new schedule [1]. The prevalence of depression is different in societies [2]. In a comprehensive review, the prevalence of depression among university students in the world is estimated to be in the range of 10% to 85% [3]. Studies in Iranian student groups show a high prevalence of depression, it is estimated between 35-69% [4-7].
Many studies have shown that aerobic exercise is effective in the treatment of depression and improve mental health [8-12], the distraction or time out hypotheses explain the positive effects of exercise training. According to the distraction model, through the act of engaging in exercise, a psychological release is provided from the primary source of worry or depression. The distraction emphasize the negative automatic thoughts [13]. To examine the effect of aerobic exercise on depression and cognitive process, a number of testable models from Oie TP et al., were used.
It seems that the consequential model provides a better explanation for depression and aerobic exercise. Thus, in the present study firstly, we tested the hypothesis; the consequences model can explain the effect of non pharmaceutics treatments appropriately. Secondly, it has been attempted to investigate whether aerobic exercise is similar to the cognitive behavioural therapy or not, thus, we used all four Oie's models in this study to find the best explanation and we then looked for the best model to explain the data.
The current study was carried out to determine the effectiveness of group aerobic exercise on depression, automatic thoughts and dysfunctional assumptions and finally, testing cognitive changes during aerobic exercise on depression.
Materials and Methods
This study was conducted through structural equation modeling; the study sample included 85 depressed students of the Kermanshah University of Medical Sciences. Participants were selected through purposive sampling method. Subsequent to the structured interview, participants signed a statement of informed consent informing them of their freedom to withdraw at any time.
The inclusion criteria required the depression score in the BDI-II between 14 and 28 (mild and moderate depression) and diagnosed depressive disorder based on the Structured Clinical Interview for DSM Disorders (SCID-I), willingness to participate in aerobic exercise (by signing the informed consent). The exclusion criteria included participants with other disorders in the axis I (other than depression), the depression episode was attributable to the physiological effects, psychotic symptoms such as hallucinations and delusions, drug abuse or drug dependence, suicidal thought or severe depression, at the same time, receiving psychiatric treatment or psychotherapy (patients should not receive psychological treatment or medication at least six months before research).
Participants
Eighty five participants (48 males and 37 females, with an average age of 21.81±3.25) engaged in eight sessions of aerobic exercise. Participants were screened according to BDI, and diagnosed depressive disorder based on the SCID-I. They were randomly allocated to two parallel groups, an experimental group (37 subjects) and a control group (48 subjects), and each individual was chosen randomly and entirely by chance (simple randomization). The experimental group received eight sessions of aerobic exercise (three times a week), while the control group received no treatment, (it is noticeable that we used 85 participants for assessing the effects of group aerobic exercise on depression and it's cognitive components in experimental and control groups, and we used 37 participants (experimental group) for comparing the competing models through Structural Equation Modeling (SEM) path analyses). The data were gathered before and after the intervention. To prevent bias, screening and evaluation of participants during the course of treatment are done by a different person with clinical psychology education, in order to blind on the accumulating data on participants’outcomes. Aerobic exercises were conducted by professors of physical education and screening, clinical interview and evaluation of participants were conducted by MA in Clinical Psychology. The study took place at the health clubs of Kermanshah University of Medical Sciences, Iran from January 2016 to April 2016.
Measurement
Structured Clinical Interview for the DSM (SCID): Structured Clinical Interview is a structured interview based on DSM-IV. In Iran, the Persian version of SCID was studied by Sharifi V et al., A kappa coefficient was 0.6 and general agreement (kappa total) for all current diagnosis was 0.52% [15].
Beck Depression Inventory (BDI-II): The BDI is a 21 question self report inventory. The BDI is consistent with the criteria for depression base on the diagnostic and statistical manual of mental disorders. BDI-II is positively correlated with the Hamilton depression rating scale (r=0.71), which is showing a good agreement, and it had also shown a high one week test retest reliability (alpha coefficient=0.91) [16].
