Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) are currently the most commonly prescribed drugs for treating pain and inflammation. They are indeed effective in managing painful inflammatory conditions like osteoathritis, ankylosing spondylitis, rheumatoid arthritis etc. However, they cause a number of side effects. The traditional NSAIDs usually cause gastrointestinal adverse effects on long term use and the selective Cyclooxygenase (COX2) inhibitors are known to possess dangerous cardiotoxic potential [1].
Opioid analgesics are the other group of drugs used for pain management with good effect. However, in patients with chronic pain opioids are rather avoided due to its addiction liability and abuse potential [2].
Researchers have been exploring various avenues to develop an ideal analgesic which is non-toxic as well as effective at the same time. A commonly used antiepileptic drug, sodium valproate has been used in various non-epileptic conditions like migraine prophylaxis and in the treatment of bipolar disorder because of the multiple mechanisms by which it acts [3]. Sodium valproate is an inhibitor of Histone Deacetylation (HDAC). Rat stroke models in the past have demonstrated the neuro-protective effect of valproate due to HDAC inhibition [4].
Fish oils contain omega-3 fatty acids (eicosapentanoic acid and DHA). They have been shown in the past to reduce risk of developing conditions like hypertension, cardiac disease and cancer. They compete with arachidonic acid for enzymes like lipo-oxygenase and COX2 as a result inflammatory mediators are not formed. One more point to be noted is that they are natural products and are therefore unlikely to cause adverse effects when compared to the traditional drugs used to treat pain [5].
In view of these existing reports we initiated a study to evaluate the analgesic potential of sodium valproate and DHA supplementation using various experimental models in albino Wistar rats.
Materials and Methods
Study Design
An in vivo experimental study conducted in the Department of Pharmacology, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
Selection and Animal Handling
Forty eight male albino Wistar healthy rats were selected for this study, which were locally bred in the Central Animal House of Manipal University, Manipal. These animals weighed 150 g to 200 g and they were around six months old, and were housed under controlled conditions with temperature of about 23±2°C, 50±5% humidity and 10-14 hour of light and dark cycle respectively. These animals were individually housed in poly propylene cages which contained paddy husk (procured locally) which was sterile, as bedding throughout the study and had easy access to animal chow (sterile food) and water ad libitum. This study was initiated after taking approval from the Institutional Animal Ethics Committee (IAEC/KMC/75/2014 dated August 22, 2014). The experiments were conducted in accordance to CPCSEA guidelines.
Identification of Individual Animals
Rats from each treatment group were marked using different colored marks on their tails, for easy identification and experimentation, according to the group allotted.
Sample Size
The minimum number of rats in each group was kept as six, so as to obtain statistically significant results within and between the groups.
Drugs, Reagents and Other Materials
Three drugs were used during the study; tramadol (Torrent Pharmaceuticals Ltd.), sodium valproate (Zydus Pharmaceuticals) and docosahexaenoic acid (Solvey Pharma India Ltd.) were used. The pure powder form was used, dissolved in distilled water. Eddy’s hot plate and tail flick analgesiometer were used in the Department of Pharmacology, KMC, Manipal.
Evaluation of Analgesic Activity
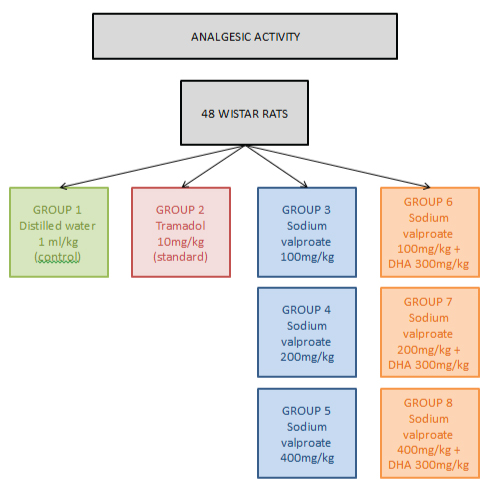
A total of 48 adult Wistar albino rats were divided into eight groups. Each group contained six rats. They were weighed and marked. Group I was control (distilled water 1 ml/kg), Group II received intraperitoneal injection of tramadol (10 mg/kg), Group III, IV, V were injected intraperitoneal sodium valproate 100, 200, 400 mg/kg dissolved with distilled water and Group VI, VII, VIII were given sodium valproate 100, 200, 400 mg/kg dissolved with distilled water along with DHA 300 mg/kg (intraperitoneal) respectively [Table/Fig-1]. The dose of sodium valproate was chosen as 100 mg/kg, 200 mg/kg and 400 mg/kg based on a study performed by Raza M et al., [6]. The dose of DHA was chosen as 300 mg/kg based on a study done by Gao J et al., [7].
