Stroke is defined as a sudden onset of focal neurological deficit lasting for more than 24 hours with no apparent cause other than vascular origin. The 24 hours threshold in the definition excludes Transient Ischemic Attacks (TIA) [1]. Stroke is classified depending upon its aetiology into either ischemic stroke (85%) or haemorrhagic stroke (15%) [1,2] about 80% of strokes are thromboembolic in origin and the embolus arises from the carotid plaque [3]. Early detection of the atheromatous changes in the carotid artery will reduce the stroke related morbidity and mortality. Sonographic evaluation of the carotid arteries, are used for risk assessment; on gray scale, CIMT in common carotid artery is evaluated on gray scale ultrasound [4]. The plaques are characterized as echogenic, calcified or hypoechoic or associated with intraplaque haemorrhage and surface ulceration and percentage stenosis [5]. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) and European Carotid Surgery Trialists (ECST) collaborative group showed a benefit of carotid endarterectomy for recently symptomatic patients with internal carotid lumen diameter narrowing of 70% or more [6]. In the present study, all patients with neurologic deficits underwent Non-Contrast Computed Tomography (NCCT) brain and diagnosis of acute ischemic stroke was made. Then retrospectively patients were evaluated by the carotid doppler sonography to find out the prevalence of carotid artery stenosis in acute ischemic stroke patients. Association between carotid artery stenosis and various risk factors such as diabetes mellitus, hypertension, hyperlipidemia, smoking and age was determined by taking detailed clinical history, laboratory investigations and examination of the patients.
Materials and Methods
The present study was a hospital based prospective study conducted in Rajindra Hospital Patiala, Punjab, India, in patients who presented with clinical symptoms of acute ischemic stroke. The study was conducted on 50 patients over a period of three years from 2010-2013. Institutional review board approval for conducting this study was obtained and informed consent of study patients was taken. Patients in which the duration of stroke was less than one week, head injury and haemorrhagic stroke patients were excluded from the study. Detailed clinical history was taken from each patient. This included- age, sex and risk factors such as hypertension, diabetes mellitus, hyperlipidemia (Serum cholesterol, triglyceride levels), and smoking. The study required the lipid profile, CT scan brain, carotid doppler, blood pressure, post-prandial blood sugar and fasting blood sugar. CT scan was performed with Siemens-Somatom Emotion 6 slice third generation spiral CT. Doppler sonography was performed with Philips Envisor ultrasound machine and Philips HD 11E 3D and 4D machine with 7.5 Mhz linear array transducer. All patients’ detail including serum lipid profile, blood sugar level and blood pressure were obtained from their admission file records.
Carotid Colour Doppler Examination Technique
Carotid arteries were examined with patient in the supine position. Neck exposure was enhanced by tilting and rotating the head away from the side being examined, and ipsilateral shoulder being dropped as far as possible. The examiner was seated at the right side of the patient. The posterolateral and far posterolateral transducer positions were used to examine the carotid arteries in long axis (longitudinal). Short axis (transverse) views of the carotid arteries were obtained from an anterior, lateral or posterolateral approach. All the examinations were performed by the same operator with a Doppler angle of 60°.
On gray scale, presence or absence of plaque, location of plaque and plaque characteristics such as echo pattern, calcification, any ulceration or intra-plaque haemorrhage were evaluated.
On Doppler study, PSV and EDV of CCA, ICA and ECA were evaluated. Criteria used for measuring percentage of stenosis in our study: (a) ICA/CCA PSV ratios; and (b) Residual lumen diameter at most stenotic portion.
Statistical Analysis
The collected data was statistically analysed and R-value test of significance was applied by using SPSS 16.0 version software.
Results
In present study, out of 50 patients, 30 (60%) patients were males and 20 (40%) were females. Out of the 50 patients studied, 28 patients had ischemic stroke on right side and 21 had ischemic stroke on left side. One had bilateral involvement. On right side, 13 patients had anterior circulation infarct, 11 patients had posterior circulation infarct and four had watershed zone involvement. On the left side, 11 patients had anterior and five had posterior circulation stroke and five patients had watershed zone infarct. MCA territory was most commonly involved in anterior circulation stroke [Table/Fig-1]. Out of 21 MCA stroke patients, 10 had right-sided and 11 had left-sided stroke [Table/Fig-2].
Axial Computed Tomography (CT) image shows Left MCA and right PCA territory infarct (arrows).