The Automatic Thoughts Questionnaire: The questionnaire was developed in 1980 by Hollon SD and Kendall PC [17]. The ATQ measures depressogenic thought frequency and the believability. Internal consistency is between 0.96 and 0.97 [18]. Nazary GH et al., reported the Cronbach's alpha and test retest coefficients 0.96 and 0.84 respectively [19].
The Dysfunctional Attitudes Scale-40 items version: The DAS is self report inventory designed to measure irrational beliefs. Clak DA and Beck AT et al., reported the reliability of 0.89 and more for the forms A and B. The correlation between the two tests was reported to be more than 0.81 [20]. Internal consistency, test retest reliability revealed the reliability coefficient of 0.87 [21].
Aerobic Exercise Protocol
Aerobic exercise session was made of the following: before starting each session, participants had to be at the college campus 30 minutes sooner to be taught how to measure radial and carotid pulse and to have enough preparation for them. In order to be sure of the aerobic nature of the exercise, the heart rates were measured. Each exercise session contained following: measuring and recording resting heart rate before starting by the carotid or wrist pulse, beginning with warm-up exercises, stretching, breathing, meditation and primary respiration. Usually, the movements start from the head, neck or legs and persistent with running in place. This phase took about 10 minutes. At that moment, the movements were continuous with more intensity. The average intensity of movements was 0.60-0.80 heart rate. This phase was quicker with gestures and activities of the hands and feet separately, one way, two way, and cross legs. At this phase, the heart rate was measured and recorded by radial or carotid pulse. Time of this period was 30 to 35 minutes. The final phase was the cooling down phase with less intensity; take long for nearly 10-15 minutes (Aerobic exercise sittings were conducted under the administration of a sports expert).
Data Analysis
The statistical analysis was performed using SPSS & AMOS. For normal distribution of quantitative data, Kolmogorov-Smirnov test; for the homogeneity of variances, the leven's test; for the comparison between groups, Analysis of Covariance (ANCOVA) and to compare the competing models, SEM path analyses were used. Comparisons were done on the basis of achieving a range of minimum fit indices. The subjects suffering from severe depression were referred to the psychiatrist for treatment. It should be noted that the tasks of the therapy and the evaluation were separately performed by two individuals.
Results
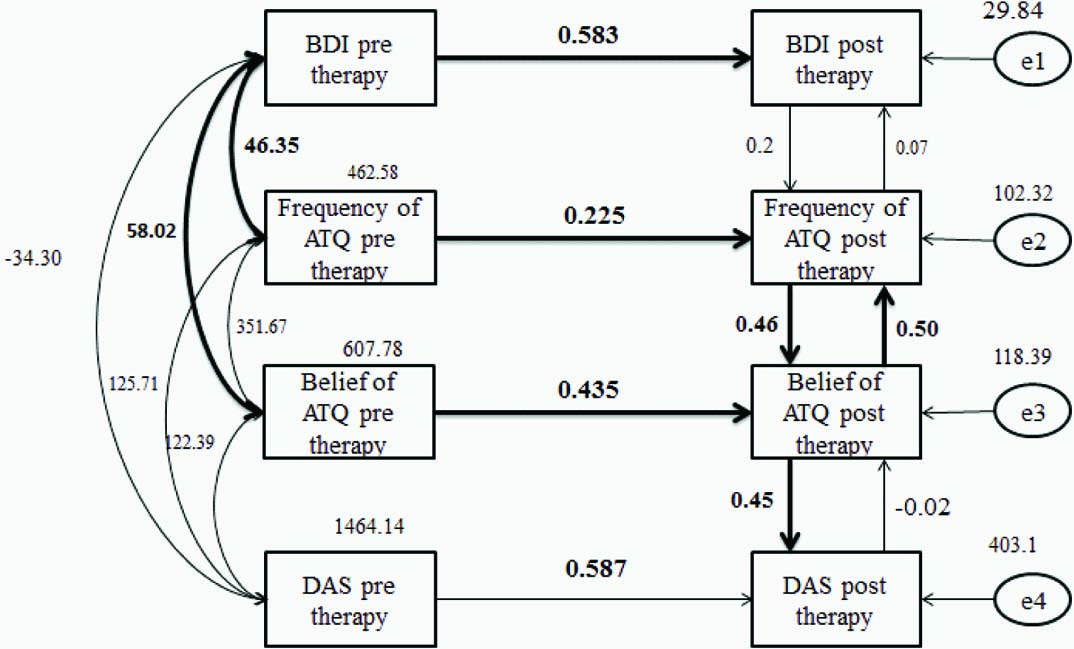
The means at pre test to post test for the four variables are shown in [Table/Fig-5], analysis of covariance showed that there was a significant difference at post test in an adjusted average of depression score in the experimental group and the control group (p=0.001). The automatic thought and dysfunctional assumption was not significantly different at pre test to post test. The findings showed that the casual and consequential models were not fit to the data and partially and fully interactive models provided an adequate fit to the data [Table/Fig-6]. The fit indices for the partial interactive model [Table/Fig-7] and fully interactive model [Table/Fig-8] were indicating a mutual relationship and feedback. This means, a reduction in negative thinking decreases depression and a reduction in depressed feelings decreases negative thinking.
