Cubitus varus deformity is the most common late complication after supracondylar fracture of distal humerus in children, incidence varying from 4% to 58% [1,2].
Elbow injuries are common in skeletally immature children, between 5-10 years of age [3,4]. Metaphyseal area of the distal humerus is the weakest region around the elbow, so supracondylar fractures are the most common elbow injuries. Also, the frequent falls in small children while playing, cycling or fall inside the house from bed, sofa has added to the increase in incidence. Non dominant side and boys have a more predilection to such injuries than dominant side and girls. Associated vascular injuries in 1% of the cases and nerve injuries involving median and radial nerve in atleast 7% of the cases adds to the concern [5,6]. Increased ligamentous laxity also correlates with the occurrence of supracondylar fracture. Fractures in this region need aggressive treatment and proper rehabilitation protocol to gain better functional outcome. Different methods have been used for the treatment of supracondylar fractures. Most can be reduced by manipulation and closed reduction, some require open reduction. Adequate reduction is assessed fluoroscopically by Baumann’s angle, formed by the physeal line between the lateral condyle and the line touching distal humeral articular margins and perpendicular with the long axis of the humerus. Difficulty arises in maintenance of the reduction which can be done by immobilization, closed percutaneous pinning or internal fixation.
Cubitus varus or bow elbow or gunstock deformity is the result of malunion occurring as a complication of supracondylar fracture of the humerus. It occurs in only the extension type of supracondylar fracture of the humerus, causing a reduction or loss of the carrying angle.
Various aetiologies have been suggested. The usual aetiology of cubitus varus deformity is malunion of distal humeral fragment rather than growth disturbance [7]. Osteonecrosis with or without growth arrest is rare but a very important cause of varus deformity [8].
Cubitus varus deformity has no tendency for spontaneous correction but it always has to be corrected. Treatment options include:
The various osteotomies performed can be fixed using metal plates, stainless steel wires, screws and staples. Unstable internal fixation allows the osteotomy fragment to slip into a varus position in a number of patients [14].
It has been found that dome osteotomy provides maximum stability of maintaining the correction, avoids lateral condyle becoming more prominent and its scar is more cosmetically acceptable. [Table/Fig-1] shows the comparison between lateral closed wedge osteotomy and dome osteotomy in terms of lateral condyle prominence.
The technique of dome osteotomy was initially mentioned by Tachdijan but he gave only theoretical description of the technique [13]. This was followed by Higaki T and Ikuta Y who reported this procedure [15].
Kirschner wire fixation or plate fixation can be used to hold the fragments and elbow immobilized post operatively with a POP cast for three-four weeks. If the fragments can be stabilized with a rigid fixation, early post operative movements can be gained, thus giving a hope of good range of movements and excellent functional outcome.
Closed dome osteotomy has various advantages like a cosmetically better scar due to minimally invasive procedure, no lateral prominence of elbow, no lateral translation of humero-ulnar axis, all rotational and angulational deformities can be corrected simultaneously and early mobilization and rehabilitation [16].
This study was done to evaluate the results of closed dome osteotomy for correction of cubitus varus deformity, after malunited supracondylar fracture of humerus in children.
Materials and Methods
The present prospective study consisted of 25 cases of either sex in children with malunited supracondylar fracture of distal humerus (cubitus varus deformity) admitted in orthopaedics department. This study was performed from June, 2010 to October, 2012.
The inclusion criteria were; age of patient less than 15 years, varus deformity due to malunited supracondylar fracture of humerus and the parent’s concern for cosmetic appearance of elbow.
The exclusion criteria included parent’s/patient’s refusal for surgery and age of patient more than 15 years.
An informed written consent of the parents was obtained before inclusion in this study. Approval from the Ethical Committee was taken for the study and inclusion of patients, in accordance with the Helsinki Declaration of 1975 (revised 2000).
Clinical history, general physical examination and local examination were performed. Patient was investigated for operative anaesthetic purposes. Supportive and prophylactic therapy in form of physiotherapy was given.