Hot Plate Method
The hot plate is an electrically heated surface which is commercially available. It can be a heated glass or copper surface maintained at around 55°C. At this temperature, rats feel heat as their paws are quite sensitive [8].
The albino Wistar rats were weighed and marked. Each rat was placed on the Eddy’s hot plate. The plate was maintained at 55±1°C. Licking of the hind paws, rotational movements or jumping were noted as withdrawal latency at baseline that is just before administering the drug, and at 15th, 30th, 60th and 120th minute post administration of the drug [9]. The time from placing the rat on the hot plate till the occurrence of responses was recorded using a stop watch. An increase in the time interval of withdrawal latency was indicative of analgesic activity. In order to avoid injury to the tissue a cut off of 60 seconds was set [10].
Tail Flick Method
Analgesia was measured using tail flick method also called the modified D Amour and Smith method [11]. The albino Wistar rats were weighed and marked. The analgesic response was checked by measuring the latency of the response (tail flick) with the help of tail flick test. The Wistar rats were held gently and their tails were placed on an analgesiometer. The tail flick response were recorded at baseline just before administering the drug followed by 15th, 30th, 60th, 90th and 120th minute post administration of the drug by giving radiation heat using a heated nichrome wire at 1 cm – 1.5 cm from the tail tip at the dorsal surface. Withdrawal latency is then recorded as the time between placing the rat tail on the heat source till the sudden sharp tail withdrawal. In order to protect tail from thermal injury, a cut off time is set at 10 seconds while checking the tail flick reaction time [12].
Acetic Acid Induced Writhing Method
This test is a type of chemical pain /nociceptive test and the principle is based on irritant induced peritonitis production. About 12 hours prior to the test, food was withdrawn and no food was given till the completion of the test [11].
The albino Wistar rats were weighed and marked. A 2% acetic acid was injected intraperitoneally in order to produce writhing in the Wistar rats about 30 minutes after the administration of the drug to be tested. Ten minutes post administration of 2% acetic acid writhing movements like elongation of body, abdominal constriction, trunk twisting, forelimb extension, hind limb extension and back arching were counted cumulatively for a period of 20 minutes [13].
Statistical Analysis
The data obtained were analysed using IBM statistical package for social sciences (SPSS) version 22.0. The results were expressed as Mean±SEM (Standard Error of Mean). The significance difference within the groups at different end points was assessed using repeated measures One-Way Analysis of Variance (ANOVA). Similarly, the significances differences between the various groups was checked for using ANOVA, followed by post-hoc Tukey’s test. Importantly, all test groups were compared against the control and standard groups, to arrive at a conclusion regarding the results. A p-value of <0.05 was considered to be statistically significant.
Results
1. Hot Plate Model
The pain reaction time was significantly increased to 10.22±0.35 (p<0.001) in the tramadol (10 mg/kg) treated group, 10.09±0.88 (p<0.001) in sodium valproate (400 mg/kg) group, 10.57±1.3 (p<0.001) in the sodium valproate (200 mg/kg) plus DHA (300 mg/kg) group and 11.15±1.26 (p<0.001) in the sodium valproate (400 mg/kg) plus DHA (300 mg/kg) group at 60 minutes when compared to control (3.39±0.27) as shown in [Table/Fig-2].
| Groups | Retention Time at Different Time Points (in seconds) |
|---|
| 0 min | 15 min | 30 min | 60 min | 90 min | 120 min |
|---|
| Control | 3.25±0.31 | 3.51±0.26 | 3.52±0.26 | 3.39±0.27 | 3.67±0.29 | 3.58±0.31 |
| Tramadol 10 mg/kg (std) | 6.35±0.59 | 6.93±0.58a | 8.48±0.49a | 10.22±0.35ab | 13.02±0.39ab | 15.57±0.53ab |
| *Val 100 mg/kg | 6.45±0.90 | 6.61±1.21 | 6.6±2.07 | 5.57±0.48c | 5.66±1.04c | 6.61±0.94c |
| *Val 200 mg/kg | 5.72±0.86 | 6.05±0.91 | 6.37±0.95 | 6.47±0.82c | 6.14±1.04c | 6.13±1.0c |
| *Val 400 mg/kg | 5.88±1.38 | 6.54±1.33 | 8.23±1.36 | 10.09±0.88ab | 11.37±1.04ab | 14.13±1.02ab |
| *Val 100 mg/kg +DHA 300 m/kg | 4.35±0.72 | 4.64±0.5 | 4.87±0.5 | 5.12±0.42c | 5.65±0.49c | 5.84±0.4c |
| *Val 200 mg/kg +DHA 300 mg/kg | 4.13±0.19 | 5.31±0.30 | 6.50±0.57 | 10.57±1.3ab | 10.79±1.24ab | 11.43±1.16b |
| *Val 400 mg/kg +DHA 300 mg/kg | 6.04±0.48 | 7.96±1.16 | 9.5±1.15 | 11.15±1.26b | 13.01±1.04ab | 15.42±0.80ab |
All values are expressed as Mean±SEM.
