Introduction
Investigators over years have been fascinated by dermatoglyphic patterns which has led to the development of dermatoglyphics as a science with numerous applications in various fields other than being the best and most widely used method for personal identification.
Aim
To assess the correlation between dermatoglyphic patterns and sagittal skeletal discrepancies.
Materials and Methods
A total of 180 patients, aged 18-40 years, were selected from those who attended the outpatient clinic of the Deparment of Orthodontics and Dentofacial Orthopedics, Mar Baselios Dental College, Kothamangalam, Kerala, India. The fingerprints of both hands were taken by ink and stamp method after proper hand washing. The patterns of arches, loops and whorls in fingerprints were assessed. The total ridge count was also evaluated. Data was also sent to the fingerprint experts for expert evaluation. The sagittal jaw relation was determined from the patient’s lateral cephalogram. The collected data was then statistically analyzed using Chi-square tests, ANOVA and Post-hoc tests and a Multinomial regression prediction was also done.
Results
A significant association was observed between the dermatoglyphic pattern exhibited by eight fingers and the sagittal skeletal discrepancies (p<0.05). An increased distribution of whorl pattern was observed in the skeletal Class II with maxillary excess group and skeletal Class II with mandibular deficiency group while an increased distribution of loop pattern was seen in the skeletal Class III with mandibular excess group and skeletal Class III with maxillary deficiency group. Higher mean of total ridge count was also seen in the groups of skeletal Class II with maxillary excess and skeletal Class II with mandibular deficiency. Multinomial regression predicting skeletal pattern with respect to the fingerprint pattern showed that the left thumb impression fits the best model for predicting the skeletal pattern.
Conclusion
There was a significant association between dermatoglyphic patterns and sagittal skeletal discrepancies. Dermatoglyphics could serve as a cost effective screening tool of these craniofacial problems.
Introduction
Valleys and ridges together form unique patterns on the skin of palms, fingers, soles and toes. The term ‘dermatoglyphics’, which is the study of dermal ridge configurations on the palmar and plantar surfaces of the hands and feet, was coined by Harold Cummins and Midlo in 1926 [1,2]. Investigators over years have been fascinated by dermatoglyphic patterns which have led to the development of dermatoglyphics as a science with numerous applications in various fields like biology, medicine, genetics and evolution. It is the best and most widely used method for personal identification [3]. Dermatoglyphic analysis has proven to be a useful preliminary diagnostic investigation aid in conditions with a suspected genetic base [4,5].
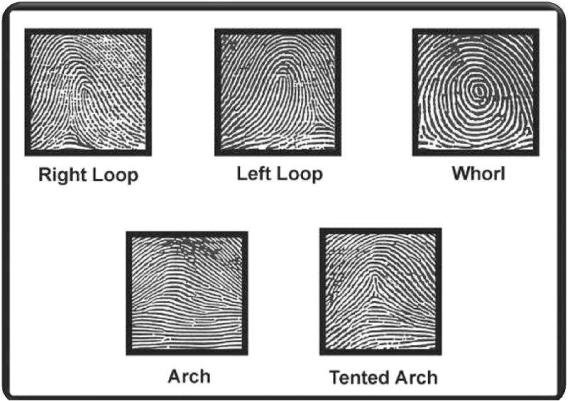
Fingerprint analysis is based on the uniqueness of the fingerprints which is determined by the minute changes in the local foetal environment and the fact that they do not change during a person’s life. Presence of pores on the surface of the ridges of fingers results in accumulation of perspiration on the fingertips which remains on the surface of the object a person touches, leaving prints [6,7]. Finger prints are usually categorized into three basic groups namely arches (60-65%), loops (30-35%) and whorls (5%) [3,8] [Table/Fig-1]. A person may have the same pattern on all ten fingers but various patterns often occur on different digits [3,9–11].
Types of fingerprint patterns.
In medical dermatoglyphics, it has been shown that there is an association between fingerprint patterns and various conditions like diabetes mellitus, hypertension [12], psychosis [13], breast cancer [14], alcohol embryopathy [15], epilepsy [16], congenital heart diseases [17] and many other conditions [18]. In the field of dentistry, irregular fingerprints have been observed among patients with periodontitis [19], dental caries [20,21], certain types of congenital anomalies like cleft lip and palate [22,23] and recently, dermatoglyphics has been related to malocclusion [24–26] and other developmental disturbances of the orofacial structures [27–29].
