Kedo-S Paediatric Rotary Files for Root Canal Preparation in Primary Teeth – Case Report
Ganesh Jeevanandan1
1 Senior Lecturer, Department of Paedodontics and Preventive Dentistry, Saveetha Dental College, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ganesh Jeevanandan, 1247/3, Mohanam Apartments, Golden Colony, Mogappair, Chennai-600037, Tamil Nadu, India.
E-mail: helloganz@gmail.com
Nickel-Titanium (Ni-Ti) instrument are widely used for root canal preparation in permanent tooth compared to primary teeth. Hand instrumentation technique remains the conventional method for root canal preparation in primary teeth. The time taken for root canal preparation with the conventional method is more resulting in patients and clinicians fatigue. Recently Ni-Ti rotary files designed for permanent tooth has been used for root canal preparation in primary teeth. Using rotary instruments for primary tooth pulpectomies resulted in better and predictable root canal filling. This article presents case reports of pulpectomy treatment performed using Kedo-S an exclusive paediatric Ni-Ti rotary files. The advantages and disadvantages in use of Ni-Ti rotary files in primary teeth are discussed in this article.
Ni-Ti files, Primary molars, Pulpectomy
Case Report
Case-1
A four-year-old child was referred to the Department of Paedodontics and Preventive Dentistry, complaining of pain in his left lower posterior region for past five days. Pain was sharp, localized and present during night. No treatment was rendered for the past five days. His medical history was found to be noncontributory. Clinical examination of the left mandibular primary second molar revealed dental caries involving enamel and dentin with tenderness on percussion. Intraoral Periapical Radiograph (IOPA) of the decayed tooth region showed radiolucency involving enamel, dentin and pulp in left mandibular primary second molar [Table/Fig-1]. Based on clinical and radiographic interpretation a diagnosis of dental caries with symptomatic irreversible pulpitis was made and pulpectomy procedure was planned. The tooth was anaesthetized using 2% lignocaine with 1:80,000 adrenaline (Lignox, Indoco Remedies Ltd. Mumbai, India). An endodontic access opening was prepared using no 330 pear shaped bur (Mani, Inc, Tochigi, Japan). The coronal tissue was removed using a No 19W Spoon Excavator (Hu-Friedy Mfg. Co. LLC). The mesiobuccal and mesiolingual canals were explored with a size 10 K-file (Mani, Inc, Tochigi, Japan) and the distal canal with a size 15 K-file. A working length was determined using pre-operative radiograph and measured 1 mm short of the apex. Biomechanical preparation was performed using crown-down technique with Kedo-S Ni-Ti rotary instruments. D1 rotary file was used to prepare the mesiobuccal and mesiolingual canals [Table/Fig-2]. E1 rotary file was used to prepare the distal canal [Table/Fig-3]. Normal saline was used as irrigating solution during canal preparation. RC helps (Prime dental products Pvt. Ltd. India), a 17% EDTA gel was used as a lubricating paste during canal preparation with rotary files. The root canal space was obturated with Metapex (Meta Biomed Co. Ltd. Chungbuk, Korea). The Metapex syringe was inserted into the root canal space, near the apex. The paste was pressed down into the canals and the syringe was slowly withdrawn. The immediate postoperative radiograph revealed optimal filling with metapex in relation to left mandibular primary second molar [Table/Fig-4]. The coronal seal of the endodontically treated tooth was done with glass ionomer cement (GC Fuji II, Tokyo, Japan). Finally size four stainless steel crown (3M ESPE, St, Paul, MN, USA) was cemented using type I glass ionomer cement. On recall visit six months later, an IOPA radiograph revealed no pain without any evidence of mobility [Table/Fig-5].
