Incidents of broken balloon in a coronary vasculature during percutaneous coronary angioplasty are very rare. Such events in cath-lab may create panic and can be life threatening for patients. Hence, immediate retrieval of broken balloon becomes vital. Here, we report an unusual complication of broken balloon in the mid portion of the left anterior descending coronary artery, which had a calcified and totally occluded in-stent restenotic lesion. The broken balloon was retrieved successfully with no eventual complication using a simple catheter-assisted balloon-supported retrieval technique. The present case highlights the need for interventional cardiologist to be acquainted with different retrieval techniques.
Balloon rupture, Calcified lesion, In-stent restenosis, Percutaneous retrieval, Simple balloon retrieval technique
Case Report
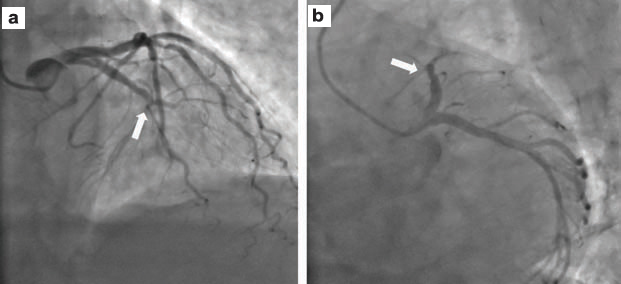
A 60-year-old male presented with unstable angina from past two days. He exhibited angina even on minimal exertion. He had, elsewhere, underwent Percutaneous Coronary Intervention (PCI) with stent implantation to Left Anterior Descending (LAD) coronary artery a year ago. At current presentation, his electrocardiogram revealed T inversion in anterior leads. Diagnostic coronary angiography revealed calcified In-Stent Restenosis (ISR) with a total occlusion (Mehran Type IV) in the mid portion of LAD artery [Table/Fig-1] and 80% tubular lesion in the left circumflex coronary artery [1]. The patient was considered for elective PCI.
Diagnostic coronary angiography revealed calcified in-stent restenosis with a total occlusion (Mehran Type IV) in the mid portion of LAD artery: a) RAO cranial view; b) LAO caudal view.
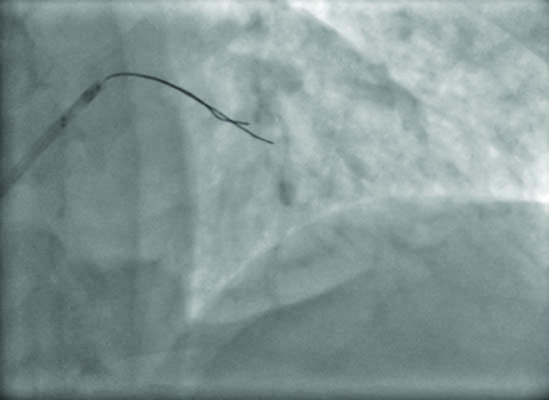
The index procedure was performed through radial approach using an EBU 6F guide catheter (Medtronic Inc., USA). A 0.014” coronary guidewire (Terumo Interventional Systems, USA) was passed through the ISR lesion in LAD vessel. Then, the lesion was predilatated with a 1.25 x 6 mm Sprinter balloon (Medtronic Inc. USA) at 10 atm pressure. Subsequently, the balloon was exchanged with another 2x12 mm semi-compliant Sprinter balloon (Medtronic Inc. USA), and was inflated at 10 atm pressure [Table/Fig-2]. While withdrawing the balloon, it accidentally broke and started floating freely in the mid LAD. Angiographic image revealed that the balloon was broken near the distal end [Table/Fig-3].
The LAD lesion predilatated with a 2 x 12 mm semi-compliant Sprinter balloon at 10 atm pressure.
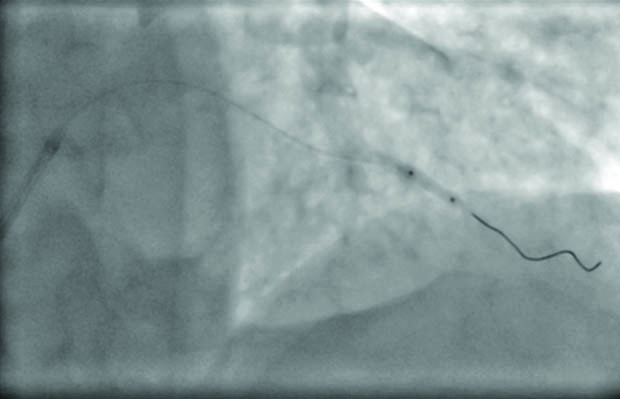
While withdrawing, the balloon accidentally got broke and started floating freely in the mid LAD.