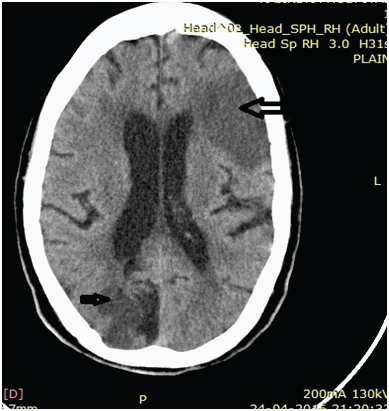
CT scan findings in stroke patients.
| CT Findings | No. of Patients | Percentage |
|---|
| Right MCA | 10 | 20.0 |
| Right ACA | 02 | 4.0 |
| Right AICA | 01 | 2.0 |
| Right PCA | 07 | 14.0 |
| Right PICA | 04 | 8.0 |
| left MCA | 11 | 22.0 |
| Left PCA | 02 | 4.0 |
| Left PICA | 03 | 6.0 |
| Left MCA/ACA | 2 | 4.0 |
| Right MCA/ACA | 1 | 2.0 |
| Right MCA/PCA | 3 | 6.0 |
| Left MCA/PCA | 3 | 6.0 |
| Right MCA Left PCA | 1 | 2.0 |
| Total | 50 | 100.0 |
MCA-middle carotid artery, ACA-anterior cerebral artery, PCA-posterior cerebral artery, PICA-posterior inferior cerebral artery, AICA-anterior inferior cerebral artery
A total of 31 patients had extracranial carotid artery stenosis, out of which 19 were males and 12 were females. Maximum number of patients who had stenosis belonged to 51-60 years of age group. Twenty patients had <50% stenosis. Seven had 50-69% stenosis. Three had ≥70% stenosis [Table/Fig-3,4]. One had complete occlusion. Nine patients had significant stenosis >60% [Table/Fig-5,6].
Distribution of patients with maximum stenosis with age and sex.
| Age Group (in years) | Gender | Stenosis % | Complete occlusion |
|---|
| Normal | Mild<50% | Moderate50-69 % | Severe≥70 % |
|---|
| 31-40 | Male | 0 | 0 | 0 | 0 | 0 |
| Female | 0 | 1 | 0 | 0 | 0 |
| 41-50 | Male | 5 | 1 | 0 | 0 | 0 |
| Female | 0 | 1 | 0 | 0 | 0 |
| 51-60 | Male | 4 | 6 | 0 | 0 | 0 |
| Female | 3 | 1 | 3 | 0 | 0 |
| 61-70 | Male | 4 | 2 | 2 | 0 | 1 |
| Female | 1 | 2 | 1 | 1 | 0 |
| 71-80 | Male | 2 | 2 | 0 | 1 | 0 |
| Female | 0 | 2 | 0 | 0 | 0 |
| 81-90 | Male | 0 | 2 | 1 | 1 | 0 |
| Female | 0 | 0 | 0 | 0 | 0 |
| Total | 19 | 20 | 7 | 3 | 1 |
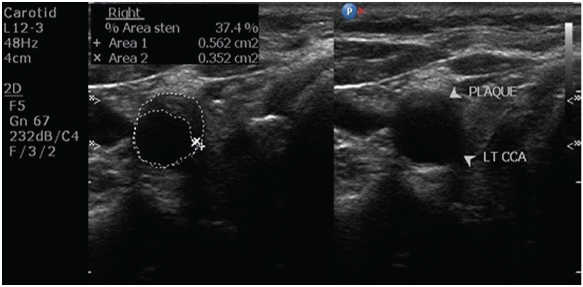
Ultrasound image shows plaque in common carotid artery with area of stenosis being 37.4%.
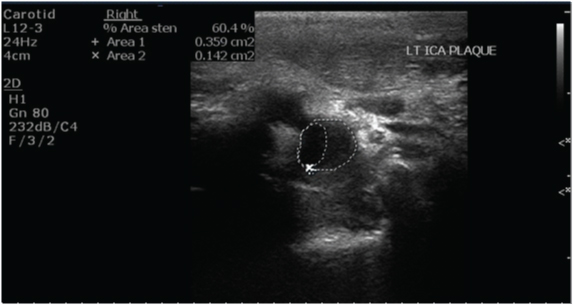
Ultrasound image shows significant stenosis (60.4%).