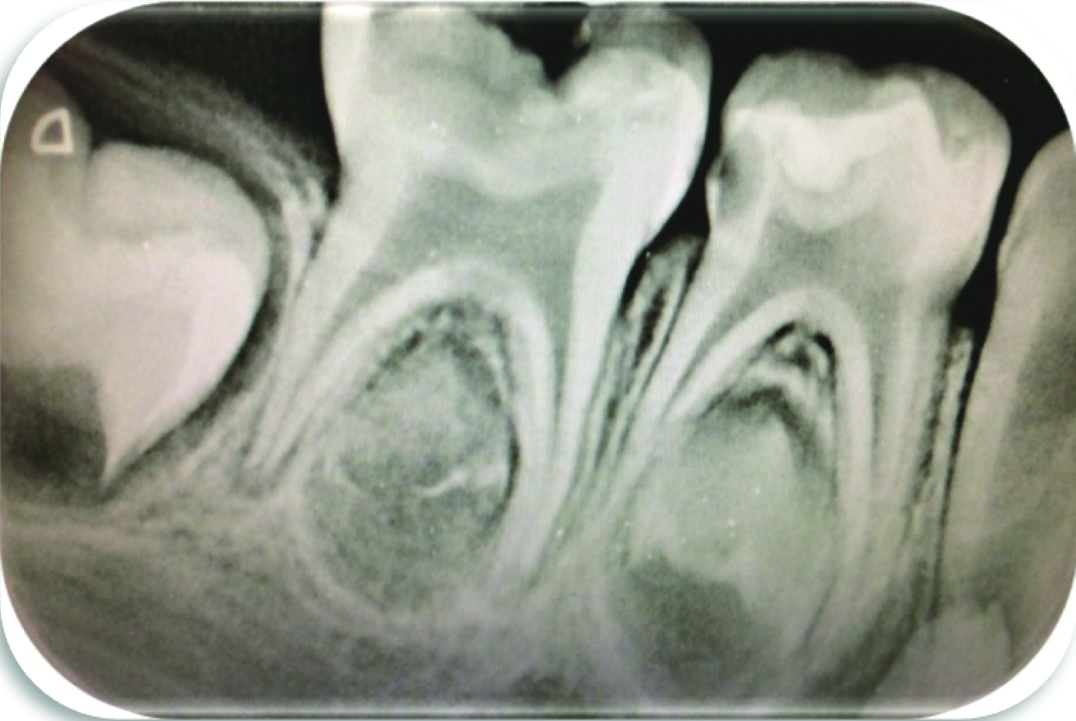
Preoperative radiograph showing radiolucency involving pulp in relation to left mandibular second molar.

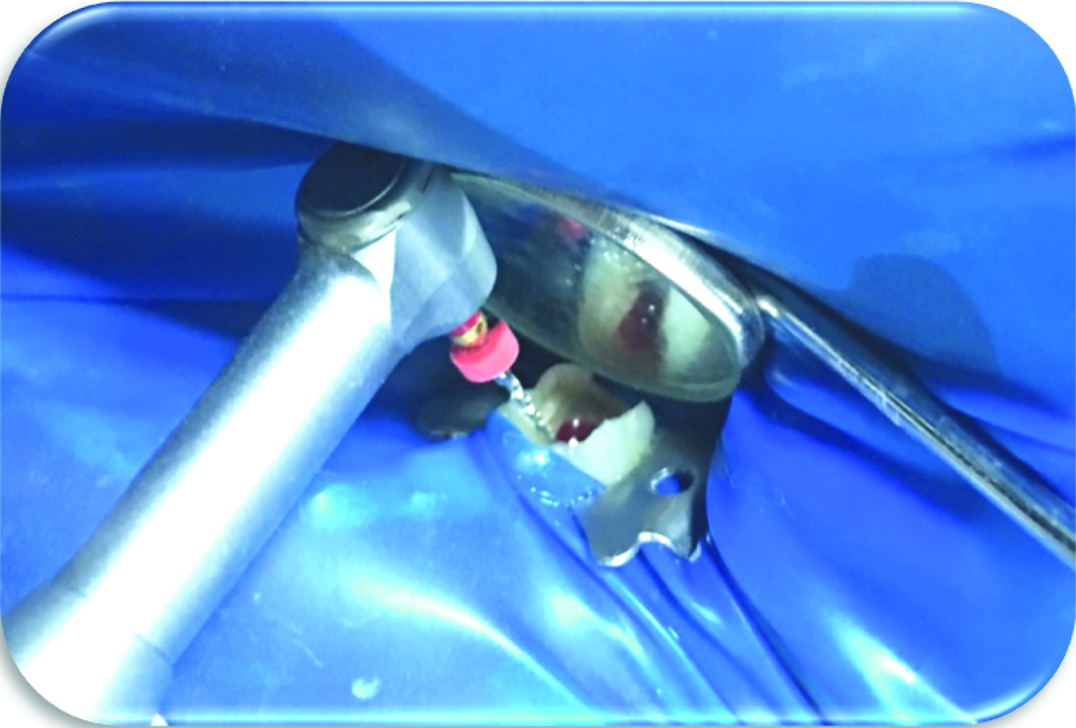
Clinical Image showing root canal preparation done using D1 rotary file in relation to mesial canal of left mandibular second molar.
