Dental caries is a global oral health problem with distinctive variations in its distribution. It continues to be the most common infectious disease in the children. It is a multifactorial disease with Streptococcus mutans being the major contributor in the development of dental caries. The bacterial cells of S.mutans colonize the tooth and forms a biofilm called as dental plaque [1].
Dental plaque is a biofilm formed on the surfaces of the tooth and restorations present in the oral cavity. Dental plaque is considered to be one of the aetiological factors in causation of dental caries, gingivitis and periodontitis [2]. Efficient plaque control is essential for maintaining good gingival and periodontal health, prevention of dental caries and to preserve the oral health [3,4].
Various chemical and mechanical methods are available commercially for the removal of plaque. Tooth brushing is found to be the most commonly used effective and safest method for plaque removal [5]. Manual tooth brush remains the primary method of maintaining good oral hygiene in majority of the population [6]. Powered tooth brush was introduced in 1960 and 62% of the people are using powered tooth brush on daily basis [7]. Effective tooth brushing requires certain degree of manual dexterity, which increases only with age. A recent innovation for plaque removal is the discovery of chewable tooth brush (Rolly mini tooth brush), comprised of fluoride and xylitol [8]. Fluoride at low concentration is bacteriostatic and at high concentration it is bactericidal [9]. Xylitol, a non-sugar sweetener used in foods is non-cariogenic and has cariostatic effect.
There is only limited evidence in the literature evaluating the effectiveness of chewable tooth brush in children. Bezgin T et al., investigated the effectiveness of chewable brush in children between 10-12 years of age and concluded that chewable brush is as effective as manual brushing [2]. Myoken Y et al., studied the effectiveness of the chewable brush in elderly population and stated that chewable brush is effective in plaque removal [10]. There is no evidence showing the association between chewable tooth brush and the levels of Streptococcus mutans in the saliva.
Therefore, the aim of this study was to evaluate the effectiveness of chewable brush in children in relation to efficient plaque removal and reduction of S.mutans levels in saliva.
Materials and Methods
The present prospective clinical study was carried out after the approval was obtained from the Institutional Ethical Committee of Saveetha Dental College (STP/SDMDS2015PED42)
Participants: All the children of age group six-nine years in an institution (Vriksham foundation, Chennai, Tamil Nadu, India) were screened and were included in the study. The study was explained to the associated member of the foundation and the participant’s details, past medical history including any recent antibiotic intake were collected from the records maintained in the institution.
Inclusion criteria: Subjects who were willing to participate, free from any systemic diseases with their first molars erupted were included in the study. The informed consent of the participants was obtained from the head of the institution as he was the guardian for the children present in the foundation.
Exclusion criteria: Children with previous medical history, with the history of intake of antibiotics for the past one month and uncooperative children were excluded from the study.
Sample size calculation: Sample size was calculated from a previous study [2] with a power of 0.95, alpha error 0.05 and arrived to a sample of 10 using G Power version 3.1. (Department of psychology, University Manheim, Germany).
Dental examination: Oral examination was done using mouth mirror and probe. Prior to the use of chewable brushes, the baseline indices were recorded at the end of seventh day of manual brushing. The indices were recorded again on the seventh day after the use of chewable brushes. The same group of children served as both control and study group. OHI-S index scores were obtained from the buccal surfaces and the lingual surfaces of the index teeth. The debris and calculus scores were calculated by adding the recorded scores and dividing it by the number of surfaces examined respectively. OHI-S score was obtained by adding the Debris Index (DI-S) and Calculus Index (CI-S) scores [11].
Turesky modification of Quigley Hein plaque index was assessed on the buccal, labial and lingual surfaces of all the teeth [11]. The index score was determined by dividing the total score obtained by the number of surfaces. This system of scoring plaque was chosen as it is relatively easier.
DMFT/deft index was assessed to determine the prevalence of dental caries [11].
Collection of saliva sample: The saliva sample was collected half an hour after brushing in the morning. The child was asked to bend down and spit the unstimulated saliva in a sterile container for five minutes [12].
The children were introduced to the chewable brush (Rolly Mini tooth brush, Rolly Brush s.r.l., 43126 Parma- Italy) and were taught how to brush [Table/Fig-1]. A video of how to use chewable brush was recorded and given to the staff employed in the institution. The staff was also provided with chewable tooth brush and was trained to use it. The children were advised to brush under the supervision for the next seven days twice daily. A demo was given and the children were observed by the investigator during their first use of chewable brush.

