Introduction
Oral Mucositis (OM), a complication of cancer treatment, is a debilitating disorder and is defined as an injury of the oral mucosa in patients with cancer, induced by chemotherapy or radiation to the head and neck region [1].
A very complicated biologic process is responsible for OM. Mechanisms such as direct injury to the oral epithelium during cell proliferation, dysregulation of the immune system, exaggerated inflammatory responses, changes in inflammatory cytokines {e.g., Tumour Necrosis Factor-α (TNF-α), Interleukin-1 (IL-1), and interleukin 6 (IL-6)}, and super infections by oral bacterial flora are involved in OM [2,3].
In some cases, OM has a dose limiting toxicity, delaying or preventing continuing of chemotherapy that may potentially have an important effect on survival or cure. Chemotherapy induced OM is typically less severe and is of shorter duration (3–12 days) than that associated with Radiotherapy (RT) (3–12 weeks) and usually affects non-keratinized mucosa, in the first and second weeks of chemotherapy treatment, and subsides during the third or fourth week following chemotherapy [2,4].
Sodium carbonate, local anaesthetics such as diphenhydramine and promethazine mixed with manganese milk, chlorhexidine and saline mouthwashes have been used to control OM in addition to covering agents such as sucralfate, and an anti-inflammatory agents (e.g., chamomile) or local steroids [5–11]. A systematic review revealed that a low level laser has beneficial effects over a range of wavelengths and intensities in managing OM in patients with cancer [12]. Other systematic reviews have shown useful effects by using cryotherapy, cytokines, growth factors, honey, aloevera, amifostin, glutamine, and antibiotic pastille in different types of cancer and treatment settings [13–17].
Quercetin belongs to the flavonoid family and is the most available type of flavonoids for daily diet and has the most antioxidant and anti-inflammatory activity among available flavonoids. The anti-inflammatory properties have been related to restriction of cytokines including IL-12, INF-γ, INF-α, IL-8, cyclo-oxygenase 2, and prostaglandin E. Furthermore, quercetin produces an antioxidant effect by inhibiting free radicals and nitric oxide [18–22]. Topical quercetin has been used to treat oral aphthous stomatitis, and complete improvement of lesions has been reported [23]. In vitro and animal studies and trials on healthy volunteers have suggested use of quercetin in various situations such as drug resistant diseases related to oxidative stress, blood pressure, inhibition of cancer cell cycle progression, and cardio-metabolic risk [24–28]. A critical review supported the safety of quercetin for addition to food as a supplement [29]. In a study conducted by the authors, systemic administration of quercetin in oral lichen planus had no considerable clinical benefit [30].
Due to the anti-inflammatory and antioxidant properties of quercetin, it may prevent or treat OM. This study assessed the efficacy of quercetin in preventing and treating chemotherapy induced oral mucositis in haematologic malignancies.
Materials and Methods
Patients
The study was conducted in the Department of Heamatology Imam Reza Hospital, Mashhad, Iran, from January 2010 to January 2012. Twenty-three patients who underwent chemotherapy for blood malignancies (for the first time) participated in this double blind, placebo controlled randomized trial.
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences (Iran), and all subjects gave written informed consent to participate in the study. This study was registered in the U.S. National Institute of Health Registry of Clinical Trials (registry number NCT01732393). The inclusion criteria were: (a) 15 years of age or older; (b) patient undergoing chemotherapy for a haematologic malignancy; (c) the haematologist approved the patient’s participation; and (d) agreement of patient to participate in the trial. Exclusion criteria were: (a) presence of any oral lesion at the beginning of the trial; (b) loss of follow up; (c) use of digoxin and cyclosporine; and (d) patient death. There were no patients with history of previous head and neck surgery, pregnancy, and previous or simultaneous radiotherapy. No patients had dentures.
Sample Size
This study was the first research on OM and quercetin, so we enrolled 23 patients in this pilot study.
Intervention, Randomization, and Blinding
The patients were randomly allocated into two groups (quercetin and placebo) according to a series of random numbers created by a calculator. Eleven patients were in the intervention group, and 12 patients in the control group. All patients were followed until the end of chemotherapy treatment and were informed about oral hygiene, including drinking water and brushing teeth with a soft tooth brush presoaked in warm water, after each meal, as well as abstinence from alcohol, smoking cigarettes, hot or cold drinks, and very spicy, acidic, and tough foods during chemotherapy. If a patient had severe thrombocytopenia (<50,000/mm3) during chemotherapy that might challenge efficient brushing, other less aggressive oral health measures was taught to the patient.
The two study groups were provided identical capsules (series A and B). The intervention group received A capsules containing 250 mg quercetin hydrate (Sigma–Aldrich Co; St Louis, MO, USA) two times a day, and the control group received B capsules (placebo) containing a lactose capsule. Drug therapy was initiated at the onset of chemotherapy. In both the groups patients received the drugs for a period of four weeks. The patients, researcher, and statistician were blind to the content of the capsules, and only the pharmacologist (HO) was aware.
