Jejunal Gastric Heterotopia causing Multiple Strictures and Perforation Peritonitis- A Case Report with Review of Literature
M Vani1, Ajit Nambiar2, K Geetha3, BYJU Kundil4
1 Associate Professor, Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
2 Associate Professor, Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
3 Professor and Head, Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
4 Associate Professor, Department of Gastrosurgery, Academy of Medical Sciences, Pariyaram, Kannur, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M Vani, Associate Professor Department of Pathology, Academy of Medical Sciences, Pariyaram, Kannur-670503, Kerala, India.
E-mail: vanim250180@gmail.com
Gastric heterotopias beyond the ligament of Treitz though rare, should be thought of in the differential diagnosis of polypoid lesions presenting with gastrointestinal bleed or obstructive symptoms especially in children and in the young. Here is a 24-year-old male with multifocal jejunal gastric heterotopias causing multiple strictures and perforation peritonitis. Patient presented with acute abdomen pain and an emergency laparotomy was performed revealing jejunum with multiple strictures and perforation, followed by jejunal resection. On gross examination polypoid mucosa was noted at the stricture sites which showed heterotopic gastric mucosa on microscopy. Jejunal gastric heterotopias are extremely rare with less than ten reported cases and those presenting with multiple strictures are even rarer. To our knowledge this is the second case of jejunal gastric heterotopia presenting with multiple strictures.
Jejunum, Obstruction, Polypoid
Case Report
A 24-year-old male reported to the gastrosurgery casualty with acute onset of abdominal pain. On general examination the patient was febrile and abdominal examination showed guarding and tenderness. Routine blood investigation reports were normal except for a mild neutrophilia. Ultrasonography of the abdomen revealed perforation peritonitis and an emergency exploratory laparotomy was performed. Peroperatively, jejunum showed multiple strictures and perforation. Jejunal resection was done and was sent for histopathological examination.
Resected specimen showed jejunal segment 40 cm long with multiple strictures and serosal exudate. Mucosa at the site of strictures appeared polypoidal [Table/Fig-1]. Histopathological examination revealed a clear transition from jejunal to gastric type epithelium in the polypoid mucosa at all stricture sites [Table/Fig-2]. The gastric glands were predominantly of pyloric type. Ulceration of gastric type mucosa at stricture site was seen. Mucosal congestion, prominent muscularis mucosa, chronic inflammation, fibrosis and serosal exudates were also seen [Table/Fig-3]. Intervening jejunal mucosa appeared normal except for mild mucosal congestion. Mucin histochemistry by alcian blue technique showed positive staining in jejunal mucosa and absence of staining in polypoid mucosa at stricture site confirming it to be gastric type foveolar epithelium which contains neutral mucin [Table/Fig-4]. Our patient was doing well after six months of follow up.
Resected segment of jejunum with multiple strictures.

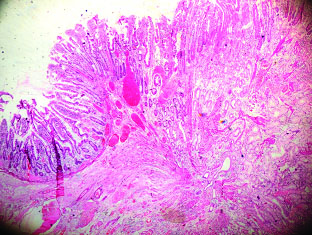
Clear transition from jejunal to gastric type mucosa in polypoid mucosa at stricture site.(H&E; 4X).
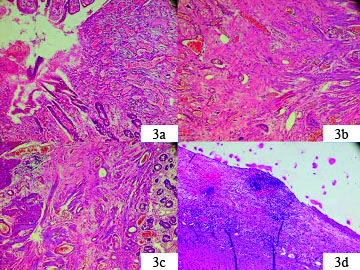
a) Heterotopic mucosa with ulceration and congestion; b) Fibrosis and chronic inflammation; c) Prominent muscularis mucosa; d) Serosal exudate (all from stricture sites) (H&E-10X).
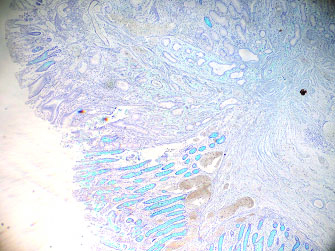
Jejunal mucosa shows positivity for alcian blue. Note the absence of staining in heterotopic gastric mucosa (alcian blue 4X).