Malocclusion is a common oral condition affecting facial aesthetics which may involve irregular alignment of teeth, faulty positioning of the jaws or a combination of both [30]. The development of the dentition and the palate occur during the same period as the development of dermal patterns which is around the sixth-seventh week of intrauterine life [11,23,31,32]. Hereditary and environmental factors causing changes in the lip, alveolus and palate, may also cause abnormalities in the appearance of finger and palm prints [22,23]. Recent recognition of correlation between dermatoglyphics and oral clefts, periodontitis, and dental caries has drawn our attention to correlate dermatoglyphics and malocclusion such as sagittal skeletal discrepancies. Both genetic and environmental factors can affect the craniofacial development creating a multifactorial aetiology for sagittal skeletal discrepancies. It is assumed that the genetic message contained in the genome during this period may reflect in the dermatoglyphic patterns [33,34]. Dermatoglyphics could thus prove to be an effective screening tool and help to strengthen the diagnosis. It could also help in the early interceptive treatment of some sagittal skeletal discrepancies.
The aim of this study was to assess the correlation between dermatoglyphic patterns and sagittal skeletal discrepancies by comparing and evaluating the palmar digital dermatoglyphic patterns in sagittal skeletal discrepancies: Ideal skeletal Class I, skeletal Class I with bimaxillary protrusion, skeletal Class II with maxillary excess, skeletal Class II with mandibular deficiency, skeletal Class III with mandibular excess and skeletal Class III with maxillary deficiency.
Materials and Methods
The present cross-sectional study was conducted on 180 subjects (90 males, 90 females), aged 18-40 years randomly selected from the outpatient clinic of Department of Orthodontics and Dentofacial Orthopaedics, Mar Baselios Dental College, Kothamangalam from 20th April 2013 to 20th April 2014. The sample size was calculated by the formula
= [13.62]2 =185.55=186 where n is the sample size, a 95% degree confidence corresponds to α=0.05, z the standard normal deviation, E the margin of error E=1 and standard deviation=6.95. To bring about uniformity during categorization, the total sample was adjusted to 180. The total sample of 180 subjects was categorized into six groups of 30 each:
Ideal skeletal Class I;
Skeletal Class I with bimaxillary protrusion;
Skeletal Class II with maxillary excess;
Skeletal Class II with mandibular deficiency;
Skeletal Class III with mandibular excess;
Skeletal Class III with maxillary deficiency.
Only systemically healthy subjects of the age 18-40 years, who consented to participate in the study, and had not undergone any previous orthodontic treatment or oro maxillofacial surgery, were included. Patients with developmental anomalies, any systemic disease affecting bone and general health, children and pregnant women, mentally retarded patients, patients with both maxillary and mandibular excess and patients who did not give an informed consent were excluded from the study.
The study protocol was approved by the Institutional Ethics Committee of Mar Baselios Dental College, Kothamangalam, Kerala, India (IEC/31/2012/MBDC). The procedure was explained to the patients and a written informed consent was obtained from them with due consideration to ethical issues and confidentiality of fingerprint records.
The sagittal jaw relation was determined from the patient’s lateral cephalogram with assessment of the following parameters: SNA, SNB, ANB, Wits appraisal, condylion to Point A, condylion to gnathion, angle of convexity and facial angle (Steiner’s, Down’s, Mcnamara and COGS analyses and Wits Apraisal). Points A and B were regarded as the anterior limits of the apical bases of maxilla and mandible and cephalometric norms of South Indian population were taken into consideration [Table/Fig-2]. The patients were thus categorized into six groups according to the skeletal relationship of maxilla and mandible.
Categorization of sagittal skeletal discrepancies.
| Category | Parameters |
|---|
| SNA | SNB | ANB | Wits Appraisal | Condylion to point A | Condylion to Gnathion | N to ANS | ANS to Gn | Angle of Convexity | Facial Angle |
|---|
| Ideal skeletal class I | 820 | 790 | 2-40 | 0 to -1mm | 92-96 mm | 121-126 mm | 50-53mm | 66mm | 2-40 | 820 |
| Skeletal Class I with bimaxillary protrusion | 82-840 | 79-800 | 40 | 0 to 1mm | 92-98mm | 121-126mm | 48-50mm | 67-69mm | 7-100 | 82-860 |
| Skeletal Class II with maxillary excess | >840 | 790 | >40 | >4mm | 98-103mm | 120-124 mm | >54mm | 64mm | >100 | 80-820 |
| Skeletal Class II with mandibular deficiency | 82-840 | <790 | >40 | 3-4mm | 90-92mm | <118mm | 50-53mm | < 64 mm | >100 | <820 |
| Skeletal Class III with mandibular excess | 82-830 | >800 | < -40 | -4mm | 90-92mm | >135mm | 50-54mm | > 69 mm | -6 to -80 | >950 |
| Skeletal Class III with maxillary deficiency | <800 | 80-810 | 1 to -40 | -2.5mm to -4mm | 78-90mm | 124mm | 48-53mm | 67-69mm | -2 to - 70 | 95-960 |
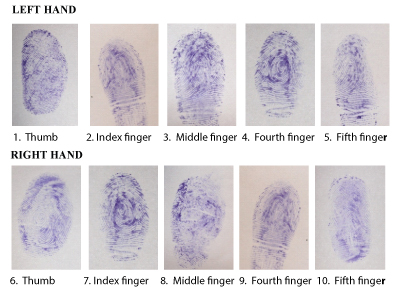
The subjects were asked to clean their hands with soap and water and wipe with ethyl alcohol to remove the sweat, oil and dirt from the skin surface. The finger prints were recorded using the ink stamp method. The dried distal phalanges of both hands were rolled on an ink pad and stamped on bond paper which was fixed in place with adhesive tape [Table/Fig-3]. To avoid duplication of fingerprints, the fingers were numbered from 1-5 from left thumb to little finger and from 6-10 for right thumb to little finger [Table/Fig-4]. All the fingerprints taken, were verified for perfection. In order to protect this sensitive data, a double coding system was used i.e., the groups were coded and the data from each patient were also coded and was stored securely. The prints obtained were assessed for the frequency of arches, loops and whorls. The total ridge count was also evaluated. Interpretation of patterns was assessed according to the method by Cummins and Midlo [1]. Data was also sent to the fingerprint experts for expert evaluation.