Percentage of significant stenosis.
| Stenosis | Right side | Left side | Bilateral stenosis |
|---|
| <60% | 17 | 10 | - |
| >60% | 5 | 02 | 2 |
| Total | 22 | 12 | 02 |
CIMT in present study was higher in males as compared to females and this difference was statistically significant (p-value <0.05). Most common location of plaque was carotid bulb [Table/Fig-7]. A total of 19 plaques were noted in carotid bulb region out of 49 total plaques (38.7%). Next most common location was CCA itself. Least common location was ECA. Out of total 49 plaques, 29 plaques were present on right side and 20 plaques on left side. Echogenic plaques were most commonly noted on both sides [Table/Fig-8] and ultrasound picture showing echogenic thrombus in [Table/Fig-9]. No intraplaque haemorrhage/ulceration seen in the present study.
| Plaque Location | Number of plaques | Percentage |
|---|
| Common Carotid Artery (CCA) | 15 | 30.6 |
| Carotid Bulb | 19 | 38.7 |
| Common Carotid Artery Bifurcation | 5 | 10.2 |
| Internal Carotid Artery (ICA) | 9 | 18.3 |
| External Carotid Artery (ECA) | 1 | 2 |
| Total | 49 | 100 |
| PlaqueCharacterisation | Right | Left |
|---|
| No. ofPatients | Percentage | No. ofPatients | Percentage |
|---|
| Hypoechoic | 09 | 31.0 | 05 | 25.0 |
| Echogenic calcified | 04 | 13.7 | 04 | 20.0 |
| Echogenic | 16 | 55.2 | 11 | 55.0 |
| Total | 29 | 100 | 20 | 100 |
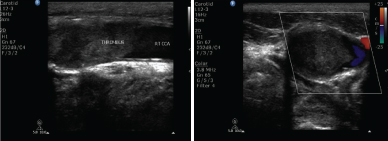
Carotid doppler sonography images show echogenic thrombus in a common carotid artery completely occluding its lumen.
Hypertension and diabetes were the most prevalent risk factors for cerebral ischemic stroke. Out of total 50 patients, 32 had hypertension (64%) and 22 had diabetes (44%).
R-value of statistical significance was applied. R-value signified positive correlation between various risk factors, CIMT and percentage stenosis. Hypertension was the most common risk factor associated with stenosis and increased CIMT [Table/Fig-10], second most common risk factor was hyperlipidemia (both of these showed positive correlation with stenosis and increased CIMT) [Table/Fig-11].
Association of risk factors with CIMT and stenosis.
| RiskFactors | Total patients havingspecified risk factors | Patientshavingstenosis(percentage) | CIMT≥ 0.09 | R-value(MultipleLogisticRegression) |
|---|
| Hypertension | 32 | 25 | 22 | 0.275 |
| Hyperlipidemia | 10 | 6 | 6 | 0.048 |
| Diabetes | 22 | 13 | 4 | 0.034 |
| Smoking | 14 | 7 | 6 | 0.028 |
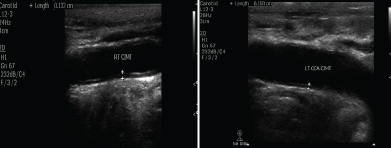
Ultrasound images show increased CIMT (carotid intima media thickness) on both sides.
Discussion
Distribution of Stroke
In present study, 28 patients had ischemic stroke on right side and 21 had ischemic stroke on left side. One had bilateral involvement. Anterior circulation infarct was more common than posterior circulation infarct. MCA territory stroke was the most prevalent [Table/Fig-2]. This result was different from the study conducted by Baidya OP et al., in which imaging findings showed that majority of the patients (52%) had left side lesion in brain and anterior circulation was the most common territory involved in the brain [7].
Ischemic Stroke and Risk Factor Association
Age: The incidence of stroke increases after 60 years of age according to previous studies [8]. Most patients belonged to 51-60 years of age group (34%), in which 10 were males and seven were females. Next most common age group was 61-70 years (28%) in which nine were males and five were females. Iemolo F et al., in his study showed that only 2.5% of stroke victims were females [9]. In present study, 30 (60%) patients were males and 20 (40%) were females.