Evaluation of Outcomes
Patients’ oral health was checked by an oral medicine specialist before chemotherapy was initiated. A dentist and an oral medicine specialist who were blinded to the randomization and treatment monitored patients for the appearance of OM daily until the end of chemotherapy. Patients were examined with an overhead light, by using dental tools and mirrors. Sterile gauze was used to wipe out debris when necessary. The World Health Organization (WHO) oral toxicity scale was used to evaluate OM. [Table/Fig-1] summarizes the WHO scale for assessing OM [31].
WHO scale for assessing oral mucositis [31].
| Grade | 0 | 1 | 2 | 3 | 4 |
|---|
| Clinical status | No oral mucositis | Erythema and soreness | Ulcers, able to eat solid foods | Ulcers, requires liquid diet (due to mucositis) | Ulcers, chewing not possible (due to mucositis) |
The primary outcome of the study was preventing incidence and onset of OM. The secondary outcome was the severity of OM based on WHO scale.
Although rare, any adverse effect in the patients was recorded and kept under observation. If the adverse event was too serious, the trial was stopped, and the patient was closely monitored.
Statistical Analysis
Statistical analysis was performed with SPSS 11.0 (SPSS 11.0 windows, SPSS Inc, Chicago, IL, USA). The Mann-Whitney U test evaluated mucositis intensity. The Friedman test evaluated the effect of time. A p-value was considered significant at the 0.05 level for the Mann-Whitney U test. To prevent a repeated measurement error, we divided α into 10 and 0.05 for the Friedman and Mann-Whitney U test.
Results
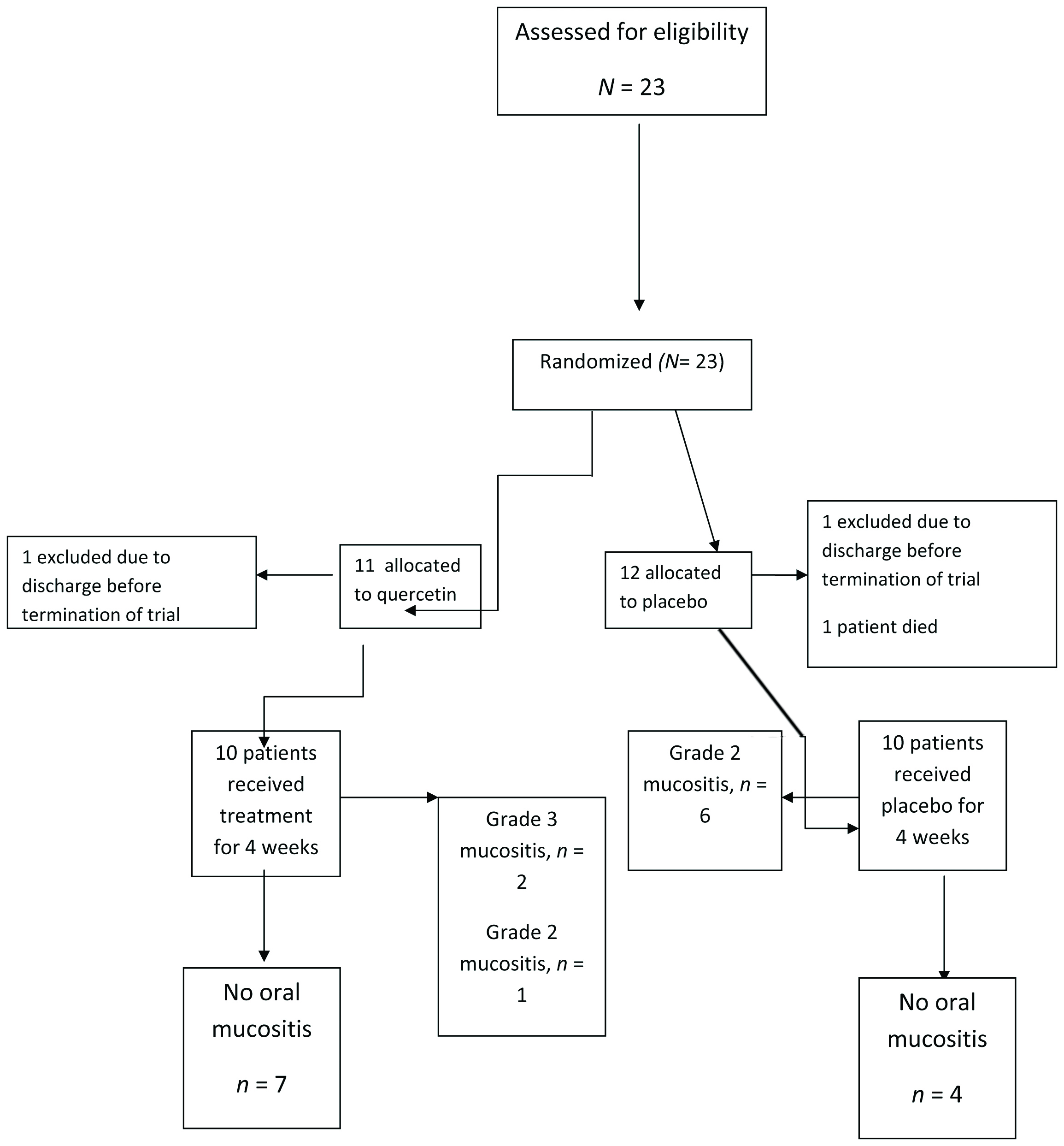
Twenty-three patients were included in this trial. One patient died (in the control group) and 2 patients were discharged (1 in each group) before the trial ended; thus, 20 patients completed the trial. In each group, four women and six men received either quercetin or placebo [Table/Fig-2].