Method of taking finger prints.

Types of fingerprint patterns.
Statistical Analysis
Data pertaining to the fingerprints were obtained and entered into an Excel spread sheet and imported to statistical software SPSS version 16.0 for descriptive and Chi-square analysis. The percentage frequency of arches, loops and whorls were assessed in the six groups and noted separately for the ten fingers of the right and left hands. The values obtained were statistically analysed using Chi-square tests, ANOVA and Post-hoc tests and a Multinomial regression prediction was also done. The level of significance was set at 5% and 95% confidence interval was taken.
Results
A total sample of 180 subjects was categorized into six groups with 30 subjects in each group based on the skeletal relationship of maxilla and mandible. The dermatoglyphic patterns for the ten fingers of these 180 subjects were recorded using ink stamp method. The fingerprints were observed and identified into arches, loops and whorls. These results were entered and calculated for each subject (N=180). The frequency distribution of the different dermatoglyphic patterns on the right and left hands in the 180 subjects categorized into six groups were assessed.
Loop and whorl patterns were more frequent than the arch pattern which was less than 5%. There was an increased distribution of whorl pattern in the skeletal Class II with maxillary excess group and skeletal Class II with mandibular deficiency group while there was an increased distribution of loop pattern in the skeletal Class III with mandibular excess group and skeletal Class III with maxillary deficiency group. Out of the ten fingers of each subject analysed, a significant association (p-value < 0.05) between the dermatoglyphic patterns was exhibited by eight fingers (left thumb, left index finger, left middle finger, left fourth finger, left fifth finger, right thumb, right index finger and right middle finger) and the sagittal skeletal discrepancies. It was seen that when the Chi-square test was done, the expected frequency was lower than what was expected within cells, so the Fisher’s exact test was utilized to rule out the independency of these dermatoglyphic patterns and the sagittal discrepancies based on the statistical rule that when the total sample (N) is greater than 40, the Chi-square test should be used with Yates’ correction [Table/Fig-5].