a denotes p<0.05 compared to baseline, b denotes p<0.05 compared to control, and c denotes p<0.05 compared to standard
p-value obtained by one-way ANOVA followed by Post-Hoc Tukey’s test, *Val: sodium valproate
The pain reaction time was significantly increased to 13.02±0.39 (p<0.001) in the tramadol (10 mg/kg) treated group, 11.37±1.04 (p<0.001) in sodium valproate (400 mg/kg) group, 10.79±1.24 (p<0.001) in the sodium valproate (200 mg/kg) plus DHA (300 mg/kg) group and 13.01±1.04 (p<0.001) in the sodium valproate (400 mg/kg) plus DHA (300 mg/kg) group at 90 minutes when compared to control (3.67±0.29) as shown in [Table/Fig-2].
The pain reaction time was significantly increased to 15.57±0.53 (p<0.001) in the tramadol (10 mg/kg) treated group, 14.13±1.02 (p<0.001) in sodium valproate (400 mg/kg) group, 11.43±1.16 (p<0.001) in the sodium valproate (200 mg/kg) plus DHA (300 mg/kg) group and 15.42±0.80 (p<0.001) in the sodium valproate (400 mg/kg) plus DHA (300 mg/kg) group at 120 minutes when compared to control (3.58±0.31) as shown in [Table/Fig-2].
2. Tail Flick Model
The tail flick time or withdrawal response was significantly increased to 9.15±0.18 (p<0.001) in the tramadol (10 mg/kg) treated group, 8.45±0.42 (p<0.001) in the sodium valproate (400 mg/kg) group and 9.07±0.23 (p<0.001) in the sodium valproate (400 mg/kg) group plus DHA (300 mg/kg) group at 120 minutes when compared to control (5.15±0.31) as shown in [Table/Fig-3].
| Groups | Retention Time at Different Time Points (in seconds) |
|---|
| 0 min | 15 min | 30 min | 60 min | 90 min | 120 min |
|---|
| Control | 5.03±0.3 | 5.18±0.33 | 5.37±0.22 | 5.30±0.38 | 5.28±0.21 | 5.15±0.31 |
| Tramadol 10 mg/kg (std) | 3.48±0.24 | 4.67±0.42 | 5.58±0.37a | 6.48±0.48a | 7.75±0.34ab | 9.15±0.18ab |
| *Val 100 mg/kg | 5.47±0.85 | 5.43±0.65 | 5.72±0.81 | 6.10±0.67 | 5.62±0.70c | 5.93±0.58c |
| *Val 200 mg/kg | 5.17±0.55 | 5.23±0.65 | 5.32±0.54 | 5.50±0.61 | 5.45±0.52c | 5.40±0.54c |
| *Val 400 mg/kg | 4.33±0.47 | 4.77±0.43 | 5.42±0.43 | 6.20±0.29 | 7.35±0.40b | 8.45±0.42ab |
| *Val 100 mg/kg +DHA 300 mg/kg | 3.32±0.29 | 4.45±0.49 | 4.87±0.34 | 5.77±0.59c | 5.29±0.32c | 5.06±0.40c |
| *Val 200 mg/kg +DHA 300 mg/kg | 4.32±0.43 | 4.20±0.36 | 4.86±0.20 | 5.10±0.33 | 5.17±0.34c | 5.25±0.33c |
| *Val 400 mg/kg +DHA 300 mg/kg | 3.87±0.21 | 4.30±0.26 | 5.03±0.50 | 6.32±0.34a | 7.56±0.35ab | 9.07±0.23ab |
All values are expressed as Mean±SEM.
a denotes p<0.05 compared to baseline, b denotes p<0.05 compared to control and c denotes p<0.05 compared to standard
p-value obtained by one-way ANOVA followed by Post-Hoc Tukey’s test, *Val: sodium valproate
The tail flick time or withdrawal response was significantly increased to 7.75±0.34 (p=0.008) in the tramadol (10 mg/kg) treated group, 7.35±0.40 (p=0.041) in the sodium valproate (400 mg/kg) group and 7.56±0.35 (p=0.018) in the sodium valproate (400 mg/kg) group plus DHA (300mg/kg) group at 90 minutes when compared to control (5.28±0.21) as shown in [Table/Fig-4].