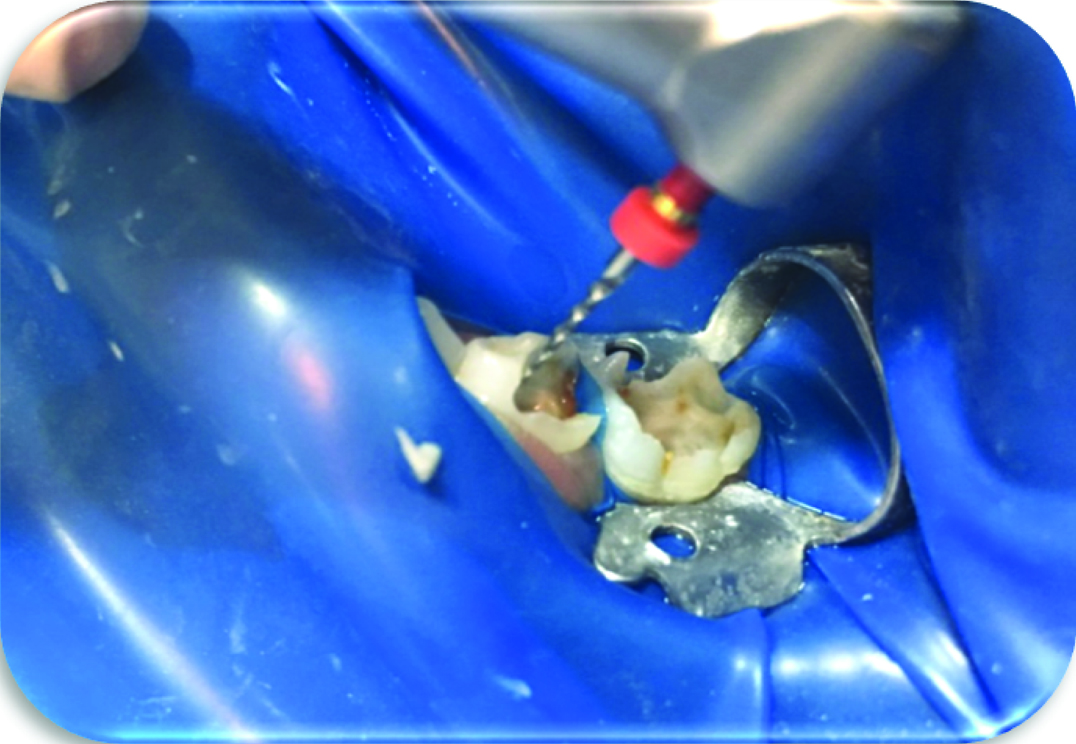
Clinical image showing root canal preparation done using E1 rotary file in relation to distal canal of left mandibular second molar. (Images left to right)

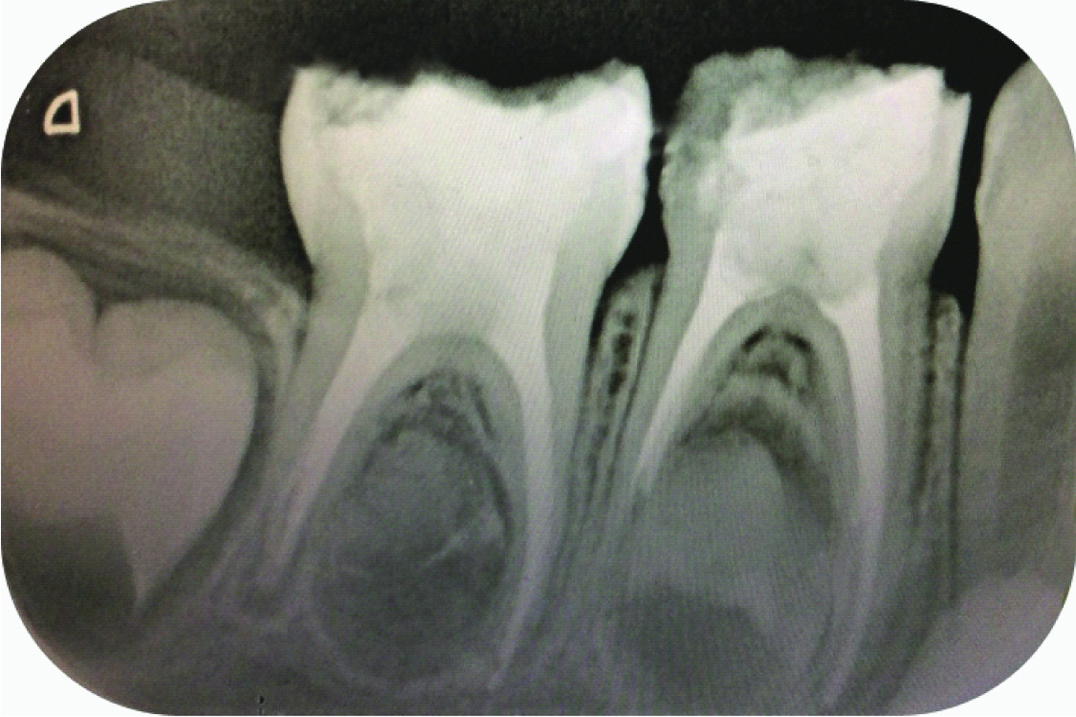
Postoperative radiograph showing obturation with metapex in relation to left mandibular primary second molar.

Postoperative radiograph after six months with no evidence of furcal infection in relation to left mandibular primary second molar.

Case-2
A four and half-year old girl child was referred to the Department of Paedodontics and Preventive Dentistry, with a complaint of pain in her left lower posterior region for past seven days. Pain was dull, localized and present during night. The child was under analgesic for the past seven days. Her medical history was found to be noncontributory. Clinical examination of the left mandibular primary first and second molars had deep carious lesion. No swelling or sinus was present. Both the teeth were tender on percussion. IOPAR revealed radiolucency involving pulp in relation to left mandibular primary first and second molars [Table/Fig-6]. Based on clinical and radiographic interpretation a diagnosis of dental caries with symptomatic irreversible pulpitis was made and pulpectomy procedure was planned. Left inferior alveolar nerve block was administered to anaesthetize