Distribution of dermatoglyphic patterns within the six groups of sagitttal skeletal discrepancies for the 10 fingers (N = 180) using:
| Dermatoglyphic Patterns | Ideal Skeletal Class I (n=30) | Skeletal Class I with Bimaxillary Protrusion (n=30) | Skeletal Class II with Maxillary excess (n=30) | Skeletal Class II with Mandibular deficiency (n=30) | Skeletal Class III with Mandibular excess (n=30) | Skeletal Class III with Maxillary deficiency (n=30) | Total (N=180) | % | (i), (ii), (iii)(Significance Level) |
|---|
| Left Thumb | Arch | 1 (3.3%) | 0 (0.0%) | 0 (0.0%) | 3 (10%) | 0 (0.0%) | 0 (0.0%) | 4 | 2.2 | 35.51731.9880.314(<0.001)* |
| Loop | 19 (63.3%) | 18 (60%) | 12 (40%) | 13(43.3%) | 28(93.3%) | 23(76.7% | 113 | 62.8 |
| Whorl | 10 (33.3%) | 12(40%) | 18(60%) | 14 (46.7%) | 2(6.7%) | 7(23.3%) | 63 | 35.0 |
| Left Index finger | Arch | 0(0.0%) | 0(0.0%) | 0(0.0%) | 7(23.3%) | 4(13.3%) | 12(40%) | 23 | 12.8 | 59.38355.3620.409(<0.001)* |
| Loop | 21(70%) | 25(83.3%) | 12(40%) | 7(23.3%) | 18(60%) | 11(36.7% | 94 | 52.2 |
| Whorl | 9(30%) | 5(16.7%) | 18(60%) | 16(53.3%) | 8(26.7%) | 7(23.3%) | 63 | 35.0 |
| Left middle finger | Arch | 1 (3.3%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 6(20%) | 7 | 3.9 | 30.01918.1980.289(<0.001)* |
| Loop | 20(66.7%) | 24(80%) | 19(63.3% | 24(80%) | 19(63.3%) | 17(56.7% | 123 | 68.3 |
| Whorl | 9(30%) | 6(20%) | 11(36.7% | 6(20%) | 11(36.7%) | 7(23.3%) | 50 | 27.8 |
| Left fourth finger | Arch | 0(0.0%) | 0(0.0%) | 0(0.0%) | 2(6.7%) | 0(0.0%) | 3(10%) | 5 | 2.8 | 21.09817.7990.242(0.019) * |
| Loop | 14(46.7%) | 12(40%) | 14(46.7% | 7(23.3%) | 11(36.7%) | 18(60%) | 76 | 42.2 |
| Whorl | 16(53.3%) | 18(60%) | 16(53.3% | 21(70%) | 19(63.3%) | 9(30%) | 99 | 55.0 |
| Left fifth finger | Arch | 2(6.7%) | 0(0.0%) | 0(0.0%) | 2(6.7%) | 0(0.0%) | 0(0.0%) | 4 | 2.2 | 21.42718.2520.244(.012) * |
| Loop | 26(86.7%) | 24(80%) | 25(83.3% | 17(56.7%) | 28(93.3%) | 23(76.7% | 143 | 79.4 |
| Whorl | 2(6.7%) | 6(20%) | 5(16.7%) | 11(36.7%) | 2(6.7%) | 7(23.3%) | 33 | 18.3 |
| Right Thumb | Arch | 0(0.0%) | 0(0.0%) | 0(0.0%) | 3(10%) | 6(20%) | 0(0.0%) | 9 | 5.0 | 27.88121.3880.278(0.006) * |
| Loop | 16(53.3%) | 13(43.3%) | 18(60%) | 14(46.7%) | 18(60%) | 15(50%) | 94 | 52.2 |
| Whorl | 14(46.7%) | 17(56.7%) | 12(40%) | 13(43.3%) | 6(20%) | 15(50%) | 77 | 42.8 |
| Right Index finger | Arch | 0(0.0%) | 2(6.7%) | 0(0.0%) | 3(10%) | 6(20%) | 6(20%) | 17 | 9.4 | 36.83836.5060.320(<0.001)* |
| Loop | 15(50%) | 18(60%) | 3(10%) | 15(50%) | 11(36.7%) | 12(40%) | 74 | 41.1 |
| Whorl | 15(50%) | 10(33.3%) | 27(90%) | 12(40%) | 13(43.3%) | 12(40%) | 89 | 49.4 |
| Right middle finger | Arch | 4(13.3%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 3(10%) | 7 | 3.9 | 27.84723.3930.278(0.002)* |
| Loop | 14(46.7%) | 27(90%) | 21(70%) | 26(86.7%) | 20(66.7%) | 20(66.7% | 128 | 71.1 |
| Whorl | 12(40%) | 3(10%) | 9(30%) | 4(13.3%) | 10(33.3%) | 7(23.3%) | 45 | 25.0 |
| Right fourth finger | Arch | 2(6.7%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 3(10%) | 5 | 2.8 | 16.54012.7560.214 (0.138) |
| Loop | 10(33.3%) | 12(40%) | 9(30%) | 8(26.7%) | 14(46.7%) | 14(46.7% | 67 | 37.2 |
| Whorl | 18(60%) | 18(60%) | 21(70%) | 22(73.3%) | 16(53.3%) | 13(43.3% | 108 | 60.0 |
| Right fifth finger | Arch | 0(0.0%) | 0(0.0%) | 0(0.0%) | 2(6.7%) | 0(0.0%) | 0(0.0%) | 2 | 1.1 | 19.14814.9170.231(0.053) |
| Loop | 26(86.7%) | 22(73.3%) | 22(73.3% | 20(66.7%) | 28(93.3%) | 20(66.7% | 138 | 76.7 |
| Whorl | 4(13.3%) | 8(26.7%) | 8(26.7%) | 8(26.7%) | 2(6.7%) | 10(33.3% | 40 | 22.2 |
Pearson Chi-square test, Fisher test and Cramer test. * shows p-value significant at 0.05. (i) is the Chi-square value, (ii) is the Fisher exact value and (iii) is the Cramer’s V value.