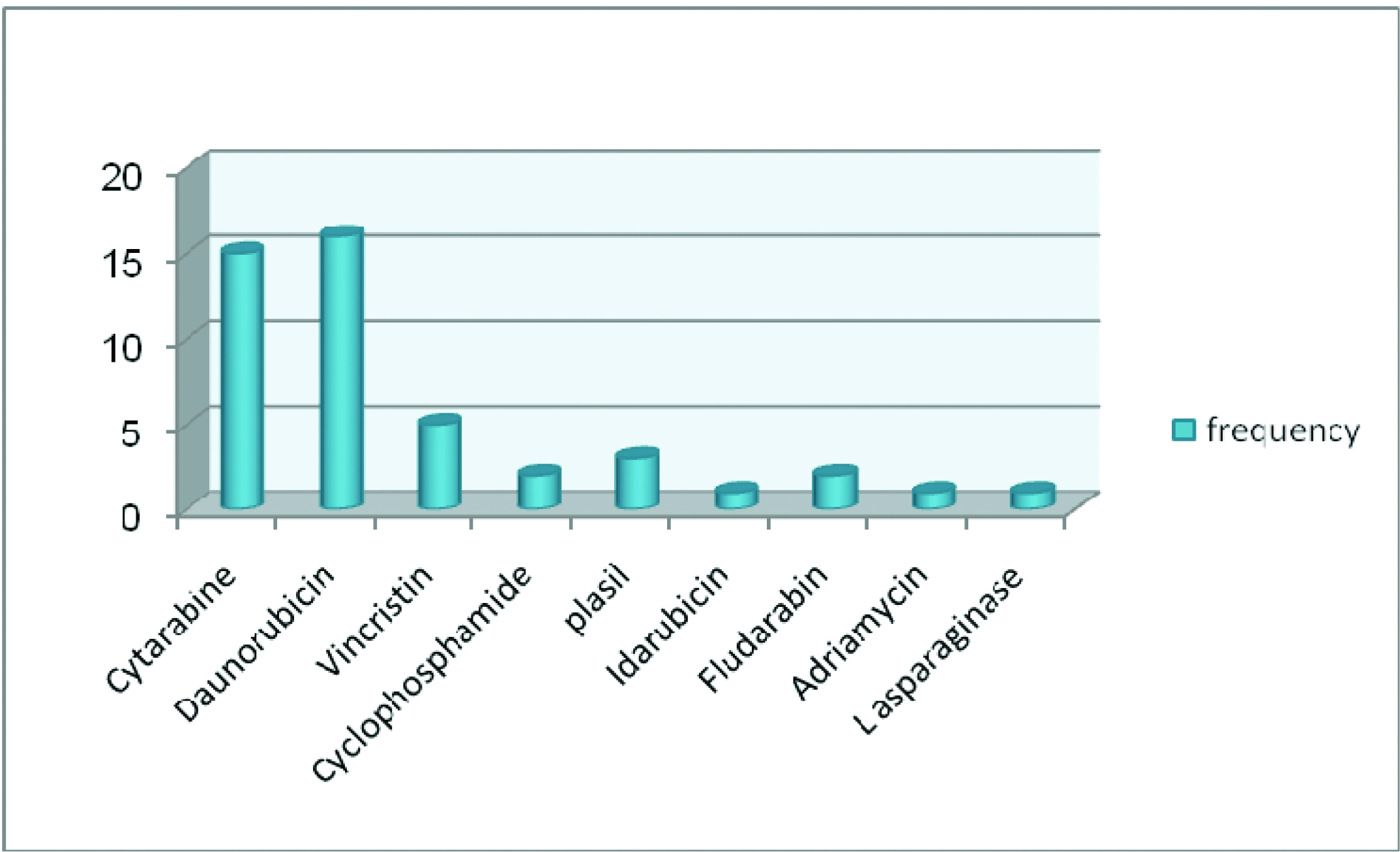
The mean age of patients was 33±15.9 (cases: 33±17, controls: 33±16), and the patients ranged from 15 to 5-year-old. There was no significant difference between the two groups (p =0.946) [Table/Fig-3]. Patients received different chemotherapy regimens [Table/Fig-4]. Cytarabin and daunorubicin was the most common regimen. The type of chemotherapy regimen was not related to incidence of mucositis in the study population (p =0.685).