both first and second molars using 2% lignocaine with 1:80,000 adrenaline (Lignox, Indoco Remedies Ltd. Mumbai, India). Access opening was done for both the molars followed by removal of coronal tissue. The mesiobuccal, mesiolingual and distal canals were located using appropriate size K-file. A working length was determined using pre-operative radiograph. Biomechanical preparation was performed with Kedo-S Ni-Ti rotary instruments. In second primary molar, D1 rotary file was first used followed by E1 rotary file to prepare the mesiobuccal canal. Only D1 rotary file was used to prepare mesiolingual canal because the canal was narrow compared to mesiobuccal canal. E1 rotary file was used to prepare the distal canal [Table/Fig-7]. In first primary molar D1 rotary file was used to prepare the mesiobuccal and mesiolingual canals. E1 rotary file was used to prepare the distal canal [Table/Fig-8]. The prepared root canals were obturated with Metapex [Table/Fig-9]. The coronal seal was obtained with glass ionomer cement (GC Fuji II, Tokyo, Japan). Finally size five stainless steel crown was selected for second molar followed by size four crowns for first molar (3M ESPE, St, Paul, MN, USA) was cemented using type I glass ionomer cement. At six months follow up both teeth revealed no pain, furcal lesion and no evidence of mobility [Table/Fig-10].