The mean total ridge count of the dermatoglyphic patterns was assessed for the ten fingers of the right and left hands in the six groups of sagittal skeletal discrepancies. The mean of total ridge count was higher in the groups of skeletal Class II with maxillary excess and skeletal Class II with mandibular deficiency [Table/Fig-6]. As the dependent variables were multiple a multinomial regression prediction was done. This showed that the ridge count could be considered for predicting skeletal pattern [Table/Fig-7]. Multinomial regression predicting skeletal pattern with respect to the fingerprint pattern showed that the left thumb impression fits the best model for predicting the skeletal pattern [Table/Fig-8].
ANOVA (F statistic) test for mean of ridge count between the six groups of skeletal sagittal discrepancies.
| Groups | Mean | Std. Deviation | F statistic | p-value |
|---|
| Ideal Skeletal Class I (n=30) | 85.9333 | 21.82838 | 13.441 | <0.001 |
| Skeletal Class I with Bimaxillary Protrusion (n=30) | 92.4333 | 11.43402 |
| Skeletal Class II with Maxillary Excess (n=30) | 111.6667 | 9.11359 |
| Skeletal Class II with Mandibular Deficiency (n=30) | 102.1667 | 23.89933 |
| Skeletal Class III with Mandibular Excess (n=30) | 78.1667 | 19.48843 |
| Skeletal Class III with Maxillary Deficiency (n=30) | 77.9 | 28.45002 |
| Total | 91.3778 | 23.46021 | |
Multinomial regression predicting skeletal pattern with respect to the ridge count.
| Parameter Estimates |
|---|
| Groupsa | Interceptb | Sig. (p-value) | Odds ratio | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Ideal Skeletal Class I | Intercept | -1.337 | 0.183 | | | |
| ridge count | 0.016 | 0.167 | 1.016 | .993 | 1.040 |
| Skeletal Class I with bimaxillary protrusion | Intercept | -2.616 | 0.017 | | | |
| ridge count | 0.031 | 0.013 | 1.031 | 1.006 | 1.056 |
| Skeletal Class II with maxillary excess | Intercept | -9.850 | <0.001 | | | |
| ridge count | 0.100 | <0.001 | 1.106 | 1.064 | 1.149 |
| Skeletal Class II with mandibular deficiency | Intercept | -5.239 | <0.001 | | | |
| ridge count | 0.058 | <0.001 | 1.059 | 1.030 | 1.089 |
| Skeletal Class III with mandibular excess | Intercept | -0.041 | 0.965 | | | |
| ridge count | 0.001 | 0.963 | 1.001 | 0.978 | 1.023 |
a. The reference category is: Skeletal Class III with maxillary deficiency
b. A statistical term used for the multinomial regression
Multinomial regression predicting skeletal pattern with respect to the finger print pattern.
| Parameter Estimates |
|---|
| Groupsa | Interceptb | Sig. (p-value) | Odds ratio | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Ideal Skeletal Class I | Intercept | 0.452 | 0.350 | | | |
| (Left thumb print=2.00) | -0.643 | 0.263 | 0.526 | 0.171 | 1.620 |
| (Left thumb print=3.00) | 0b | - | - | - | - |
| Skeletal Class I with bimaxillary protrusion | Intercept | 0.539 | 0.257 | | | |
| (Left thumb print=2.00) | -0.784 | 0.169 | 0.457 | 0.149 | 1.396 |
| (Left thumb print=3.00) | 0b | - | - | - | - |
| Skeletal Class II with maxillary excess | Intercept | 0.944 | 0.034 | | | |
| (Left thumb print=2.00) | -1.595 | 0.005 | 0.203 | 0.066 | 0.620 |
| (Left thumb print=3.00) | 0b | - | - | - | - |
| Skeletal Class II with mandibular deficiency | Intercept | 0.887 | 0.048 | | | |
| (Left thumb print=2.00) | -1.458 | 0.010 | 0.233 | 0.077 | 0.708 |
| (Left thumb print=3.00) | 0b | . | - | - | - |
| Skeletal Class III with mandibular excess | Intercept | -1.253 | 0.118 | | | |
| (Left thumb print=2.00) | 1.449 | 0.088 | 4.261 | 0.806 | 22.532 |
| (Left thumb print=3.00) | 0b | - | - | - | - |
a. The reference category is: Skeletal Class III with maxillary deficiency. b. This parameter is set to zero because it is redundant.
Discussion
Dermatoglyphic patterns are genetically determined and their inheritance is considered to follow a classic polygenic model which has proved useful to study many genetic disorders [5]. Dermatoglyphic investigation being convenient, cost effective and non invasive, had been applied in many fields and dentistry has been no where behind in the race of investigation with several investigators utilizing this useful diagnostic tool to unveil genetic factors related to many oral diseases [34]. An early diagnosis and correction of deviated growth patterns of jaws through early interceptive orthodontic treatment may help preventing some of the future orthognathic surgeries [35].