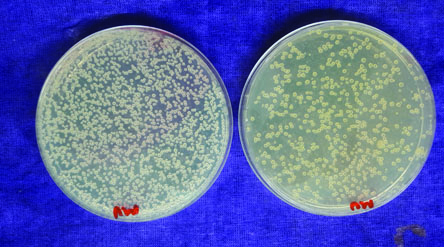
The collected saliva sample was sent to the laboratory for estimation of the S.mutans levels in the saliva. The sample was made into 1:40 dilutions and the samples were spread on the Mitis salivarius - bacitracin culture media. It was incubated for 48 hours at 37°C. After 48 hours, Streptococcus mutans appeared as small raised colonies on the plate. Colonies were identified and counted manually by the microbiology personnel who were blinded to the sample. The pH of the collected sample was also noted using pH strips (pH Balanced Life, Crystal Lake, IL.60039).
After seven days, the saliva sample was collected and the indices were assessed again. The saliva sample was sent to the lab for estimation of the S.mutans levels and pH of the saliva [Table/Fig-2].
S.mutans colonies in the saliva with manual brush and chewable tooth brush respectively.
Statistical Analysis
The raw data was entered in Microsoft excel sheet and the statistical analysis was done using SPSS version 21.0 (SPSS. Inc., Chicago III., USA) using paired t-tests to compare the pre-brushing and post-brushing index scores, salivary pH and salivary S. mutans counts.
Results
There were 10 children between the ages six-nine-year-old with a mean age of 7.1±0.99 participated in the study. The distribution of the subjects is shown in [Table/Fig-3]. The mean pre operative OHI-S index scores was 1.11±0.43 and the plaque index of these 10 children was 0.70±0.31 [Table/Fig-4].
Distribution of study subjects according to gender.
| Gender | N | % |
|---|
| Male | 6 | 60 |
| Female | 4 | 40 |
| Total | 10 | 100 |
Distribution of study subjects according to oral hygiene status and plaque index (PI) status.
| OHI(S) | Good | Fair | Poor | Total |
|---|
| Pre op | 5 | 5 | 0 | 10 |
| Post op | 10 | 0 | 0 | 10 |
| PI | Good | Fair | Poor | Total |
| Pre op | 10 | 0 | 0 | 10 |
| Post op | 10 | 0 | 0 | 10 |
The mean pre operative pH of the saliva was found to be 7.20±0.25 and the Streptococcus mutans level was found to be 740800.00±377956.14 CFU. The mean DMFT score was 5.0±1.414.
A significant reduction was seen in the debris index, oral hygiene index, plaque index, pH of the saliva and S.mutans level with manual brushing and after brushing with chewable brush [Table/Fig-5].
Comparison of parameters between pre op (prior to the use of chewable brush) and post operative (after seven days of using chewable brush) using paired t-test, p<0.05 significant.
| Parameters | Pre operative | Post operative | p-value |
|---|
| DI (S) | 0.79±0.32 | 0.41±0.40 | 0.001 (Significant) |
| CI (S) | 0.32±0.34 | 0.22±0.33 | 0.168 (Not Significant) |
| OHI (S) | 1.11±0.43 | 0.63±0.47 | 0.000 (Significant) |
| PI | 0.70±0.31 | 0.26±0.21 | 0.000 (Significant) |
| pH | 7.20±0.25 | 7.00±0.00 | 0.037 (Significant) |
| S. mutans | 740800.00±377956.14 | 299200.00±88940.430 | 0.006 (Significant) |
Discussion
Despite the increased awareness and numerous preventive measures available, dental caries remains to persist as a serious oral health problem. Various studies have shown that the dental caries is more prevalent in children [13,14]. This can be attributed to factors such as high intake of sugars, inability of the young children to brush their teeth properly and lack of oral health education [13,14].
Dental plaque is the direct precursor for dental caries and periodontal diseases. Understanding about the mechanism of formation of plaque is essential for development of control measures for these diseases [15]. Retention of the food and lowered buffering action of the saliva decreases the plaque pH, favours the growth of aciduric bacteria, increasing the risk of demineralization. On the other hand, when the plaque pH increases, super-saturation of the calcium and phosphorous is found in biofilm and saliva, restoring the lost minerals of the enamel by a process called remineralization. Thus, dental caries is a dynamic process that occurs due to the dental plaque that is present in the tooth surface, causing disturbance in the equilibrium resulting in loss of mineral from the tooth surface [1].