Immediately, several options for retrieving the broken balloon were considered. At first, we thought of attempting to retrieve the ruptured balloon by entangling it between two guidewires or using a small goose neck snare. However, we did not proceed with these retrieval techniques as the chances of success were less and probability of injury to coronary intima were more. Since proximal portion of the coronary artery was free of atherosclerotic plaque, we thought of using balloon-supported catheter-assisted retrieval technique.
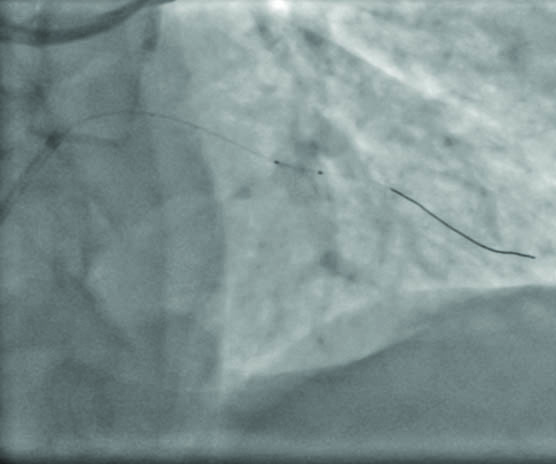
For retrieval of ruptured balloon, a buddy wire (Terumo Interventional Systems, USA) was inserted across the balloon and a 2.5 x 12 mm semi-compliant Sprinter balloon (Medtronic Inc., USA), equal to the angiographic size of mid LAD lesion, was passed on the buddy wire, partially across the broken balloon, and was inflated at 6 atm pressure. Then, the guide catheter was pushed inside the coronary system till it reached broken balloon. Simultaneously, a pulling force was kept upon the inflated balloon, which acted as an anchor. As guide catheter reached broken balloon, the inflated balloon was partially deflated. Due to sudden deflation of the inserted balloon and pulling pressure, the broken balloon was sucked into the guidewire [Video-1]. As both balloons came inside the guide [Table/Fig-4], they were subsequently pulled into the left main coronary artery. Inflation of this supporting balloon inside the guide catheter assisted us in trapping the broken balloon between the outer surface of the inflated balloon and inner surface of the guide catheter. Subsequently, the whole assembly was pulled out enmasse [Table/Fig-5], resulting in successful retrieval of broken balloon [Table/Fig-6] from the mid LAD without much injury to coronary intima. Patient was given unfractionated heparin (7000 units) along with loading doses of dual antiplatelet therapy (ticagrelor and aspirin) for the prevention of thrombus during retrieval. Since LAD lesion appeared significantly calcified and totally occluded, it was decided not to further attempt it.
Attempt to retrieve broken balloon using balloon-supported catheter-assisted retrieval technique.
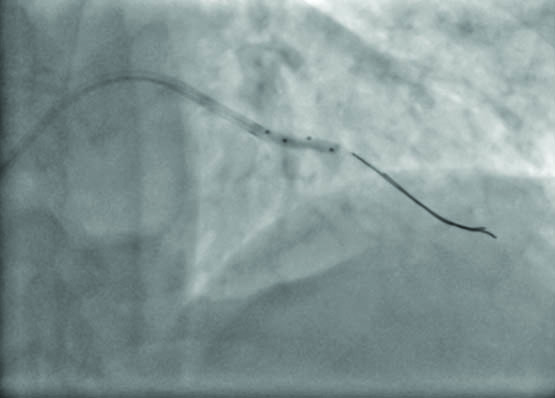
Balloon-supported catheter-assisted trapping of broken balloon lead to its successful retrieval.
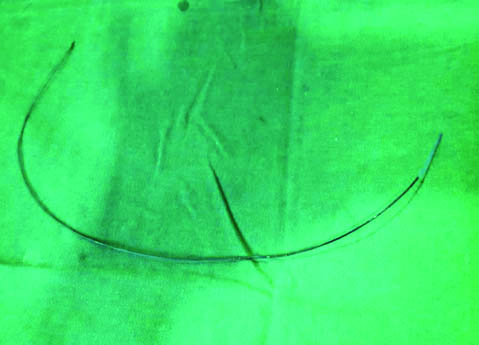
Broken balloon catheter after its retrieval.
Nevertheless, the patient underwent stent implantation for obtuse marginal vessel, which also had a significant lesion. The procedure was successful and the post-procedural stay in hospital was uneventful. The patient was discharged in stable condition after three days with optimized medical therapy. We believe that highly calcified lesion and a significant bend before the lesion in LAD could be the cause for balloon rupture in the present case.
Discussion
PCI is a safe procedure for the management of short and discrete coronary artery stenosis [2]. However, its increasing application in managing complex coronary lesions has led to rise in incidents of fracture, dislodgement, or entrapment of various angioplasty devices. According to an estimate, such incidents of broken or entrapped catheters, guide wires, angioplasty balloons, or stents are noted in 0.1%–0.8% of routine cath lab procedures [3]. Of them, the reports of broken balloon are even rare. At our hospital, we perform more than 1,200 PCI procedures per year and the incidents of device lost, device fracture, or device entrapment was not observed in any of the case so far, making this case as the first such case at our hospital.