It has been seen that though a person may have the same pattern on all ten fingers, various patterns often can occur on different digits. Loops were however the most common pattern on the fingertips. Whorls were most likely to be found on the thumb and the ring finger while radial loops and arches were most common on the index finger. On the little finger, the most frequent pattern was an ulnar loop [3,7,9–11].
In our study, an increased distribution of whorl pattern in the skeletal Class II with maxillary excess group and skeletal Class II with mandibular deficiency group while there was an increased distribution of loop pattern in the skeletal Class III with mandibular excess group and skeletal Class III with maxillary deficiency group. The mean of the total ridge count of the dermatoglyphic patterns were also assessed for the ten fingers of the right and left hands in the six groups of sagittal skeletal discrepancies. The ANOVA and Post-hoc tests showed that the percentage of total ridge count was also higher in skeletal Class II with maxillary excess and skeletal Class II with mandibular deficiency. Multinomial regression predicting skeletal pattern with respect to ridge count showed that the ridge count could be considered for predicting skeletal pattern. On the other hand the multinomial regression predicting skeletal pattern with respect to the fingerprint pattern showed that the left thumb impression fits the best model for predicting the skeletal pattern.
Previous studies have reported varying results. In a recent study comparing the dermatoglyphic characteristics of different malocclusions, some slight differences in dermatoglyphic peculiarities especially between Class I and Class III patients in terms of a-b ridge count were seen, while most other dermatoglyphic characteristics failed to indicate significant differences [35]. In another study on the association of dermatoglyphic features with different classes of malocclusion, although no fingerprint pattern was found to be specific for a particular class of malocclusion, in subjects with Class II malocclusion increased frequency of whorl pattern especially on the thumb was observed, while subjects with Class III malocclusion showed an increased frequency of plain arches [34]. Results of a previous study using dermatoglyphics to predict and compare Class I, Class II Div 1, Div 2 and Class III malocclusions revealed that the craniofacial Class II Div 1, Class II Div 2 patterns were associated with an increased frequency of arches and ulnar loops and a decreased frequency of whorls [24]. However, in one dermatoglyphic study of normal occlusion and malocclusion, as compared to normal occlusion, Class I and Class III malocclusions were associated with an increased frequency of whorls but both Class I and Class II Div 1 malocclusions were associated with an increased frequency of radial loops and arches [25]. Another comparative study of dermatoglyphics in individuals with normal occlusion and malocclusions indicated a decreased frequency of radial loops, twinned loops and central pocket loops associated with Class III malocclusions. No significant increase in arches in Class III malocclusions was found except on the middle finger.
In another study comparing the dermatoglyphic patterns with normal, hypodivergent and hyperdivergent subjects, an increased presence of loop pattern followed by whorls and arches was observed in hypodivergent growth pattern. However, an increased presence of whorl pattern followed by loops and arches was seen in the hyperdivergent growth pattern. Nearly the same pattern of distribution of loops and whorls was observed in subjects with average growth pattern. These average growth subjects also showed an increased presence of arch pattern than hypodivergent and hyperdivergent growth pattern [36]. There was a significant increase in whorls in Class II Div 1 cases. The sensitivity values were found to be higher and more reliable in predicting Class III malocclusions based on the frequency of arches, than those of Class II Div 1 and Div 2 malocclusions [37]. Another study assessing the relationship between fingerprints and malocclusion found that though there was no overall statistical association observed between fingerprint patterns and malocclusion, a significant statistical association was seen with whorl patterns and Class I and Class II malocclusion [26]. A dermatoglyphic evaluation of twenty five North Indian males with true mandibular prognathism revealed an association with an increase in arches and ulnar loops at the expense of whorls on all digits except the index finger with the craniofacial skeletal Class III pattern. There was an increased frequency of whorls and radial loops and carpel loops on the interdigital area of palms [28]. The disparity in results could be due to variations in sample size, differences in protocol for recording fingerprint patterns, ethnic and racial variations etc.
According to the current study, dermatoglyphics can be used in clinical situations to add on to the diagnostic impression of the sagittal skeletal relationships of maxilla and mandible. An example in this context would be the association of an increased whorl pattern with skeletal Class II with maxillary excess and skeletal Class II with mandibular deficiency. This dermatoglyphic information not only adds to strengthen the diagnosis, but a prompt diagnosis and efficient treatment planning could be used in utilizing the catch up growth of the mandible. This is true for early interception in a young child presenting with skeletal Class II with mandibular deficiency. Thus, in the long run the duration and complexity of the next phase of comprehensive treatment would be greatly reduced. Multicentre studies are thus highly recommended to deliver a generalized impression especially in utilizing the potential of dermatoglyphics as a screening tool which will eventually lead to early and timely orthodontic interception.