| Variables | Age range | Mean age | Blood dyscrasiaAML*,ALL** | Incidence ofmucositis | Mean severityof mucositis intotal studypopulation | Mean disease-free time | Mean onset ofmucositis (dayafter initiation ofchemotherapy)in involvedpatients(n=9) | Mean durationof healing ofmucositis(days) |
|---|
| Case | 19–68 | 33±17 | 8,2 | 3 | 0.8±1.30 | 17.30±6 | 9.67 | 14±4.16 |
| Control | 15–65 | 33±16 | 7,3 | 6 | 1.3±1.16 | 13.4±6.57 | 9.33 | 10±2.26 |
| P-value | 0.946 | 0.946 | 0.615 | 0.189 | 0.379 | 0.218 | 0.756 | 0.167 |
| Total | 15–68 | 33±15.9 | 15,5 | 9 | 1.05±1.23 | 15.35±6.44 | 9.44±1.00 | 11.78±3.34 |
Chemotherapy regimens in the study population.
Three patients in the intervention group were affected by OM. Two patients had Grade 3 OM, and one had Grade 2 OM. The mean severity of OM was 0.8±1.30 in the intervention group. In the control group, six patients were involved, and all had Grade 2 OM. The mean severity of OM was 1.30±1.16 in the control group. No patients had Grade 4 OM. [Table/Fig-5] shows the mean severity of mucositis in the two groups and the total study population. Incidence of mucositis was lower in the intervention group (30% vs 60%).
Mean severity of oral mucositis (vertical axis) in the intervention group (red line), the control group (blue line), and the total study population (green line) due to days after initiation of chemotherapy (horizontal axis).
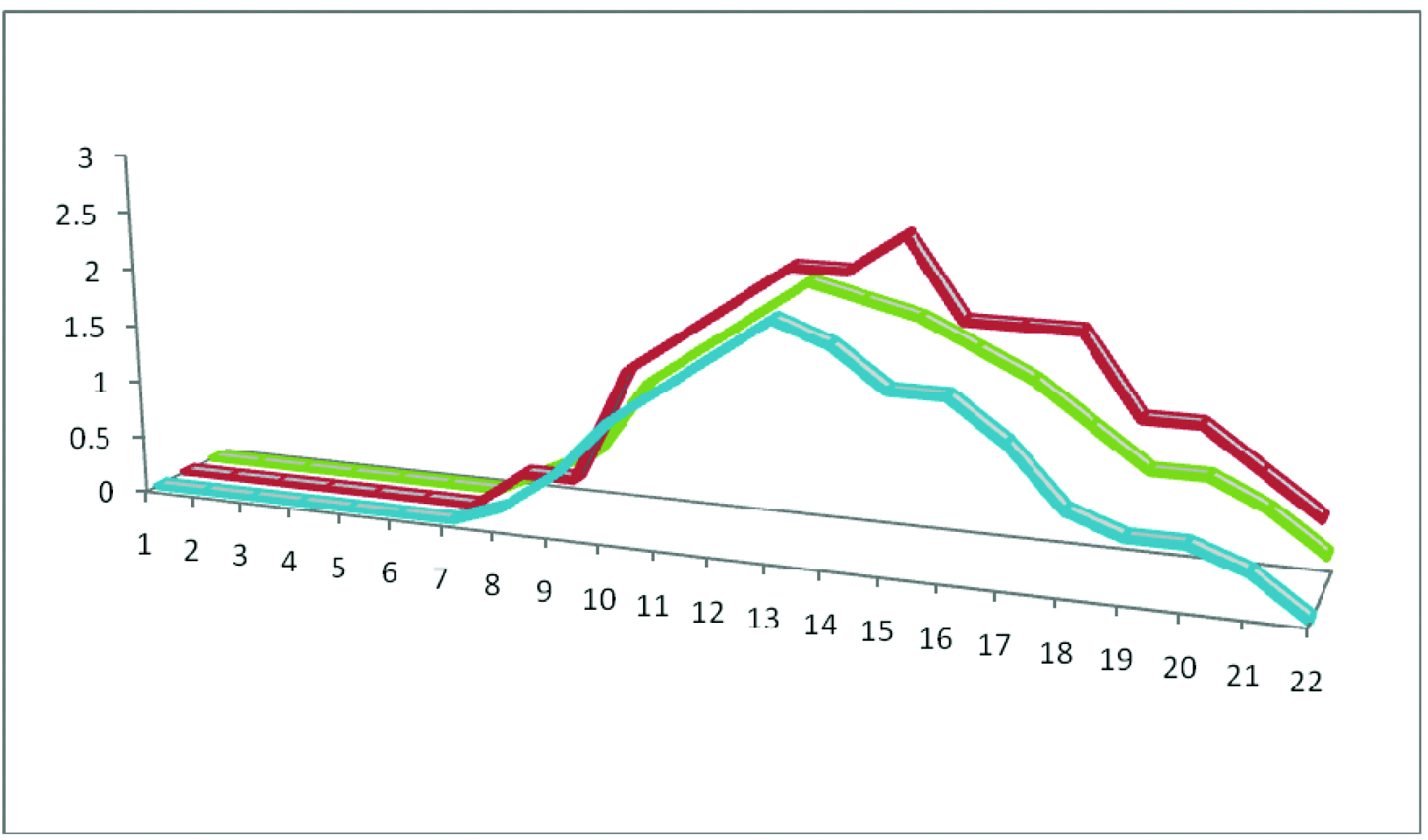
Although, fewer patients had mucositis in the intervention group, the mucositis was more severe in this group (2.6) compared to the control group (2) but was not statistically different (p =.12). [Table/Fig-3] shows detailed findings of the study. An interesting finding in these three patients was the poor oral health level due to the severity of the systemic disease. Onset of mucositis was different from 8 to 11 days after chemotherapy was initiated. The mean onset was similar in the two groups [Table/Fig-3].