Acetic acid writhing model.
| Groups | Writhing response |
|---|
| Control | 34.5±4.4 |
| Tramadol 10 mg/kg (std) | 5.33±0.62b |
| *Val 100 mg/kg | 31.17±2.02c |
| *Val 200 mg/kg | 22.83±2.81bc |
| *Val 400 mg/kg | 8.33±1.75b |
| *Val 100 mg/kg + DHA 300 mg/kg | 30.5±1.18c |
| *Val 200 mg/kg + DHA 300 mg/kg | 19.17±1.22bc |
| *Val 400 mg/kg + DHA 300 mg/kg | 6.67±1.31b |
All values are expressed as Mean±SEM.
b denotes p<0.05 compared to control and c denotes p<0.05 compared to standard p-value obtained by one-way ANOVA followed by Post-Hoc Tukey’s test *Val: sodium valproate.
3. Acetic Acid Writhing Model
The number of abdominal constrictions or writhing were significantly reduced to 5.33±0.62 (p<0.001) in the tramadol (10 mg/kg) treated group, 22.83±2.81 (p=0.013) in the sodium valproate (200 mg/kg) group, 8.33±1.75 (p<0.001) in the sodium valproate (400 mg/kg) group, 19.17±1.22 (p<0.001) in the sodium valproate (200 mg/kg) plus DHA (300 mg/kg) group and 6.67±1.31(p<0.001) in the sodium valproate (400 mg/kg) plus DHA (300 mg/kg) group when compared to control (34.5±4.4) as shown in [Table/Fig-4].
Discussion
Analgesics are common medications which relieve pain of multiple aetiologies with no effect on the level of consciousness of the patient. They interfere with the mode of transmission of the pain message. The present study was carried out using different experimental pain models to evaluate analgesic activity of sodium valproate and DHA. The analgesic activity in our experiment was checked using hot plate, tail flick and acetic acid writhing models which are standard models for screening agents for analgesic activity.
In the hot plate model sodium valproate 400 mg/kg, combination of sodium valproate 200 mg with 300 mg of DHA and combination of sodium valproate 400 mg with 300 mg DHA showed significant analgesic activity compared to control at 60 minutes, 90 minutes and 120 minutes. In the tail flick model, sodium valproate given at 400 mg and combination of sodium valproate 400 mg with 300 mg of DHA showed significant analgesic activity when compared to control at 90 and 120 minutes. In the acetic acid Writhing model, sodium valproate given at a dose of 200 mg, sodium valproate given at a dose of 400 mg, combination of sodium valproate 200 mg with 300 mg of DHA and combination of sodium valproate 400 mg with 300 mg of DHA showed significant analgesic activity as compared to control. Mesdjian E et al., in 1983 reported that sodium valproate possessed analgesic activity when used alone [14]. Similarly Nakamoto K et al., in 2010 reported that DHA when used alone possessed analgesic activity [15]. But the co-administration of DHA along with sodium valproate has potentiated the analgesic activity of the later.
The analgesic activity of sodium valproate can be attributed to the increase in glutamate transporters like glial Glutamate Transporter 1 (GLT 1) and Glutamate Aspartate Transporter (GLAST), in dorsal horn of the spinal cord and also in the hippocampus. This action of sodium valproate is due to inhibition of histone deacetylation [16]. Ximenes JCM et al., attributes the analgesic activity of sodium valproate to its effect on GABA neurotransmission. Sodium valproate is said to increase the GABA neurotransmission causing analgesia [17].
Similar to sodium valproate, DHA too modulates the glutamate transporters. It is said to increase GLT 1. When supplemented by DHA, the synaptic activity in the neurons is increased which is attributed to the enhanced glutaminergic activity [18]. Another study done by Mas E et al., attributes the analgesic activity of DHA to increased resolvin and neuroprotectin levels [19]. This may be the probable reason for potentiating the analgesic activity of sodium valproate by DHA.
Limitation
Only one dose of DHA was used in the last three groups. So, we don’t know whether the effects show dose dependence. The mechanisms by which sodium valproate and DHA showed analgesic activity was not studied. Mechanisms mentioned in previous studies were considered instead.
Conclusion
In conclusion, the combination of sodium valproate and DHA has shown promising analgesic activity and was almost comparable to standard drugs used in this study. A well planned clinical trial using this combination may be worthwhile to evaluate the possibility of its therapeutic uses in various painful and inflammatory conditions.