The present study had some limitations. This was a hospital based study as the subjects recruited were those who visited the hospital for treatment purposes. In order to establish an association with dermatoglyphic patterns and sagittal discrepancies, observations should be made on a larger sample which is representative of entire population. The recording of fingerprints was much dependent on the pliable nature of application of fingerprint pressure which could lead to incomplete fingerprints. The ink stamp method has its limitations with many a times recording of smudged fingerprints. Digitalized fingerprint sensors could be useful to overcome this limitation. Galton’s classification of dermatoglyphic patterns into arches, loops and whorls was used in the current study, however, composite fingerprint patterns were noted in a few patients and these patterns were recorded according to the majority of the patterns exhibited by ten fingers. The presence of scars, warts and deterioration of ridge minutiae patterns in people who did a lot of manual work did bring about difficulty in identification of fingerprints and thus errors in the fingerprint recognition system. The training in fingerprint recognition is mostly for good quality fingerprints and not for worn and damaged fingerprint patterns.
Conclusion
There is a significant association between dermatoglyphic patterns and sagittal skeletal discrepancies. Dermatoglyphics could be used as a cost effective tool for the preliminary investigation of sagittal skeletal discrepancies and could also strengthen the diagnostic impression of these craniofacial problems. Identifying these problems at an early age by the utilization of this dermatoglyphic information could eventually lead to formulate an efficient treatment plan.
Pearson Chi-square test, Fisher test and Cramer test. * shows p-value significant at 0.05. (i) is the Chi-square value, (ii) is the Fisher exact value and (iii) is the Cramer’s V value.
a. The reference category is: Skeletal Class III with maxillary deficiency
b. A statistical term used for the multinomial regression
a. The reference category is: Skeletal Class III with maxillary deficiency. b. This parameter is set to zero because it is redundant.
[1]. Cummins H, Midlo C, Finger prints, palms and solesAn introduction to Dermatoglyphics 1961 New YorkDover Publications, Inc [Google Scholar]
[2]. Mulvihill JJ, Smith DW, The genesis of dermatoglyphicsJournal of Pediatrics 1969 75(4):579-89. [Google Scholar]
[3]. Pratibha R, Abhilash PR, Sherlin HJ, Anuja N, Premkumar P, Chandrasekar T, Conventional dermatoglyphics – revived concept: A reviewInternational Journal of Pharma and Bio Sciences 2011 2(3):446-58. [Google Scholar]
[4]. Uchida IA, Soltan HC, Evaluation of dermatoglyphics in medical geneticsPediatric Clinics of North America 1963 10:409-21. [Google Scholar]
[5]. Holt SB, Quantitative genetics of finger print patternsBritish Medical Bulletin 1961b 17:247 [Google Scholar]
[6]. Lichanska A. Fingerprint Analysis. Available from http://www.faqs.org/espionage/Ep-Fo/Fingerprint-Analysis.html [Google Scholar]
[7]. Maltoni D, Maio D, Jain AK, Prabhakar S, Handbook of fingerprint recognition 2003 Springer - Verlag [Google Scholar]
[8]. Galton F, Finger Prints 1892 LondonMacmillan [Google Scholar]
[9]. Lakshmi V, Dermatoglyphics and orthodontics – A reviewAnnals and Essences of Dentistry 2013 5(4):30-33. [Google Scholar]
[10]. Soni A, Singh SK, Gupta A, Implications of dermatolyphics in dentistryJournal of Dentofacial Sciences 2013 2(2):27-30. [Google Scholar]
[11]. Verbov J, Clinical significance and genetics of epidermal ridges – A review of dermatoglyphicsThe Journal of Investigative Dermatology 1970 54(4):261-71. [Google Scholar]
[12]. Igbigbi PS, Msamati BC, Ng’ambi TM, Plantar and digital dermatoglyphic patterns in Malawian patients with diabetes mellitus, hypertension and diabetes mellitus with hypertensionInt J Diabetes metabolism 2001 9:24-31. [Google Scholar]