Descriptive statistics and ANCOVA for depression and cognitive components.
| Variables | Groups | Post test | Pre test | Mean Square | F | Sig |
|---|
| Mean ± SD | Mean ±SD |
|---|
| Depression | Aerobic exercise | 20.28±6.42 | 12.04±7.53 | 466.79 | 12.39 | 0.001 |
| Control | 23.77±8.74 | 21.33±9.98 |
| Automatic thoughts (frequency) | Aerobic exercise | 69.52±22.99 | 60.90±22.55 | 201.65 | 0.683 | 0.413 |
| Control | 71.03±23.92 | 61.11±24.73 |
| Automatic thoughts (beliefs) | Aerobic exercise | 70.62±29.15 | 62.57±25.20 | 48.46 | 0.178 | 0.676 |
| Control | 73.37±23.03 | 66.23±21.93 |
| Dysfunctional assumption | Aerobic exercise | 173.80±36.91 | 166.90±25.30 | 674.24 | 1.55 | 0.219 |
| Control | 172.77±27.03 | 174.42±25.10 |
Goodness of fit indices for causal, consequential and interactive models.
| Indices | χ2 | p | GFI | NFI | CM/df | TLI | RMSEA | AGFI | CFI | RFI | Hoelter |
|---|
| Min. | | >0.05 | >0.90 | >0.90 | >0.90 | <2.5 | >0.90 | <0.10 | >0.90 | >0.90 | >200 |
| Good | >0.95 | >0.95 | <0.05 | >0.95 | >0.95 |
| Model |
| 1 | 42.27 | 0.001 | 0.795 | 0.709 | 4.22 | 0/455 | 0.299 | 0.426 | 0.740 | 0.389 | 16 |
| 2 | 51.66 | 0.001 | 0.715 | 0.480 | 10.23 | 0/044 | 0.509 | 0.145 | 0.478 | 0.044 | 8 |
| 3 | 10.47 | 0.574 | 0.940 | 0.940 | 0.87 | 1.024 | 0.001 | 0.819 | 1.000 | 0.859 | 73 |
| 4 | 2.78 | 0.836 | 0.981 | 0.984 | 0.46 | 1.103 | 0.001 | 0.889 | 1.000 | 0.925 | 163 |
GFI=Goodness-of-Fit Index, NFI=Normed Fit Index, CM/Df=Minimum Discrepancy Divided By The Degrees Of Freedom, TLI=Tucker-Lewis Index, RMSEA=Root Mean Square Error Of Approximation, AGFI=Goodness-Of-Fit Index Adjusted For Degrees Of Freedom, CFI=Comparative Fit Index, RFI=Relative Fit Index And Hoelter=Adequacy Of Sample Size. Min=Minimum Required For An Adequate Fit, Good=Good To Superior Fit. 1=Causal, 2=Consequential, 3=Partially Interactive And 4=Fully Interactive Models.
Partially interactive model, in this model GFI=0.94, p=0.57, χ2=10.47,NFI= 0.94,CFI=1and RMSEA=0.001, which represents a good model fit. It means that a reduction in negative thinking reduces depression and a reduction in depressed feelings reduces negative thinking and the relationship between negative thinking.