Preoperative Assessment
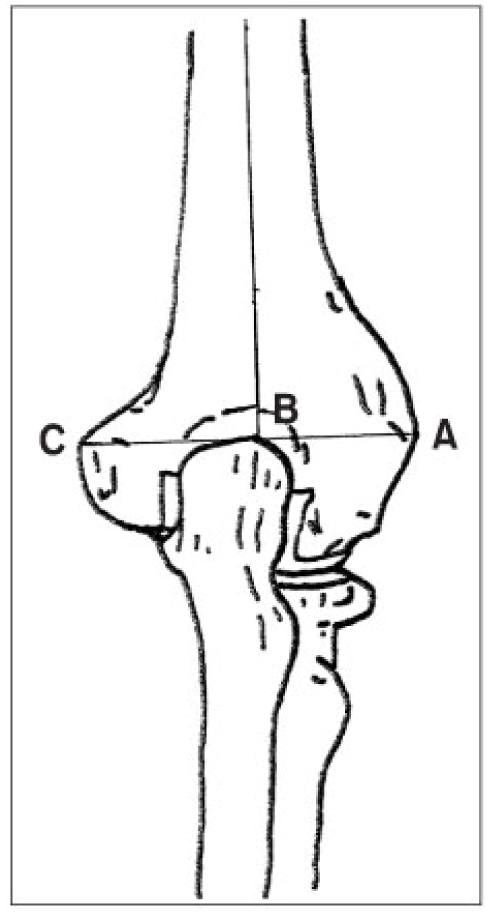
Anterio-posterior and lateral radiographs of elbow were taken with elbow in full extension and forearm in full supination [Table/Fig-2]. The humerus-elbow-wrist angle was measured on both sides using the Oppenheim method and the angle of correction was estimated [Table/Fig-3]. The LCPI was calculated on the affected side as described by Wong HK [17], using the formula {LCPI= (AB-BC)/AC*100}, where B is the crosslink between a line connecting the lateral prominence A, the medial prominence C and the longitudional mid-humeral axis [Table/Fig-4]. Range of motion of the affected elbow was noted, along with complaints of cosmesis, pain and loss of motor power and sensation.
Preoperative X-ray and clinical photo.

Humerus-elbow-wrist angle measured using the Oppenheim method.

Calculating the lateral condylar prominence index.
Preoperative Plan for Osteotomy
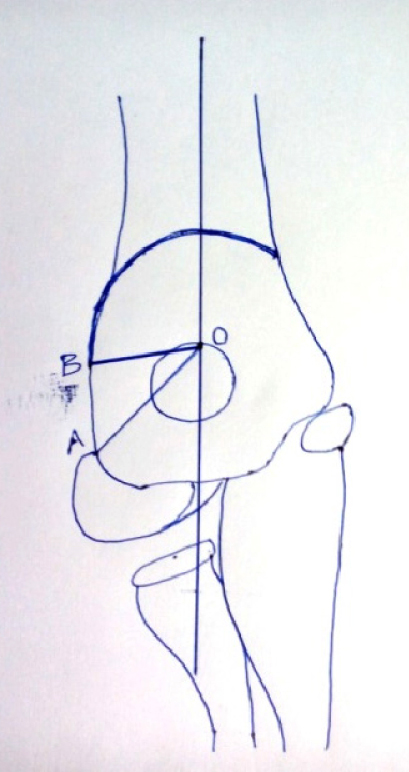
The mid humeral axis was drawn over the Anterio-posterior (AP) radiograph of the affected side. A point (point O) was marked where this axis cut the olecranon fossa, another point (point A) was marked at the junction of lateral condylar epiphysis with distal humerus. Point O and point A were joined. Then the angle of correction making OA as base was drawn. Another point was made where this angle cut the distal humerus (point B). Now O becomes the centre of the dome and OB the radius of the dome. With this radius a dome was drawn. The arc of the dome was the proposed site of osteotomy as shown in [Table/Fig-5].
Mid humeral axis over the AP radiograph of the affected side to propose the site of osteotomy;
Surgical Technique
All the necessary aseptic precautions and preparations were done for the surgery. A Moore’s pin was passed from posterior to anterior just proximal to olecranon fossa and perpendicular to the coronal plane of humerus. A stab incision was given at the margins of humerus and periosteum elevated. Multiple holes in a dome shape were drilled with help of Small Dynamic Compression Plate (SDCP) Mounted on the moore’s pin which was used as jig. A K-wire was passed distal to the osteotomy site, parallel to the articular surface. Another K-wire was passed parallel to this wire. Two K-wires were also passed proximal to osteotomy site from lateral to medial side. The osteotomy holes were connected with help of 10 mm osteotome to complete the break in the bone. Deformity was corrected under fluoroscopy by translating the distal fragment and derotating if required. The K-wires were connected with mini external fixator which was used as lateral tension band. An additional K-wire was used if stability was in doubt. In addition, a ledge excision was done prior to dome osteotomy in cases where anterior ledge was present which restricted the flexion movement at elbow.
Postoperative Protocol
The limb was put to rest in an arm sling. Exercise was started once the patient was pain free. Postoperative X-ray was taken [Table/Fig-6], carrying angle and LCPI were calculated. X-ray was repeated after four weeks. K-wires and fixator were removed when there was sufficient union. Follow up was done every four weeks with X-rays till complete radiological union and complete expected results were obtained. At final follow up carrying angle, LCPI and range of motion at elbow were checked [Table/Fig-7]. Parents and patients were asked about the cosmetic satisfaction with results. Result was graded according to Mitchell and Adams Criteria [18] as under:
Final follow-up X-ray and clinical photo.