Hypertension: Hypertension was most prevalent risk factor (64%) seen in present study. Atherosclerosis in hypertension results from the continuous trauma to the endothelium and ultimately leads to the plaque formation and contributes to plaque growth [9]. [Table/Fig-12] shows that mean systolic blood pressure in females was more as compared to males and these results were comparable with study done by Philip A et al., [10].
Comparison of mean Systolic Blood Pressure (SBP) of present study with previous study.
| Study | Gender | Systolic blood pressure (mm Hg) |
|---|
| Philip Aet al., [10] | MalesFemales | 139.3 mmHg142.8 mmHg |
| Present study | MalesFemales | 144.58 mmHg157.25 mmHg |
Garg S et al., demonstrate the association of risk factors with wall thickness and stenosis by using multiple regression analysis. In this study, risk factors such as diabetes, smoking, hyperlipidemia and cardiac disease showed maximum mean values. Smoking and heart disease showed maximum positive correlation with stenosis [11]. In present study, hypertension and hyperlipidemia showed maximum mean values and positive correlation with stenosis.
Diabetes mellitus: It is recognized significant risk factor. Plasminogen activator antigen and plasminogen activator inhibitor-1 levels have been significantly associated with ischemic stroke in diabetic patients [12]. In present study, 22 patients were diabetic (36.66%) out of 50 acute ischemic stroke patients. Out of 22 diabetic patients, nine were normal, 8 (44%) patients had <40% stenosis, 4 (18.18%) patients had >40% stenosis and one had complete occlusion (4.5%). This result was comparable with study done by Sethi SK et al., in which out of total 16 diabetics patients, five were normal [13]. Eight had <40% stenosis, two had >40% stenosis and one had complete occlusion [13].
Cigarette smoking: Chronic cigarette smoking is a strong predictor for severe extracranial carotid atherosclerosis [14]. In present study, smoking was the least common factor associated with increased CIMT and stenosis, may be due to the fact that the study was conducted in Punjab and prevalence of smoking in Punjab is less (3%) as compared to other states [15].
Ischemic Stroke and Carotid Parameters
Carotid Intima Media Thickness (CIMT): CIMT is related to adaptive hypertrophy of the media layer and not a true representation of an atherosclerotic lesion [16]. Increased CIMT may be represented by “fatty streaks” composed of foamy macrophages which have a non-raised appearance in the arterial lumen. In contrast, “pathologic intimal thickening” is increased CIMT, which represents the earliest manifestation of progressive atherosclerosis [17]. In present study, 0.09 cm was taken as a cut-off value for increased CIMT.
In present study, mean CIMT in males 0.091±0.021 and in females 0.082±0.020 [Table/Fig-13]. This difference in CIMT was statistically significant (p-value<0.05) [18,19].
Comparison of CIMT of present study with previous studies.
| Study | Mean CIMT males | Mean CIMT females |
|---|
| Vicenzini Eet al., [18] | Right (R) 0.98±0. 18Left (L)1.02±0.21 | R 0.90±0.18L 0.92±0.19 |
| Riccio SA et al., [19] | Overall 0.88±0. 15 | Overall 0.84±.20 |
| Present study (2014) | R 0.097333L 0.089666Overall 0.091±0.021 | R 0.0835L 0.082Overall 0.082±0.020 |
Plaque: Atherosclerotic disease involves extracranial carotid arteries usually within 2 cm of the carotid bifurcation in approximately 30-60% patients [6]. Carotid sonography is unique among vascular imaging procedures in that it can assess plaque location and composition. Plaque features marked by carotid Doppler may be useful for selection of medical and surgical therapy [8]. Most common site of plaque in present study was carotid bulb (38.7%) [Table/Fig-7]. Plaques seen on ultrasonography of carotids were classified in many different ways in the previously done studies. In present study, we took into consideration the location and morphology of the plaque along with its characteristics. Plaque characteristics such as echogenic, hypoechoic or calcified and whether ulcerated or smooth or any intraplaque haemorrhage were studied. Most of the plaques in present study were echogenic and smooth. No surface ulceration/intraplaque haemorrhage was seen in any of them. Intraplaque haemorrhages in the carotid plaques lead to frank ulceration and severe luminal narrowing due to rapid progression [6]. Consistent with the study done by Sethi SK et al., and Petrovic S et al., the most common location for plaque formation is the carotid bulb [13,20]. This is due to the fact that there is a sudden and rapid change in the velocity and direction of blood in the bulb region leading to increase in stress faced by the arterial walls and thus, having higher propensity to get damaged [21].