The healing duration was longer in the intervention group but was not statistically significant (p =0.167). [Table/Fig-3] shows a detailed description of the patients’ data. Analysis showed a reduced risk of OM with 50% (CI=0.02–50.397) Relative Risk (RR) in the intervention group compared to the control group.
Discussion
OM is a common and debilitating complication of cancer treatment with many clinical and economic outcomes; thus, many studies have been conducted. Perhaps the most aversive outcome of OM is the inability to intake food orally. Although many local and systemic modalities have been suggested for preventing and treating OM, little evidence is available to support a specific and effective treatment. Each treatment may lead to complications that must be considered. Some guidelines and oral care protocols has been suggested for managing oral mucositis that are not globally accepted [31–36].
In this randomized clinical trial, quercetin, an herbal flavonoid, was used to prevent and treat chemotherapy induced oral mucositis. This flavonoid is safe, absorbs adequately, and is not expensive. Many studies have shown anti-inflammatory properties of quercetin. Sotnikova R planned an in vivo study to reveal efficacy of two derivatives of quercetin (chloronaphthoquinone quercetin and monochloropivaloyl quercetin) in prevention of ulcerative colitis in rats. He concluded that chloronaphthoquinone quercetin can depress inflammatory damage to the colon although the exact mechanism remains unclear [36]. Effect of quercetin on oxaliplatin induced peripheral neuropathy was assessed by Azevedo MI et al., an animal study on mice showed that quercetin can inhibit thermal and mechanical nociceptive response in dorsal horn via decreased inducible nitric oxide synthase [37]. Another study on nano quercetin showed that downregulating MMP-9 and NOS-2 by this drug can prevent ethanol induced gastric inflammation in rats [38]. Several studies have shown that quercetin can protect gastric mucosa from ulceration [39–44]. This protective effect works due to antioxidative mechanisms such as inhibition of lipid peroxidation, decrease of reactive oxygen metabolites, inhibition of neutrophil infiltration, increase of superoxide dismutase activity, increased gastric mucus secretion, inhibition of free radical production by activated neutrophils via ICAM-1, and pro-inflammatory cytokine down regulation [40–44]. Evidence about anti-inflammatory effect of quercetin on oral ulcers is lacking. In a study by Hamdy AA showed that topical quercetin can improve recurrent aphthous stomatitis [23]. Effect of quercetin on prevention and treatment of chemotherapy induced OM was assessed in our study. Twenty-three patients were enrolled in this study. Three patients were excluded; thus, 20 patients finished the trial. Eight men and 12 women with a mean age of 33-year-old were randomly assigned to two study groups. The chemotherapy regimens were similar in both groups; therefore, OM was not related to the chemotherapy drugs. The incidence of mucositis was lower in the intervention group (3 of 10 vs 6 of 10). This difference was not statistically significant (p=0.189), but perhaps quercetin has some protective effect on OM.
Qutob AF et al., performed a systematic review to assess a preventive model for oral mucositis in children [45]. There was not enough evidence to support any modality (chlorhexidin mouthwash, laser therapy, glutamine, etc.,) for preventing OM. They concluded that oral sucralfate suspension, prostaglandin E2 tablets, and Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF) mouthwashes should not be considered in preventing OM due to the strength of evidence against their use. The authors showed that evidence is in favour of oral care protocols; thus, the only confirmed preventive means is oral health care. Another systematic review showed that oral cryotherapy can prevent OM in patients receiving bolus fluorouracil (5-FU) or high-dose melphalan [13]. In our study, the three patients in the intervention group with OM had more severe OM than those affected in the control group. They had a poor oral health status due to the severity of systemic disease. We did not compare oral health status in the groups because criteria of oral health were not used.