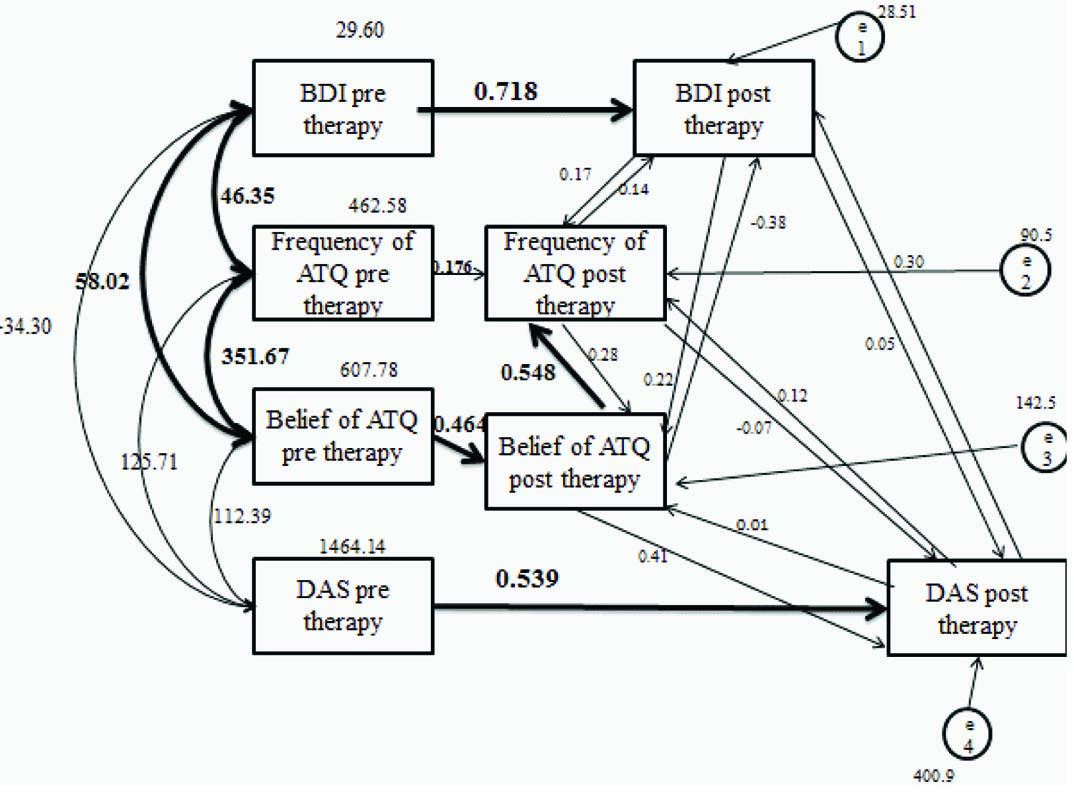
Fully interactive model, in this model, GFI=0.98, p=0.83, χ2=2.78,NFI=0.98, CFI= 1 and RMSEA=0.001, which represents a goodmodel fit. It seems that fully interactive model provided the best fit of the data and aerobic exercise affects separately on depression, automatic thoughts, and dysfunctional assumptions and there is no relevant path.
Four models were reviewed to understand the effect of aerobic exercise on depression. These four models included: the casual, consequential, partial and fully interactive models [Table/Fig-6]. Results for the casual and the consequential models were not significant, but the results for the partial and the fully interactive models were significant. For scrutinizing each model, the scores obtained for χ2, NFI, CFI, and RMSEA indices should be considered. The Chi-Square value is the traditional measure for evaluating overall model fit and, ‘assess the magnitude of discrepancy between the sample and fitted covariances matrices’. A good model fit would provide an insignificant result at a 0.05 threshold [22].