Carotid Stenosis
Two methods were used in two large population based studies that were done to quantify the carotid stenosis using catheter angiography (the gold standard). One of these two studies was the NASCET which used the criterion of diameter reduction and the other one was ECST [6]. The measurement of carotid stenosis in the present study was done using the method of percentage area reduction [6,20]. Normal CCA Doppler waveform is shown in [Table/Fig-14]. In the previous literature, different authors observed that one of the three major Doppler parameters that is, PSV, EDV, or PSV ratio is the most accurate predictor of clinically significant ICA stenosis [6]. As the ratio compensates from patient to patient physiological variability and also compensate for instrument variability, PSV ratio has been considered best for assessing stenosis. NASCET demonstrated that the long-term benefits of endarterectomy were significantly greater than medical treatment in patients with 60% or 70% ICA stenosis, whether symptomatic, or asymptomatic. Also, the endarterectomy trials established 60–70% diameter reduction as clinically significant levels of ICA stenosis. ICA/CCA, PSV ratio of >1.8 is an indicator of 60% or greater and a ratio of 3.7 is an indicator of more than 80% diameter stenosis. If PSV ratio >1.5 is an indicator of 50% or greater stenosis. It has been found that the ratio is more accurate than PSV [6]. In present study, ICA/CCA PSV ratio of >1 was indicative of <50% stenosis, ratio >2 indicative of 50-69% stenosis and ratio >3 is indicative of >70% stenosis. By using this criteria of ICA/CCA ratio, out of 50 patients, 20 patients had <50% stenosis. Seven had 50-69% stenosis. Three had ≥70 % stenosis. One had complete occlusion. Nine patients had significant stenosis >60%.
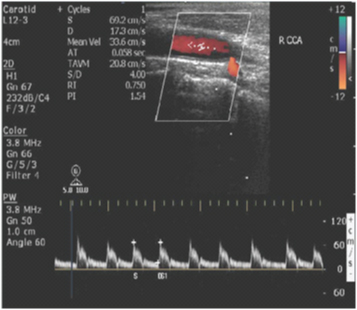
Carotid doppler image shows waveform with normal PSV and EDV in right common carotid artery (R CCA).
In view of the above mentioned findings, the role of carotid sonography in detecting the site and morphology of plaque and quantifying the degree of stenosis is well justified especially in high risk patients. Most patients in present study belonged to 51-60 years of age group. Hence, patients aged above 50 years with the risk factors mentioned in the study should undergo screening of extracranial carotid arterial system by duplex sonography.
Limitation
Some patients of acute ischemic stroke presented in debilitated and unconscious states which resulted in difficult patient’s positioning during carotid doppler examination. Large calcified plaques obscured the area of examination due to posterior acoustic shadowing. In patients with high carotid bifurcation, external and internal carotid arteries could not be evaluated properly.
Conclusion
In the present study, anterior circulation stroke was more common than posterior circulation stroke with MCA territory being the most prevalent site of ischemic stroke. Hypertension and diabetes were most prevalent risk factors for stroke. Hypertension and hyperlipidemia showed maximum mean R-values and positive correlation with stenosis and increased CIMT. Smoking was the least common factor associated. Most common site of plaque was carotid bulb. Echogenic plaques were most commonly noted on both sides. Doppler sonography is a safe, non-invasive, accurate and less time consuming method of diagnosing carotid stenosis. The present study highlights the importance of doppler sonography in stroke patients through surveillance of various risk factors that predisposes a person to cerebral ischemia. In future routine screening of high risk patients is necessary to prevent the occurrence of stroke.
Abbreviation
CIMT- Carotid Intima Media Thickness
PSV- Peak Systolic Velocity
EDV-End Diastolic Velocity
CCA-Common Carotid Artery
ICA-Internal Carotid Artery
ECA-External Carotid Artery
MCA-Middle Carotid Artery
ACA- Anterior Cerebral Artery
PCA-Posterior Cerebral Artery
PICA-Posterior Inferior Cerebral Artery
AICA-Anterior Inferior Cerebral Artery
NASCET-North American Symptomatic
Carotid Endarterectomy Trial
ECST-European Carotid Surgery Trialists.
MCA-middle carotid artery, ACA-anterior cerebral artery, PCA-posterior cerebral artery, PICA-posterior inferior cerebral artery, AICA-anterior inferior cerebral artery