We used 250 mg quercetin BID. The maximum daily use for quercetin is 1500 mg, but due to special medical situation of the patient and the risk of unknown adverse drug effects and interactions, we used the minimal effective dose.
In our study, 20% of the intervention group had Grade 3 OM, but none of the control group had Grade 3 and 4 OM. Interventions to reduce OM severity have shown that paliformin, triclosan, zinc sulfate, and chlorhexidin can be effective, but further research is necessary to obtain enough evidence. A systematic review showed that low-level laser therapy can be helpful in preventing OM in patients undergoing radiotherapy without concomitant chemotherapy for head and neck cancer, but was not feasible for other treatment settings. Palifermin and GM-CSF may be useful in preventing OM in patients receiving allograft stem cell transplantation. In a Cochrane systematic review, 10 interventions including aloevera, amifostine, cryotherapy, granulocyte-colony stimulating factor (G-CSF), intravenous glutamine, honey, keratinocyte growth factor, laser, Polymixin/Tobramycin/Amphotericin (PTA) antibiotic pastille/paste, and sucralfate had some benefit (albeit sometimes weak) for preventing or treating OM, although the researcher observed that the benefit may be specific for treatment of certain types of cancer and subgroup analysis must be performed in larger study populations [17].
Rodriguez-Caballero A et al., performed a critical review and concluded that it is necessary to combine interventions that act on the different phases of OM. We showed that quercetin can reduce the total relative risk of OM (30% vs 60%), but the risk of Grade 3 and 4 OM was high in the intervention group (20% vs 0%) [46].
Quercetin has a biphasic anti-inflammatory effect. At a lower dose, lymphocytes are irritated, but at higher doses, quercetin has an inhibitory effect on lymphocytes. Using higher doses might prevent or treat OM effectively; however, further study is needed to reveal the effect of administering quercetin in preventing and treating OM [20].
Quercetin is an herbal medication with little adverse reaction. If future research confirms using this drug in treating OM, it would be of great help. This study has several limitations, such as small sample size and the patients’ poor oral health state. We suggest future studies use a larger sample and higher quercetin dose and control oral health status by using the oral health index in study groups.
Conclusion
Quercetin could prevent OM in intervention group but further research with larger sample size and more controlled clinical setting is recommended.
Conflict of interest disclosure
The authors declare no competing financial interests with any product mentioned in this manuscript.
[1]. Motallebnejad M, Akram S, Moghadamnia A, Moulana Z, Omidi S, The effect of topical application of pure honey on radiation-induced mucositis: A randomized clinical trialJ Contemp Dent Pract 2008 9(3):40-47. [Google Scholar]
[2]. Arbabi-Kalati F, Arbabi-Kalati F, Deghatipour M, Ansari Moghaddam A, Evaluation of the efficacy of zinc sulfate in the prevention of chemotherapy-induced mucositis: A double-blind randomized clinical trialArch Iran Med 2012 15(7):413-17. [Google Scholar]
[3]. Watanabe T, Ishihara M, Matsuura K, Mizuta K, Itoh Y, Polaprezinc prevents oral mucositis associated with radiochemotherapy in patients with head and neck cancerInt J Cancer 2010 127(8):1984-90. [Google Scholar]
[4]. Rosenthal DI, Trotti A, Strategies for managing radiation-induced mucositis in head and neck cancerSemin Radiat Oncol 2009 19(1):29-34. [Google Scholar]
[5]. Dodd MJ, Larson PJ, Dibble SL, Miaskowski C, Greenspan D, MacPhail L, Randomized clinical trial of chlorhexidine versus placebo for prevention of oral mucositis in patients receiving chemotherapyOncol Nurs Forum 1996 23(6):921-27. [Google Scholar]
[6]. Carl W, Emrich LS, Management of oral mucositis during local radiation and systemic chemotherapy: A study of 98 patientsJ Prosthet Dent 1991 66(3):361-69. [Google Scholar]
[7]. Barker G, Loftus L, Cuddy P, Barker B, The effects of sucralfate suspension and diphenhydramine syrup plus kaolin-pectin on radiotherapy-induced mucositisOral Surg Oral Med Oral Path 1991 71(3):288-93. [Google Scholar]
