Delayed Presentation of Isolated Jejunal Perforation Following Accidental Trauma
Kshitij Arun Manerikar1, Priyank Verma2, Abhijit Ghatage3, Shishir Garg4, Mirat Dholakia5
1 Resident, Department of Surgery, Dr. D.Y. Patil Medical College and Hospital Research Centre, Pune, Maharashtra, India.
2 Resident, Department of Paediatrics, Dr. D.Y. Patil Medical College and Hospital Research Centre, Pune, Maharashtra, India.
3 Resident, Department of Paediatrics, Dr. D.Y. Patil Medical College and Hospital Research Centre, Pune, Maharashtra, India.
4 Resident, Department of Paediatrics, Dr. D.Y. Patil Medical College and Hospital Research Centre, Pune, Maharashtra, India.
5 Resident, Department of Surgery, Dr. D.Y. Patil Medical College and Hospital Research Centre, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kshitij Arun Manerikar, Resident, Department of Surgery, Dr D Y Patil Medical College Hospital and Research Centre, Sant Tukaram Nagar, Pimpri-411018, Pune, Maharashtra, India.
E-mail: drkshitijmanerikar@gmail.com
Blunt abdominal trauma can injure any abdominal organs which had significant morbidity and mortality in paediatric age group. It can lead to duodenal, jejunal or rather any bowel perforation. Isolated jejunal perforation still remains rare entity with less documented reports in specifically paediatric age group. We hereby present a case of three-year-old female child with isolated jejunal perforation, post history of fall from height. Early exploration and prompt surgical intervention led to successful outcome in this patient.
Abdominal trauma, Jejuno-jejunostomy, Paediatric patient
Case Report
A three-year-old female child was admitted to emergency department with a history of accidental fall from six-feet height to ground one day before. According to the parents, the child was asymptomatic initially. She started complaining of pain all over abdomen after four hours of fall, which was generalised in nature. She started vomiting approximately eight hours after initial trauma, which was greenish in colour and non-projectile. There was no history of loss of consciousness, Ear, Nose and Throat (ENT) bleed, haematemesis or melaena.
The child was then taken to the nearest doctor who advised ultrasonography of abdomen and pelvis which revealed diffusely oedematous jejunal loops, minimal ascites with internal septation due to duodenal or jejunal perforation. There were signs of generalised peritonitis.
On admission to our hospital, 24 hours post trauma, patient was febrile and she looked toxic with signs of dehydration. Physical examination revealed pulse– 134 beats/min and blood pressure was 86/66 mmHg. No bruises or other external injuries were noted. Abdominal examination revealed distension of abdomen with tenderness and guarding all over the abdomen. Shifting dullness was present and bowel sounds were absent.
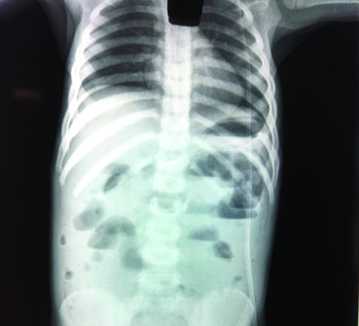
Routine blood investigations were done which were within normal limits other than raised total leucocyte count which was 13600/mm3 and decreased serum sodium which was 130 mmol/lit. Erect X-Ray abdomen showed gas under the diaphragm [Table/Fig-1]. Repeat ultrasonography and Computed Tomography (CT) abdomen was not done due to frank clinical diagnosis and considering the duration of trauma.
Erect X-ray abdomen: showing gas under the diaphragm.
Patient was planned for emergency explorative laparotomy. Right upper transverse incision was taken considering the age of patient. On exploration abdomen was found to be filled with bilious fluid. There was a single isolated jejunal perforation of size 3×2 cm at antimesenteric border, about 100 cm away from the ligament of Treitz [Table/Fig-2]. Jejunal loop of 15 cm was found to be gangrenous [Table/Fig-3]. The rest of the bowel and other organs were normal.
Isolated jejunal perforation - 3 x 2 cm in size.
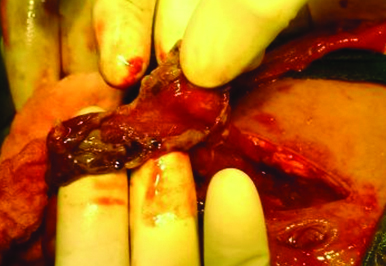
Jejunal loop gangrene of 15 cm.

Resection of gangrenous segment of jejunum and jejuno-jejunostomy was done. Drains were inserted and the abdomen was closed after thorough saline wash. Patient was started on antibiotics as per routine protocol. Postoperatively, drain was removed on fifth day and all sutures were removed on eighth day. The postoperative course was uneventful and the patient was discharged after 10 days.
Discussion
Trauma causes significant morbidity and mortality in paediatric age group with motor vehicle accidents causing most deaths [1]. Blunt Abdominal Trauma (BAT) can injure any abdominal organs. Isolated Jejunal Perforation (IJP) following BAT is extremely rare [2]. Although, majority of intestinal perforations are caused by Motor Vehicle Accidents (MVA) it can also result from physical assault, fall from height or injury caused by bicycle handle bar.
Blunt abdominal trauma causing perforation of the gastrointestinal tract is relatively infrequent with incidence of hollow visceral injury being <1%–8.5% [3,4]. Samuel Annan reported the first case of intestinal rupture secondary to blunt trauma [5]. IJP post blunt trauma is seen in less than 1% cases [2].