Immediate removal of broken cath-lab fragments from the coronary vasculature becomes imperative as they may cause life-threatening consequences like thrombus formation, acute embolization, and myocardial infarction [3]. While cardiothoracic surgery is considered as the last resort, [4] the commonly used percutaneous retrieval techniques include the use of snare devices, paired guidewires, balloon inflation, micro catheter, and biopsy forceps [5]. Despite the availability of such retrieval equipments, percutaneous retrieval may be difficult, unpredictable and, often dangerous. Further, there is no evidence-based optimal approach for the management of such cases, and the choice of retrieval technique is usually individualized in most cases based on patient’s condition, operator experience, and availability of retrieval devices. Hence, it is vital for an interventional cardiologist to be acquainted with different retrieval techniques as the breakage of angioplasty devices in the coronary vasculature can often cause panic in the cath lab and can test the nerves of even the most experienced interventional cardiologist [2].
Earlier, Mehta V et al., reported a successful retrieval of impacted broken balloon by balloon inflation in guiding catheter [6]. Conversely, Girish MP et al., also reported a successful retrieval of a partially inflated balloon with a broken shaft from the coronary system using a simple technique using a Fogarty balloon, which did not involve the use of a snare or any other retrieval tool [3]. Chang WT et al., also described two similar cases of successful percutaneous retrieval of ruptured coronary balloon during emergency or elective PCI [7]. In similar lines, we present a challenging case of accidentally broken semi-compliant balloon in a calcified ISR lesion in LAD vessel. We did not opt for snare devices or paired-guide wire techniques for retrieval due to the concerns over thrombotic risks associated with them. On the contrary, we opted for the balloon-supported retrieval technique demonstrating that this technique was quite easy, less cumbersome, less time-consuming and safe way to remove the entrapped fragments of cath-lab devices from the coronary system. In addition, we monitored the activated clotting time during device retrieval to prevent thrombus formation around the broken balloon.
Usually, the events of broken balloon during PCI occurs due to patient-related factors (i.e., calcified or tortuous vessel, complex lesion), operator-related factors (i.e., inadequate predilatation, excessive pushing, frequent re-use of hardware), or device-related factors (i.e., manufacturing defects) [8]. We believe that highly calcified ISR lesion and a significant bend before the LAD lesion could be the contributing cause for balloon rupture in the present case. Remarkably, the balloon was broken during pre-dilatation.
Conclusion
The indexed case highlights the importance of adequate lesion assessment and preparation during the index procedure. We demonstrated that broken balloon can be retrieved successfully using a simple trapping technique with another noncompliant balloon, without the need for additional devices such as a snare. Availability and knowledge of such retrieval systems can be life saving for the patient.
[1]. Mehran R, Dangas G, Abizaid AS, Mintz GS, Lansky AJ, Satler LF, Angiographic patterns of in-stent restenosis: classification and implications for long-term outcomeCirculation 1999 100:1872-78. [Google Scholar]
[2]. Singh J, Thingnam SK, Das D, Singh H, Sharma R, Vijayvergia R, Surgical removal of entrapped and broken percutaneous transluminal coronary angioplasty balloon catheterInteract Cardiovasc Thorac Surg 2007 6:94-96. [Google Scholar]
[3]. Girish MP, Gupta MD, Mittal A, Percutaneous retrieval of entrapped partially inflated broken coronary angioplasty balloon by modified Fogarty techniqueJ Invasive Cardiol 2011 23:E173-76. [Google Scholar]
[4]. Patil S, Ramalingam R, Kharge J, Nayak M, Manjunath CN, Successful retrieval of uncoiled coronary guidewire using simple balloon methodJ Clin Diagn Res 2015 9:OD01-03. [Google Scholar]
[5]. Ancona MB, Giannini F, Jabbour RJ, Tanaka A, Regazzoli D, Mangieri A, Left main "Culotte in Culotte" to manage a trapped broken balloonInt J Cardiol 2016 221:347-49. [Google Scholar]
[6]. Mehta V, Pandit BN, Yusuf J, Mukhopadhyay S, Trehan V, Tyagi S, Retrieval of impacted broken balloon by balloon inflation in guiding catheterCardiovasc Interv Ther 2014 29:252-55. [Google Scholar]
[7]. Chang WT, Chen JY, Li YH, Tsai LM, Lee CH, A two-case series of entrapment of a ruptured balloon in the coronary artery: Avoidable complications and nonsurgical managementJ Formos Med Assoc 2015 114:1135-39. [Google Scholar]
[8]. Kharge J, Sreekumar P, Swamy K, Bharatha A, Ramegowda RT, Nanjappa MC, Balloon-assisted retrieval of a broken stent-delivery systemTex Heart Inst J 2012 39:644-46. [Google Scholar]