Pre-operative radiograph showing radiolucency involving pulp in relation to left mandibular first and second molars. (Images left to right)
Clinical image showing root canal preparation done using E1 rotary file in relation distal canal of left mandibular second molar.

Clinical image showing root canal preparation done using D1 rotary file in relation mesial canal of left mandibular first molar.
Postoperative radiograph showing obturation with metapex in relation to left mandibular primary first and second molars. (Images left to right)
Postoperative radiograph after six months with no evidence of furcal infection in to relation left mandibular primary first and second molars.

Discussion
In paediatric dentistry the most important concerns is the loss of necrotic primary molars leading to space loss. Pulpectomy is considered to be the treatment of choice for primary teeth with pulp involvement. Bacteria plays an important role in the initiation and perpetuation of pulpal and periapical disease [1]. During cleaning and shaping the root canal system the primary objective is to remove soft and hard bacteria-containing tissue. Proper cleaning and shaping aids the irrigant to reach the apical third of the root during irrigation process resulting in sterile root canal for obturation [2]. Endodontic treatment is performed using reamers, files; burs, sonic instruments, and Nickel–Titanium (Ni–Ti) rotary file systems. Canal preparation with hand file techniques are time consuming and can lead to iatrogenic errors like ledging, zipping, canal transportation and apical blockage. This resulted in use of Ni-Ti rotary files for root canal preparation during endodontic treatment which reduces above mentioned complications [3]. In present case reports, the Kedo-S Ni-Ti rotary instruments were used to prepare the root canals of the primary molars. The Kedo-S file system (Reeganz dental care Pvt. Ltd. India) consists of three Ni-Ti rotary files. The total length of the files is 16 mm. The working length of the files is 12 mm. The files are named as D1, E1, U1, respectively. All the files have a variable taper corresponding to the use in primary teeth. D1 file has a tip diameter of 0.25 mm with a variable taper. It can be used in primary molars with narrow canals (mesial canals in mandibular molars and disto buccal canal in maxillary molars). E1 file has a tip diameter of 0.30 mm and can be used in wider molar canals (distal canal in mandibular molars and palatal canal in maxillary molars). U1 has a tip diameter of 0.40 mm and used in primary incisor teeth [Table/Fig-11]. The taper of the instruments are designed according to the diameter of primary teeth with narrow and wide root canals. Kedo-S paediatric rotary file system must be used in a low speed constant- torque handpiece. The ideal rotation speed is 150-300 rpm. Various studies have shown that Ni-Ti instruments are efficient and effective for root canal preparation in permanent teeth [4–9]. Barr ES et al., used Ni-Ti ProFile 0.04 taper rotary files for pulpectomy procedures and concluded that use of Ni-Ti files resulted in a uniform and predictable root canal fillings [10]. Although these files are frequently used for permanent teeth, a major concern in applying them for primary teeth is the possibility of lateral perforation on the inner surface of primary teeth. These lateral perforations can be due to the predesigned greater taper of the rotary files [11]. Primary teeth have shorter, thinner, curved roots and ribbon-shaped morphology compared to permanent teeth [12]. The above parameters hamper the use of existing rotary files designed for permanent teeth. The kedo-S paediatric rotary files have a gradual taper aiding in easy coronal enlargement and straight line access. This gradual taper also help in efficient canal preparation and avoids over instrumentation of the inner wall of root surface. It is necessary to use copious amount of irrigating solution to remove any loose pulp tissue and to ensure canal walls are clean before obturation. The obturating material used was Metapex containing calcium hydroxide and iodoform. Metapex provides adequate bacterial control after obturation [13]. The advantage of kedo-S Ni-Ti alloy instruments is to preserve the original anatomy of the curved canals in primary teeth during canal preparation. The clockwise motion of kedo-S rotary file pulls pulpal tissue and dentin out of the canal resulting in effective cleaning of primary molar canals. The duration of canal preparation is reduced using kedo-S rotary file system in primary teeth approximately 2-3 minutes. This would help to reduce fatigue of the patient and operator resulting better quality of treatment. Uniform canal preparation is obtained using rotary files resulting in better quality of obturation. The cost of constant torque hand-piece and Ni-Ti rotary files are the disadvantages. The use of Ni-Ti instruments are technique sensitive and proper training is required for the operator. After six months follow up, both cases showed clinical as well as radiographic success.