[8]. Meredith R, Salter M, Kim R, Spencer S, Wepplemann B, Rodu B, Sucralfate for radiation mucositis: Results of a double-blind randomized trialInt J Radiat Oncol Biol Physics 1997 37(2):275-79. [Google Scholar]
[9]. Martins MD, Marques MM, Bussadori SK, Martins MAT, Pavesi VCS, Mesquita-Ferrari RA, Comparative analysis between Chamomillarecutita and corticosteroids on wound healing. An in vitro and in vivo studyPhytother Res 2009 23(2):274-78. [Google Scholar]
[10]. Turhal N, Erdal S, Karacay S, Efficacy of treatment to relieve mucositis-induced discomfortSupport Care Cancer 2000 8(1):55-58. [Google Scholar]
[11]. Nyman J, Turesson I, Does the interval between fractions matter in the range of 4–8 h in radiotherapy? A study of acute and late human skin reactionsRadiother Oncol 1995 34(3):171-78. [Google Scholar]
[12]. Migliorati C, Hewson I, Lalla RV, Antunes HS, Estilo CL, Hodgson B, Systematic review of laser and other light therapy for the management of oral mucositis in cancer patientsSupport Care Cancer 2013 21(1):333-41. [Google Scholar]
[13]. Peterson DE, Ohrn K, Bowen J, Fliedner M, Lees J, Loprinzi C, Systematic review of oral cryotherapy for management of oral mucositis caused by cancer therapySupport Care Cancer 2013 21(1):327-32. [Google Scholar]
[14]. Raber-Durlacher JE, von Bultzingslowen I, Logan RM, Bowen J, Al-Azri AR, Everaus H, Systematic review of cytokines and growth factors for the management of oral mucositis in cancer patientsSupport Care Cancer 2013 21(1):343-55. [Google Scholar]
[15]. Song JJ, Twumasi-Ankrah P, Salcido R, Systematic review and meta-analysis on the use of honey to protect from the effects of radiation-induced oral mucositisAdv Skin Wound Care 2012 25(1):23-28. [Google Scholar]
[16]. Worthington HV, Clarkson JE, Bryan G, Furness S, Glenny AM, Littlewood A, Interventions for preventing oral mucositis for patients with cancer receiving treatmentCochrane Database Syst Rev 2010 (12):CD000978 [Google Scholar]
[17]. Worthington HV, Clarkson JE, Bryan G, Furness S, Glenny AM, Littlewood A, Interventions for preventing oral mucositis for patients with cancer receiving treatmentCochrane Database Syst Rev 2011 (4):CD000978 [Google Scholar]
[18]. Ying B, Yang T, Song X, Hu X, Fan H, Lu X, Quercetin inhibits IL-1 beta-induced ICAM-1 expression in pulmonary epithelial cell line A549 through the MAPK pathwaysMol Biol Rep 2009 36(7):1825-32. [Google Scholar]
[19]. Yu ES, Min HJ, An SY, Won HY, Hong JH, Hwang ES, Regulatory mechanisms of IL-2 and IFNγ suppression by quercetin in T helper cellsBiochem Pharmacol 2008 76(1):70-78. [Google Scholar]
[20]. Zakizadeh M, Nabavi S, Nabavi S, Ebrahimzadeh M, In vitro antioxidant activity of flower, seed and leaves of Alcea hyrcana GrosshEur Rev Med Pharmacol Sci 2011 15(4):406 [Google Scholar]
[21]. Yousef MI, Omar SA, El-Guendi MI, Abdelmegid LA, Potential protective effects of quercetin and curcumin on paracetamol-induced histological changes, oxidative stress, impaired liver and kidney functions and haematotoxicity in ratFood ChemToxicol 2010 48(11):3246-61. [Google Scholar]
[22]. Kao TK, Ou YC, Raung SL, Lai CY, Liao SL, Chen CJ, Inhibition of nitric oxide production by quercetin in endotoxin/cytokine-stimulated microgliaLife Sci 2010 86(9):315-21. [Google Scholar]
[23]. Hamdy AA, Ibrahem MA, Management of aphthous ulceration with topical quercetin: A randomized clinical trialJ Contemp Dent Pract 2010 11(4):E009-16. [Google Scholar]
[24]. Chen C, Zhou J, Ji C, Quercetin: A potential drug to reverse multidrug resistanceLife Sci 2010 87(11):333-38. [Google Scholar]
[25]. Boots AW, Wilms LC, Swennen EL, Kleinjans J, Bast A, Haenen GR, In vitro and ex vivo anti-inflammatory activity of quercetin in healthy volunteersNutrition 2008 24(7):703-10. [Google Scholar]
[26]. Boots AW, Haenen GR, Bast A, Health effects of quercetin: from antioxidant to nutraceuticalEur J Pharmacol 2008 585(2):325-37. [Google Scholar]
[27]. Jeong JH, An JY, Kwon YT, Rhee JG, Lee YJ, Effects of low dose quercetin: Cancer cell-specific inhibition of cell cycle progressionJ Cell Biochem 2009 106(1):73-82. [Google Scholar]