Excellent: Change in the carrying angle of less than 50, restriction of movement in any plane less than 100.
Good: Change in the carrying angle from 50 to 150 (i.e., not beyond cubitus rectus), restriction of flexion, extension or rotation by 100 to 200.
Unsatisfactory: When the changes surpass the above mentioned limits.
Results
In our study, 68% of the cases were male, rest female. Almost 84% of the patients were in 5-10 years of age group while remaining 16% were of one to five years of age. Nearby, 56% of the cases involved left sided deformity while remaining 44% had right side involvement.
Carrying angle on the normal side was more in females (average 11.50) than in males (average 10.10). Carrying angle on the affected side pre operatively and post operatively is shown in [Table/Fig-8].
Carrying angle on the affected side pre operatively and post operatively.
| Carrying angle (Pre operative) | No of Patients | Percentage | Carrying angle (Post operative) | No of patients | Percentage |
|---|
| 0 to -10 | 5 | 20.0 | 0 to 5 | 2 | 8.0 |
| -11 to -20 | 13 | 52.0 | 6 to 10 | 14 | 56.0 |
| Less than -20 | 7 | 28.0 | >10 | 9 | 36.0 |
| Total | 25 | 100.0 | Total | 25 | 100.0 |
Degree of deformity, calculated by subtracting the carrying angle on affected side from the carrying angle on normal side, was found to be 110 to 20 in 16% of the patients, 210 to 30 in 36% of patients, more than 30 in 48% of patients, while no patient had 00 to 10 of deformity.
Lateral Condyle Prominent Index (LCPI)
Pre operative LCPI ranged from -7.60% to +10.64%, average being +1.18%. Post operative LCPI decreased, ranging from -9.09% to +3.00%, average being -2.75%. Change in LCPI ranged from +5.0% to -10.7%, with an average of -2.75%. Decrease in LCPI resulted in better cosmetic appearance of elbow after surgery.
Range of Motion at the Elbow
Pre operatively eight patients (32%) had limitation of flexion while three pateints (12%) had limited extension. Rest 14 patients (56%) had normal range of motion at the elbow. Post operative range of motion is shown in [Table/Fig-9].
Post operative range of motion at elbow.
| Postoperatively Range of Motion | No of patients | Percentage |
|---|
| Increased | 11 | 44 |
| Decreased | 0 -10 311 -20 1>20 0 | 16 |
| Full prior motion who regained their full range | 10 | 40 |
| Total | 25 | 100 |
Complications
In this series no long term complications were observed. A few complications occurred are as shown in [Table/Fig-10]. One case of radial nerve neurapraxia occurred which recovered within three months period.
| Complications | No of patients | %age |
|---|
| Neurological injury | 1 | 4 |
| Vascular injury | 0 | 0 |
| Postoperative oedema | 4 | 16 |
| Infection | 4 | 16 |
| Loss of correction | 0 | 0 |
| Implant failure | 0 | 0 |
| Scar | 0 | 0 |
| Lateral bump | 0 | 0 |
| Total | 9 | 36 |
Time of Osteotomy Union
Time of union ranged from four to eight weeks with an average of 6.3 weeks. Union occurred within four weeks in three cases (12%), while 15 cases (60%) showed union time from four to six weeks. Rest seven cases (28%) showed union within eight weeks.
Evaluation of results
In our series we were able to achieve our aim of cosmetic correction of varus which the patients and their parents reported subjectively also. According to Mitchell and Adams Criteria, result are shown in [Table/Fig-11].
Results of our study according to Mitchell and Adams criteria.
| Results | No of patients | %age |
|---|
| Excellent | 22 | 88 |
| Good | 03 | 12 |
| Poor | 00 | 00 |
| Total | 25 | 100 |
Discussion
Cubitus varus is one of the most common complication of supracondylar fracture of humerus in children treated with non operative management without reduction and fixation, incidence of which varies from 4% to 58%. Most surgeons consider the deformity to result from inadequate reduction that leaves a residual rotatory deformity that can collapse into medial tilt and result in a varus deformity. In India, such injuries are still commonly handled by local bone setters rather than a certified orthopaedician. Most of the patients in this series were mainly the result of this practice. All the cases were treated conservatively with no history of any associated injuries. In cubitus varus, child often presents to improve the unsightly deformity, functionally the limb is not greatly disturbed.
In this study, all 25 cases presented for correction of deformity, eight patients had associated restricted movements at elbow joint due to anterior ledge. Parent’s concern was the major indication for surgery.
The lateral closing wedge osteotomy is the most commonly used procedure to correct the deformity. However, the appearance of the joint post surgery is different from the unaffected side, although the carrying angle was matched. Since this procedure does not allow translation of the distal humerus, the residual cosmetic appearance might be due to a radial shift of distal fragment causing a protrusion of the lateral condyle. Wong HK et al., reported an incidence of 64% of this complication in a series of 22 patients [17].
