Chaput Tubercle Fracture in an Adult- A Rare Case Report
Pankaj Kumar Mishra1, Vikram Patidar2, Satya Prakash Singh3
1 Assistant Professor, Department of Orthopaedics, G.M.C and Hamidia Hospital, Bhopal, Madhya Pradesh, India.
2 Senior Resident, Department of Orthopaedics, G.M.C and Hamidia Hospital, Madhya Pradesh, India.
3 Private Practioner, Satya Trauma Center, Varansi, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pankaj Kumar Mishra, E-115/4, Shivaji Nagar, Bhopal-462016, Madhya Pradesh, India.
E-mail: drpankajv@yahoo.com
Chaput tubercle fracture occurs at the antero-lateral position of the distal tibia in adult as a counterpart of adolescent Tillaux fracture. It is a case of adult male which presented to us with onset of acute pain, swelling and restricted movements of ankle after a road side accident. A clinical diagnosis of Chaput tubercle fracture was established after a CT-scan. The displaced fracture was managed by open reduction and internal fixation by screw. At the end of follow up, the foot and ankle ability score measured. Through this case report we convey that Chaput tubercle fracture in an adult is a rare entity.
Antero-lateral, Avulsion fracture, Distal tibial epiphysis
Case Report
A 33-year-old male presented to the causality of the hospital after encountering a road accident about an hour ago. The patient experienced a head on collision with another bike while driving his two wheeler. The patient complained of pain, contusion and swelling over the anterior aspect of left ankle. On examination, tender swelling with pain and restricted movement of ankle was noted. No associated history of vomiting, unconsciousness or any related injuries was found except the superficial abrasion over the dorsum of ipsilateral hand.
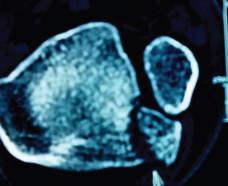
The antero-posterior and lateral X-rays were carried out which revealed a suspicious intra-articular fracture of the antero-lateral part of the distal tibia. For the diagnostic confirmation the CT- scan of the left ankle was done, which confirmed the displaced Chaput tubercle fracture [Table/Fig-1,2].
Computed tomography showing the displaced antero-lateral part of the distal tibia.
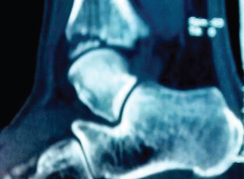
In the sagittal section of computed tomography showing the intra-articular confinement of the avulsion.
The informed consent was taken from the patient and surgical intervention was planned. The antero-lateral approach was used for the open reduction. Intraoperatively the K-wire was used to manipulate the fracture as a “joystick” and fixed with canulated 4 mm lag screw [Table/Fig-3]. Postoperatively the POP slab and IV antibiotics (ceftriaxone and amikacin for three days) was given. Sutures were removed and ankle movement was started on postoperative day 11. Full range of movement was achieved in the next six days. Partial weight bearing started at sixth weeks of followup and the full weight bearing allowed at 10th weeks. Patient was on regular follow up for one year and the Foot and Ankle Ability Measure (FAAM) score was 97% (100/116) and the patient has satisfactory clinico-radiological union [Table/Fig-4,5].
Immediate postoperative oblique and AP view of Chaput tubercle fracture.

One-year-old follow-up AP view of fixed Chaput tubercle fracture.

One-year-old follow-up oblique view of the fixed Chaput tubercle fracture.

Discussion
Tillaux fracture occurs at the antero-lateral part of the lower end of tibial epiphysis and has a tendency to be displaced with the variable amounts. The epiphysis of distal tibia starts fusing from the middle, and first goes medially then the lateral side (12-14 years in female and 15-18 years in male). So that in the adolescent age group the Tillaux fracture is common because the lateral side of distal tibia is about to fuse which make it vulnerable for being avulsed when the anterior-inferior tibiofibular ligament (usually stronger than physis) fails to rupture during external rotation injury in the adolescents [1]. Since it is the transition period of epiphysiodesis which occurs during the adolescence to skeletal maturity so also known as transition fracture. The transition fracture of ankle is classified by Von Laer L as biplane and triplane fracture and the biplane fracture of epiphysis is analogous to Tillaux fracture [2].
The triplane fracture of the lower tibial epiphysis was first described by Marmor and has transverse component through growth plate, coronal component through posterior tibial metaphysic (Salter-harris type II or IV in lateral view) and saggital component (Salter-harris type III in AP view) in distal tibial epiphysis [3]. On the contrary the Tillaux fracture is a biplane fracture, so the radiological diagnosis of Tillaux fracture is utterly arduous due to the lack of coronal component of the fracture as the triplane (Marmor-Lynn) fracture [4]. Since the traditional radiography is not always sufficient to confirm the diagnosis, so the CT scan becomes necessary to understand the fracture orientation to clinch the diagnosis.
Usually in the adult the ligament is supposed to rupture before the avulsion fracture of antero-inferior part of tibial plafond due to epiphysiodesis. So, the avulsion fracture of antero-inferior part of distal tibia (rather than ligament rupture) in adult becomes the rarebit finding (Chaput tubercle fracture) which entails it as a rare entity [5].
Non-displaced fracture (≤ 2mm displacement) can be managed conservatively by long leg cast with internally rotated foot. Since the strong antero-inferior ligament is attached to the fibula, it renders it displaced and angulated [6]. So the displaced fracture is managed by close/open reduction and internal fixation [7].
In our case, the open reduction was done by antero-lateral approach and fracture segment was fixed by screw.
Conclusion
Chaput tubercle fracture is an unusual fracture in adult. The conventional radiology may not suffice to clinch the diagnosis sometimes. Due to the displacement and angulations, it can be better managed by surgery.
[1]. Hasler C, Hardegger F, Fracture of the Tillaux-Chaput tubercle–a case from pediatric traumatologyZ Unfallchir Versicherungsmed 1993 86(3):149-51. [Google Scholar]
[2]. Von Laer L, Classification, diagnosis, and treatment of transitional fractures of the distal part of the tibiaJ Bone Joint Surg Am 1985 2013:687-98. [Google Scholar]
[3]. Marmor L, An unusual fracture of the tibial epiphysisClin Orthop Relat Res 1970 73:132-35. [Google Scholar]
[4]. Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD, Radiologic evaluation of juvenile tillaux fractures of the distal tibiaJ Pediatr Orthop 2001 21:162-64. [Google Scholar]
[5]. Kumar N, Prasad M, Tillaux fracture of the ankle in an adult: A rare injuryJournal of Foot and Ankle Surgery 2014 53(6):757-58. [Google Scholar]
[6]. Cooperman DR, Spiegel PG, Laros GS, Tibial fractures involving the ankle in children: the so-called triplane epiphyseal fractureJ Bone Joint Surg (Am) l978 60-A:l040-46. [Google Scholar]
[7]. Cooper AP, On dislocation of the ankle jointsIn: A Treatise on Dislocations and on Fractures of the joints 1822 LondonLongman, Hurst, Reese, Orme and Brown. E Cox and Son [Google Scholar]