[13]. Rosa A, Fañanas L, Bracha HS, Torrey EF, van Os J, Congenital dermatoglyphic malformations and psychosis: A twin studyAm J Psychiatry 2000 157:1511-13. [Google Scholar]
[14]. Chintamani Khandelwal R, Mittal A, Qualitative and quantitative dermatoglyphic traits in patients with breast cancer: A prospective clinical studyBMC Cancer 2007 7:44 [Google Scholar]
[15]. Quazi QH, Masokawa A, McGann B, Woods J, Dermatoglyphic abnormalities in the fetal alcohol syndromeTeratology 1980 21:157-60. [Google Scholar]
[16]. Balgir RS, Dermatoglyphic studies in epilepsy, juvenile delinquency and criminality and mental retardation: A reviewActa Anthropogenet 1986 10:15-25. [Google Scholar]
[17]. Alter M, Schulenberg R, Dermatoglyphics in congenital heart diseaseCirculation 1970 41:49-54. [Google Scholar]
[18]. Schaumann B, Alter M, Dermatoglyphics in medical disorders 1976 New YorkSpringer – Verlag [Google Scholar]
[19]. Atasu M, Kuru B, Firatli E, Meriç H, Dermatoglyphic findings in periodontal diseasesInt J Anthropol 2005 20:63-75. [Google Scholar]
[20]. Sharma A, Somani R, Dermatoglyphic interpretation of dental caries and its correlation to salivary bacteria interactions: An in vivo studyJ Indian Soc Pedod Prev Dent 2009 27:17-21. [Google Scholar]
[21]. Sengupta AB, Bazmi BA, Sarkar S, Kar S, Ghosh C, Mubtasum H, A cross sectional study of dermatoglyphics and dental caries in Bengalee childrenJ Indian Soc Pedod Prev Dent 2013 31(4):245-48. [Google Scholar]
[22]. Balgir RS, Dermatoglyphic features in congenital cleft lip and cleft palate anomaliesJ Indian MA 1986 84(12):369-72. [Google Scholar]
[23]. Mathew L, Hegde AM, Rai K, Dermatoglyphic peculiarities in children with oral cleftsJ Indian Soc Pedod Prev Dent 2005 23:179-82. [Google Scholar]
[24]. Reddy S, Prabhakar AR, Reddy VVS, A dermatoglyphic predictive and comparative study of class I, class II, div.1, div. 2 and class III malocclusionsJ Indian Soc Pedod Prev Dent 1997 15:13-19. [Google Scholar]
[25]. Trehan M, Kapoor DN, Tandon P, Sharma VP, Dermatoglyphic study of normal occlusion and malocclusionJ Ind Orthod Soc 2001 34:114-25. [Google Scholar]
[26]. Tikare S, Rajesh G, Prasad KW, Thippeswamy V, Javali SB, Dermatoglyphics – A marker for malocclusion?Int Dent Journ 2010 60(4):300-04. [Google Scholar]
[27]. Sharma VP, Gupta DS, Kharbanda OP, Dermatoglyphic evaluation of retrognathismJ Indian Dent Assoc 1980 52:111-14. [Google Scholar]
[28]. Kharbanda OP, Sharma V, Gupta DS, Dermatoglyphic evaluation of mandibular prognathismJ Indian Dent Assoc 1982 54:179-86. [Google Scholar]
[29]. Akyuz S, Hemifacial microsomia. Oral, clinical, genetic and dermatoglyphic findingsJ Clin Pediatr Dent 1998 23:63-68. [Google Scholar]
[30]. Bhasin MT, Bhasin P, Singh A, Bhatia N, Shewale AH, Gambhir N, Dermatoglyphics and malocclusion – A forensic linkBritish Biotechnology Journal 2016 13(1):1-12. [Google Scholar]
[31]. Penrose LS, O’Hara PT, The development of epidermal ridgesJ Med Genetics 1973 10:201-08. [Google Scholar]
[32]. Kumbnani HK, Dermatoglyphics: A reviewAnthropologist Special Volume 2007 3:285-95. [Google Scholar]
[33]. Mossey PA, The heritability of malocclusion: Part 2. The influence of genetics in malocclusionBritish Journal of Orthodontics 1999 26:195-203. [Google Scholar]
[34]. Jindal G, Pandey RK, Gupta S, Sandhu M, A comparative evaluation of dermatoglyphics in different classes of malocclusionThe Saudi Dental Journal 2015 27:88-92. [Google Scholar]
[35]. Eslami N, Jahanbin A, Ezzati A, Banihashemi E, Kianifar H, Can Dermatoglyphics be used as a marker for predicting Future MalocclusionsElectronic Physician 2016 8(2):1927-32. [Google Scholar]
[36]. Thakkar DP, Joshipura AJ, A dermatoglyphic comparative study of hypodivergent, hyperdivergent and normal subjectsJournal of Pearldent 2012 3(4):20-24. [Google Scholar]
[37]. Reddy BRM, Sankar G, Roy ET, Govula S, A comparative study of dermatoglyphics in individuals with normal occlusions and malocclusionsJ Clin Diagn Res 2013 7(12):3060-65. [Google Scholar]