Apart from lateral condylar prominence, lateral closing wedge osteotomy has another pitfall, the centre of rotation of distal humeral fragment is located at the medial cortex, making a large rotation arc necessary for correction of deformity. This results in further tightening of the already contracted medial structures and a large varus movement acting on the osteotomy site. In this situation, the osteotomy is mechanically unstable and loss of correction would occur easily if the fixation were inadequate [19].
On the other hand, dome osteotomy uses the midline of the humerus as the centre of rotation, therefore the distal fragment does not shift laterally and is thus prevented from becoming prominent. Also, the rotation required for correction is less producing a much smaller varus moment, making the osteotomy mechanically more stable. Additionally, the muscles attached to distal fragment pull distal dome into claws of proximal fragment, reinforcing the stability [20].
Ippolito E et al., reported 60% patients with unattractive post operative scar after open dome osteotomy [21]. However, we performed percutaneous dome osteotomy. So none of the patient had unattractive scar except one in whom ledge excision was done.
Male to female ratio was 17:8 and the age group of our patients was 4 to 10 years with an average of 7.7 years.
In the past, open approach either with triceps splitting or olecranon osteotomy was used to approach distal humerus. Reduction was fixed using various mechanisms. Langenskiold A and Kivilaakso R used a metal plate with screw for internal fixation [22]. Carlson CS Jr and Rosman MA described use of lateral closing wedge osteotomy with staple fixation [23]. French PR advised a lateral closing wedge osteotomy and internal fixation with two parallel screws and stainless steel wire [24].
In this study, only stab incisions were given to reach at the osteotomy site under fluoroscopic guidance and reduction was fixed with mini external fixator on lateral side. This stable fixation allowed us to commence physiotherapy in immediate post operative period.
In our series 21 out of 25 patients (84%) reported no loss of range of motion arc and four patients had loss of range of motion. In contrast, all series of French osteotomy reported loss of range of motion arc in a significant number of patients. Bellemore M et al., reported loss of range of motion in 77% of patients after French osteotomy [25]. Considering the results of our study, we are not aware of any previous study in which 44% patients reported gain in range of motion arc and 40% patients reported no loss or gain in range of motion arc. This can be attributed to early commencement of physiotherapy actively and passively which was possible due to stable fixation. Other contributory factors were minimal soft tissue handling and prevention of anterior angulation.
Upon analysing the results we found that 22 out of 25 patients carrying angle was within 5° of contralateral elbow which was assigned as excellent outcome.
In all series of dome osteotomy, LCPI improved indicating that dome osteotomy is better than French osteotomy in term of prevention of lateral condyle from being prominent.
In a study done by Tien YC et al., on 15 patients, the pre operative carrying angle ranging from 19° to 31° varus showed improvement to post operative carrying angle ranging from 7° to 15° valgus. Also, the pre operative and post operative differences of LCPI ranged from -67% to +6%, average being -30.1% [16].
Our study showed the same improvement in LCPI which improved in all but one patient gave good cosmetic outcome after a surgery which was done primarily for cosmetic purpose.
In this study we did not find any loss of correction and one of our patient suffered from complications like neuropraxia of radial nerve and four of our patients suffers from superficial pin tract infection and none of our patient suffers from complications like brachial artery aneurysm, haematoma formation etc., which was seen in previous groups. All patients in our series were willing to get the surgery repeated under same circumstances.
In our observation, we found that in younger age group rotation of dome and correction of deformity was easier which was difficult in older age group due to tight soft tissue structures.
In our study, the results of deformity correction, in terms of elbow range of motion, were comparable to lateral closed wedge osteotomy in various other studies. The outcome in terms of lateral condyle prominence, cosmesis, maintenance of correction and complications were superior in our study as compared to lateral closing wedge osteotomy in other studies [26]. The results of percutaneous dome osteotomy for correction of post traumatic cubitus varus in our series were comparable to those of lateral closing wedge osteotomy by various authors in terms of preservation of elbow movement and superior in terms of lateral condyle prominence, maintenance of correction, cosmetic outcome and complication. Such superior results were attributed to thorough pre operative planning and meticulous intraoperative procedure along with percutaneous technique and mini external fixator used which gave stable fixation for early rehabilitation.
Limitation
Most of the patients visiting in orthopaedics department with supracondylar fracture of humerus having cubitus varus deformity were of lower socio-economic strata and from far fetched areas. Loss of follow was a major limitation of this study.
Conclusion
Closed dome osteotomy for the correction of cubitus varus deformity is safe and effective method which gives near normal elbow and no post operative scar, cosmetically more acceptable to the parents.