[28]. Lee KH, Park E, Lee HJ, Kim MO, Cha YJ, Kim JM, Effects of daily quercetin-rich supplementation on cardiometabolic risks in male smokersNutr Res Pract 2011 5(1):28-33. [Google Scholar]
[29]. Harwood M, Danielewska-Nikiel B, Borzelleca J, Flamm G, Williams G, Lines T, A critical review of the data related to the safety of quercetin and lack of evidence of in vivo toxicity, including lack of genotoxic/carcinogenic propertiesFood Chem Toxicol 2007 45(11):2179-205. [Google Scholar]
[30]. Amirchaghmaghi M, Delavarian Z, Iranshahi M, Shakeri MT, Mosannen Mozafari P, Mohammadpour AH, A randomized placebo-controlled double blind clinical trial of quercetin in oral lichen planusJ Dent Res Dent Clin Dent Prospects 2015 9(1):23-28. [Google Scholar]
[31]. Peterson D, Bensadoun RJ, Roila F, Management of oral and gastrointestinal mucositis: ESMO clinical practice guidelinesAnn Oncol 2011 22(suppl 6):vi78-vi84. [Google Scholar]
[32]. Cheng K, Molassiotis A, Chang A, Wai W, Cheung S, Evaluation of an oral care protocol intervention in the prevention of chemotherapy-induced oral mucositis in paediatric cancer patientsEur J Cancer 2001 37(16):2056-63. [Google Scholar]
[33]. Levy-Polack MP, Sebelli P, Polack NL, Incidence of oral complications and application of a preventive protocol in children with acute leukemiaSpec Care Dentist 1998 18(5):189-93. [Google Scholar]
[34]. Cheng KK, Chang AM, Yuen M, Prevention of oral mucositis in paediatric patients treated with chemotherapy: A randomised crossover trial comparing two protocols of oral careEur J Cancer 2004 40(8):1208-16. [Google Scholar]
[35]. Chen CF, Wang RH, Cheng SN, Chang YC, Assessment of chemotherapy-induced oral complications in children with cancerJ Pediatr Oncol Nurs 2004 21(1):33-39. [Google Scholar]
[36]. Sotnikova R, Nosalova V, Navarova J, Efficacy of quercetin derivatives in prevention of ulcerative colitis in ratsInterdiscip Toxicol 2013 6(1):9-12. [Google Scholar]
[37]. Azevedo MI, Pereira AF, Nogueira RB, Rolim FE, Brito GA, Wong DV, The antioxidant effects of the flavonoids rutin and quercetin inhibit oxaliplatin-induced chronic painful peripheral neuropathyMol Pain 2013 9(1):53 [Google Scholar]
[38]. Chakraborty S, Stalin S, Das N, Thakur Choudhury S, Ghosh S, Swarnakar S, The use of nano-quercetin to arrest mitochondrial damage and MMP-9 upregulation during prevention of gastric inflammation induced by ethanol in ratBiomaterials 2012 33(10):2991-3001. [Google Scholar]
[39]. Martin M, La-Casa C, Alarcon-de-La-Lastra C, Cabeza J, Villegas I, Motilva V, Anti-oxidant mechanisms involved in gastroprotective effects of quercetinZeitschrift für Naturforschung C 1998 53(1-2):82 [Google Scholar]
[40]. Suzuki Y, Ishihara M, Segami T, Ito M, Anti-ulcer effects of antioxidants, Quercetin,. ALPHA.-Tocopherol, Nifedipine and Tetracycline in ratsJpn J Pharmacol 1998 78(4):435-41. [Google Scholar]
[41]. Zahorodny M, Effect of quercetin on sodium diclofenac-induced ulcerationLik Sprava 2003 (1):96-99. [Google Scholar]
[42]. Min YS, Lee SE, Hong ST, Kim HS, Choi BC, Sim SS, The inhibitory effect of quercetin-3-O-β-D-glucuronopyranoside on gastritis and reflux esophagitis in ratsKorean J Physiol Pharmacol 2009 13(4):295-300. [Google Scholar]
[43]. Sumbul S, Ahmad MA, Mohd A, Mohd A, Role of phenolic compounds in peptic ulcer: An overviewJ Pharm Bioallied Sci 2011 3(3):361 [Google Scholar]
[44]. Yan XM, Joo MJ, Lim JC, Whang WK, Sim SS, Im C, The effect of quercetin-3-O-β-D-glucuronopyranoside on indomethacin-induced gastric damage in rats via induction of mucus secretion and down-regulation of ICAM-1 expressionArchives of Pharmacal Research 2011 34(9):1527-34. [Google Scholar]
[45]. Qutob AF, Gue S, Revesz T, Logan RM, Keefe D, Prevention of oral mucositis in children receiving cancer therapy: A systematic review and evidence-based analysisOral Oncol 2013 49(2):102-07. [Google Scholar]
[46]. Rodriguez-Caballero A, Torres-Lagares D, Robles-Garcia M, Pachon-Ibanez J, Gonzalez-Padilla D, Gutierrez-Perez JL, Cancer treatment-induced oral mucositis: A critical reviewInt J Oral Maxillofac Surg 2012 41(2):225-38. [Google Scholar]