Discussion
Heterotopia is defined as the presence of mature tissue in a location in which it is not normally seen. Gastric heterotopias are not uncommon lesions and can occur anywhere in the gastrointestinal tract. But they are rare beyond the duodenum except for its frequent association with Meckel’s diverticulum [1]. Patients may be asymptomatic or may present with gastrointestinal bleeding due to peptic ulceration or with obstructive symptoms [2,3]. Gross appearance is that of a mucosal nodularity or a polypoid lesion [4,5]. Peptic ulceration at the heterotopic focus with subsequent inflammation and fibrosis can lead to stricture formation [6]. Polyps can cause intussusception. Microscopically, heterotopic focus shows surface lining by gastric foveolar epithelium with gastric glands (usually fundic type mucosa) [7].
Gastric heterotopias should be differentiated from gastric metaplasias. Gastric metaplasias are acquired lesions. They are usually seen in association with chronic inflammatory conditions like Crohn’s disease. Unlike heterotopias in which grossly identifiable polypoid lesions are present, metaplasias are microscopic lesions composed of foveolar and pyloric glands [8]. Gastric heterotopias are usually congenital. It is believed that rare acquired lesions may be seen in conditions causing hypergastrinemia in which a microscopic lesion undergoes hyperplasia to become a grossly visible lesion [1].
In most of the reported cases of gastric heterotopias in the jejunum patients were below 25 years of age with the youngest patient being one-year-old [7]. Clinical presentation in all the cases were gastrointestinal bleeding [2,3] or obstructive symptoms [1,4,7] caused by polypoid mass [4,5] or stricture [6,7]. In one case report in a 21-year-old female the polypoid mass was 15 cm in size [4] and only one case of jejunal gastric heterotopia with multiple strictures is reported [6]. Our patient was a 24-year-old male with a history of ileocaecal tuberculosis who presented with multiple jejunal strictures and perforation peritonitis. In none of the cases was gastric heterotopia suspected clinically. Diagnosis was made on histotathological examination.
Conclusion
This case is presented for its rarity and to emphasize the fact that the possibility of gastric heterotopia should also be considered in the differential diagnosis of polypoid lesions of the gastrointestinal tract below the ligament of Treitz presenting with bleeding or obstructive symptoms.
[1]. Chinnery GE, Bernon MM, Roberts R, Gastric heterotopias causing jejunal ulceration and obstructionS Afr J Surg 2013 51:146-47. [Google Scholar]
[2]. Jimenez JC, Emil S, Steinmetz B, Rowansky S, Welber M, Recurrent GIT bleeding secondary to jejunal gastric heterotopiasJournal of paediatric surgery 2005 40:1654-57. [Google Scholar]
[3]. Arda MS, Tokar B, Ilhan H, Eren M, Massive gastrointestinal bleeding in children. Diagnosis by enterotomy introduced endoscopyJ Clin Anal Med 2013 4:4-6. [Google Scholar]
[4]. Martinez A, Decanini-Teran O, Soria-Cespedes D, Polypoid and hyperplastic heterotopic gastric mucosa in the jejunum as a cause of recurrent subocclusive episodesAnnals of Gastroenterology 2013 26:1 [Google Scholar]
[5]. Omotosho PA, Varnholt H, Tirabassi MV, Prasad R, Moriarty KP, Giant polypoid gastric heterotopia of jejunum presenting with intermittent intussussceptionJ of Laproendoscop Adv Surg Tech 2007 17:249-51. [Google Scholar]
[6]. Houissa-Vuong S, Martin B, Lascar G, Vuong PN, Multiple jejunal strictures caused by gastric heterotopiaAnn Chir 2001 126:70-74. [Google Scholar]
[7]. Al-Jadaan S, Oda O, A rare clinical presentation of heterotopic gastric mucosa of the jejunum: A case report and review of literatureJ of Ped Surg Case Reports 2014 2:337-40. [Google Scholar]
[8]. Min Y II, Lee BW, Chang YW, Chi HS, Lee JK, The incidence of gastric metaplasia in patients with duodenal ulcerThe Korean Journal of Internal Medicine 1987 2:93-96. [Google Scholar]