A sudden increase in intra-luminal pressure in a fluid or air-filled bowel loop causes perforations on the anti-mesenteric border. These perforations occur due to raised intraluminal pressure and not due to crushing hence, usually they are not surrounded by damaged tissue [6]. Delayed diagnosis of IJP has significant morbidity and mortality [7,8].
Trauma injuring abdomen is the third most common instance [2]. There are different mechanisms of injuries of blunt abdominal trauma in paediatric age group. MVA being most common followed by handlebar injury and fall from height [9]. Gastrointestinal tract injury following BAT is not so uncommon. Duodenal injuries are frequent following BAT and usually they are partial thickness injuries. Full thickness duodenal injuries are rare and observed only in 15% of cases [10]. Isolated jejunal perforation is furthermore rare and seen only in less than 1% of BAT patients [11].
Different mechanisms of small bowel perforation following BAT includes shearing forces, compression between vertebra and abdominal wall and blowout injury due to sudden increase in intra-luminal pressure of bowel loop [6]. Overall incidence of small bowel perforation post abdominal trauma appears to be lesser in children than adults [8].
Diagnosis of hollow visceral organ injury post BAT presents a significant challenge to surgeon. These injuries often pose a diagnostic dilemma due to usual non-specific and vague clinical signs.
Moderate to severe abdominal pain is the most frequent symptom seen in 64% of cases [2]. as it was in our case. Though none of the available data signifies about the duration of trauma and elicitation of pain, as in our case child was asymptomatic for initial four hours. Tenderness over the abdomen is the second most common sign seen in 46.7% of cases [2]. Proper history, detail physical examination and prolonged observation with repeated examination up to 72 hours are mandatory for proper diagnosis, as BAT can cause delayed perforation. In delayed perforation leading cause is compression necrosis of gut wall due to BAT [2]. Gas under diaphragm on erect X-ray chest or abdomen is seen in less than 50% of cases, that too in early hours of injury, limiting its usefulness [11]. Several other modalities such as Diagnostic Peritoneal Lavage (DPL), Computed Tomography (CT), Focused Abdominal Sonography for Trauma (FAST) and diagnostic laparotomy also been used for confirmation of bowel perforation.
Though, diagnostic laparotomy is the most confirmative method of diagnosis in cases of bowel perforation literature mentions about DPL being more sensitive specifically in the cases of IJP in early hours, more than CT scan [7]. In our case X-ray abdomen was the only available investigation, and any other radiological investigations were not done due to obvious clinical diagnosis and history of long duration post trauma.
Once the diagnosis is confirmed open or laparoscopic repair is the first and best line of treatment. Identification of site of perforation, drainage of septic peritoneal collection followed by proper saline lavage is usual intraoperative steps. Closure of perforation in simple two-layers is usual dictum for single isolated jejuna perforation [8] as done in our case.
Improper diagnosis and delayed decision to operate in such cases has significant impact on morbidity as well as on mortality but exact duration of delay is still the topic of controversy. According to available literature, delay of eight hours can result in increased morbidity and mortality [7]. Inspite of significant delay in presenting to us, our patient was taken for operation as early as possible and the outcome proved to be life saving for the child.
Conclusion
Earliest clinical diagnosis confirmed by available radiological modality is important with respect to morbidity and mortality outcome. Final step to be taken irrespective of confirmation or dilemma of diagnosis is emergency laparaoscopy or laparotomy as done in our case which proved to be life saving for patient.
[1]. American College of Surgeons. Paediatric TraumaAdvanced Trauma Life Support for Doctors 1997 Chicago:355-76. [Google Scholar]
[2]. Goyal S, Garg MK, Single jejunal blowout perforation following blunt abdominal trauma: diagnostic dilemmaJ Mahatma Gandhi Inst Med Sci 2013 18:144-46. [Google Scholar]
[3]. Canty TG, Brown C, Injuries of the gastrointestinal tract from blunt abdominal injuries in childrenJ Trauma 1999 46:234-40. [Google Scholar]
[4]. Albanes CT, Meza MP, Gardner J, Smith SD, Rowe MI, Lynch JM, Is computed Tomography a useful adjunct to the clinical examination for the diagnosis of paediatric gastrointestinal perforation from blunt abdominal traumaJ Trauma 1996 403:417-21. [Google Scholar]
[5]. Chiang WK, Isolated jejunal perforation from non-penetrating abdominal traumaAm J Emerg Med 1993 11:473-75. [Google Scholar]
[6]. Robbs JV, Moore SW, Pillay SP, Blunt abdominal trauma with jejunal injury: A reviewJ Trauma 1980 20:308-11. [Google Scholar]
[7]. Fakhry SM, Brownstein M, Watts DD, Baker CC, Oller D, Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: An analysis of time to operative intervention in 198 patients from a multicenter experienceJ Trauma 2000 48:408-15. [Google Scholar]
[8]. Thompson SR, Holland AJ, Perforating small bowel injuries in children: influence of time to operation on outcomeInjury 2005 36:1029-33. [Google Scholar]
[9]. Abbas S, Upadhyay V, Hollow viscus injury in children: Starship hospital experienceWorld Journal of Emergency Surgery 2007 2:14 [Google Scholar]
[10]. Ballard RB, Badellino MM, Eynon CA, Spott MA, Staz CF, Buckman RF, Duodenal rupture: A 6-year state wide experienceJ Trauma 1997 43:229-32. [Google Scholar]
[11]. Allen GS, Moore FA, Cox CS Jr, Wilson JT, Cohn JM, Duke JH, Hollow visceral injury and blunt traumaJ Trauma 1998 45:69-78. [Google Scholar]