Indicators for the casual model was (χ2=42.272, p=0.001), NFI =0.7, CFI=0.74, RMSEA=0.29 and for the consequential model was (χ2 =51.66, p=0.001), NFI=0.48, CFI=0.47, RMSEA=0.50. The χ2 change is not significant for casual and consequential models (p=0.001). The χ2 change is acceptable if more than 0.05 (p>0.05). Other indicators, such as CFI and NFI fit are acceptable if more than 0.95 and for the RMSEA is acceptable if less than 0.08. So the casual and consequential models do not provide good fit to data. [Table/Fig-6].
Discussion
The hypothesis that the symptoms of depression, automatic thoughts and dysfunctional assumption reduced during aerobic exercise was confirmed and supported by previous studies [3,5,6,23,24], explaining these findings; some factors were influenced, one is biological processes, studies showing that exercising could change the doping of neurotransmitter, therefore, physical exercise might be a therapeutic strategy in treating depression because of discharge of neurotransmitters [1]. This is compatible with the findings of Sadeghi K et al., which showed that aerobic exercise reduces students' depression, and also showed that aerobic exercise can reduce the frequency and the belief of automatic thoughts in the pre test and post test. It could be argued that the discrepancy may exist because only male sample had been used in Sadeghi K et al., study, however, the present study conducted to investigate the effectiveness of aerobic exercise on both male and female students with larger sample size [25].
The results showed that aerobic exercise reduces automatic thoughts and dysfunctional assumptions, but was not statistically significant; explaining these findings, it could be argued that aerobic exercise causes a distraction than a source of concern. According to the distraction model, through the act of engaging in exercise, a psychological release is provided from the primary source of worry or depression [26]. About this finding it could be argued that automatic thought and dysfunctional beliefs are rooted in the dysfunctional assumption and schemas [27]. Since there is no intervention for changing beliefs, it is expected that there was no difference in treatment and control groups.
The other aim involved testing cognitive changes during aerobic exercise on depression, as shown in [Table/Fig-1], this study showed that aerobic exercise significantly reduced depression, as well as reduced cognitive component of depression, but this reduction was not statistically significant. Considering the correlation between depression and cognitive components, it seems that the consequential model would better explain the data. That is, aerobic exercise reduce depression and cognitive components. However, we used path analysis to examine our hypothesis which showed that casual and consequential models were not fit to data and partially and fully interactive models were fit to data [Table/Fig-7,8]. This study shows that aerobic exercise has separate effects on depression, automatic thoughts, and dysfunctional assumptions and there is no relevant path. So we can say, that aerobic exercise is effective in reducing depression and cognitive components but does not follow a particular pattern or model. It seems that aerobic exercise reduces automatic thoughts which reducing automatic thoughts consequently lead to reduce dysfunctional assumptions [Table/Fig-8], but there is not cause relation in casual and consequential models.
In [Table/Fig-2], it is assumed that the consequential models would provide a superior fit to the data which this hypothesis did not confirm, and the fully interactive model provided a superior fit to the data [Table/Fig-8], which indicates that the relationship between negative thinking and depression may be bidirectional. That is, a reduction in negative thinking reduces depression and a reduction in depressed feelings reduces negative thinking, in other words, an interactive process. This finding is interesting and consistent with the clinical observations and literature.
Limitation
In present study, sample size was limited. In structural equation modeling we need more sample size to test the model fitness. It would be better if the study was conducted on more depressed students. The concomitant variable should be specified for ANCOVA analysis. These limitation needs to be overcome in future studies.
Conclusion
This study tested a number of testable models based on Beck's cognitive theory of depression in depressed students. The results showed that fully interactive model provided a superior fit to data, and it seems that aerobic exercise reduces cognitive components separately which consequently leads to depression reduction.
GFI=Goodness-of-Fit Index, NFI=Normed Fit Index, CM/Df=Minimum Discrepancy Divided By The Degrees Of Freedom, TLI=Tucker-Lewis Index, RMSEA=Root Mean Square Error Of Approximation, AGFI=Goodness-Of-Fit Index Adjusted For Degrees Of Freedom, CFI=Comparative Fit Index, RFI=Relative Fit Index And Hoelter=Adequacy Of Sample Size. Min=Minimum Required For An Adequate Fit, Good=Good To Superior Fit. 1=Causal, 2=Consequential, 3=Partially Interactive And 4=Fully Interactive Models.