Effective plaque control measures can significantly contribute to the prevention of dental caries. In the present day, various chemical and mechanical methods are available, of which tooth brushing persists to be the most effective method [16]. Parent’s reasons for not brushing their children’s teeth has been assessed and was found that hectic schedule can be one of the causes for improper brushing in the children [17]. Effective manual brushing depends on various patient related factors such as use of proper tooth brush, tooth paste, adequate brushing technique and presence of proper motivation. Owing to the inability of the children to brush their teeth properly due to decreased manual dexterity, the effectiveness of chewable tooth brush (Rolly mini tooth brush), a recent innovation for plaque removal was investigated in the present study.
In the present study, oral hygiene status of the children aged six-nine years was assessed using OHI-S index and plaque index [2]. The children of six-nine-year-old were selected as they are in the mixed dentition period and are more prone to plaque accumulation. Both OHI-S index and plaque index were recorded for better accuracy in detecting the effectiveness of the chewable brush. It is found that there is a significant improvement in the oral hygiene of the children after using chewable brushes. This result was comparable to the study done by Bezgin T et al., which showed significant reduction in the overall plaque scores, proposing chewable brush to be an appropriate oral hygiene adjunct in the children [2]. Also, the results were found to be consistent with the study done by Myoken Y et al., in elderly population [10]. These findings suggest that chewable brush can be used as an effective alternative to the manual brushing in all kinds of population.
Evaluating the debris and calculus index individually, there was a significant reduction in the debris present around the tooth surface. However, a considerable change was not noticed in the calculus level. This indicates the need of professional oral health care despite the advancements in the oral hygiene methods [18].
In addition, the present study showed a marked reduction in S. mutans levels and a significant difference in the pH were noticed after using chewable brush. This could be attributed by the presence of fluoride and xylitol in the chewable brush [8]. Fluoride influences the metabolic activities and growth of the bacteria present in the dental plaque, reduces the rate of acid production and maintains higher levels of plaque pH [19,20]. A marked reduction in the S. mutans level in the plaque could be attributed to the fact that xylitol inhibits the adherence of bacteria to the plaque, and makes its removal easier [21,22]. The indication, contra-indication, advantages, disadvantages are discussed in [Table/Fig-6,7].
Indications and contra-indications of chewable brush.
| Indications | Contra-indications |
|---|
| 1. All kinds of population – children, elderly populations | 1. In individuals lacking cooperative ability |
| 2. Handicapped individuals and in others who lack manual dexterity | 2. In individuals with mental disability |
Advantages and disadvantages of chewable brush.
| Advantages | Disadvantages |
|---|
| 1. Convenient, quick and easy to use | 1. High cost |
| 2. No need of water | 2. Single use |
| 3. No need of tooth paste | 3. Potential risk of swallowing |
Limitation
The possible limitations of the study include smaller sample size. The impact of hawthrone and novelty effect on the children included in the study, beacuse they were advised to brush under the supervision of the staff and also as they were introduced to a newer method of brushing, could have introduced a bias in the research.
Clinical Significance
Scientific rationale for the study: Efficiency of the chewable tooth brush in decreasing the plaque and S. mutans level in saliva is not known.
Principal findings: The findings demonstrated that there is a marked reduction in the levels of S. mutans, plaque and debris after using the chewable tooth brush in children.
Practical implications: Chewable brush is an effective alternative to manual brushing and can be used in children with decreased dexterity. With adequate usage, it can reduce the occurrence of gingivitis and dental caries. It also serves as a handy tool to maintain oral hygiene at any time and any place.
Future Prospects
With this conception, chewable brush can be effectively used in children for effective reduction of both plaque and caries. However, long term studies are needed to determine the role of chewable tooth brush in caries prevention and also to determine if its usage is satisfactory in children with reduced manual dexterity.
Conclusion
The use of chewable brush not only exhibited the potential of maintaining good oral hygiene by significantly reducing the plaque and debris level but also with long term and proper use can significantly reduce the S. mutans level in the saliva preventing the development of caries. Hence, chewable brush can be effectively used as an alternative to manual tooth brushing in children.