Picture showing Kedo-S paediatric Ni-Ti rotary files – Red colour coded- 0.25 tips diameter, Blue colour coded- 0.30 tip diameter and Black colour coded- 0.40 tip diameter used for root canal preparation in primary teeth.

Conclusion
The Kedo-S paediatric rotary file system will help the dentist in performing the pulpectomy procedure faster. These instrumentation techniques are considered to be an effective method to debride the uneven walls of primary teeth. The root canal preparation with the paediatric rotary file system has consistently resulted in uniform and predictable quality of obturation. However, considering better root canal preparation and quality of obturation, the use of Kedo-S paediatric rotary files is recommended for pulpectomy procedure in primary teeth.
[1]. Cohen S, Hargreaves KM, Pathways of the Pulp 2006 9th edSt. LouisMosby Publishers:301-311.:842 [Google Scholar]
[2]. Siqueira JF Jr, Araújo MC, Garcia PF, Fraga RC, Dantas CJ, Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canalsJ. Endod 1997 23(8):499-502. [Google Scholar]
[3]. Walton RE, Torabinejad M, Principles and Practice of Endodontics 2002 3rd edSaunders Company:222 [Google Scholar]
[4]. Kummer TR, Calvo MC, Cordeiro MM, de Sousa Vieira R, de Carvalho Rocha MJ, Ex-vivo study of manual and rotary instrumentation techniques in human primary teethOral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 105(4):e84-92. [Google Scholar]
[5]. Silva LA, Leonardo MR, Nelson-Filho P, Tanomaru JM, Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molarsJ Dent Child 2004 71(1):45-47. [Google Scholar]
[6]. Crespo S, Cortes O, Garcia C, Perez L, Comparison between rotary and manual instrumentation in primary teethJ Clin Paediatr Dent 2008 32(4):295-98. [Google Scholar]
[7]. Azar MR, Safi L, Nikaein A, Comparison of the cleaning capacity of Mtwo and ProTaper rotary systems and manual instruments in primary teethDent Res J 2012 9(2):146-51. [Google Scholar]
[8]. Madan N, Rathnam A, Shigli AL, Indushekhar KR, K-file vs Profiles in cleaning capacity and instrumentation time in primary molar root canals: an in vitro studyJ Indian Soc Pedod Prev Dent 2011 29(1):2-6. [Google Scholar]
[9]. Nagaratna PJ, Shashikiran ND, Subbareddy VV, In vitro comparison of NiTi rotary instruments and stainless steel hand instruments in root canal preparations of primary and permanent molarJ Indian Soc Pedod Prev Dent 2006 24(4):186-91. [Google Scholar]
[10]. Barr ES, Kleir DJ, Barr NV, Use of nickel titanium rotary files for root canal preparation in primary teethPaediatr Dent 2000 22:77-78. [Google Scholar]
[11]. Kuo CI, Wang YL, Chang HH, Huang GF, Lin CP, Li UM, Application of Ni-Ti rotary files for pulpectomy in primary molarsJ Dent Sci 2006 1:10-15. [Google Scholar]
[12]. Finn SB, Morphology of primary teethIn “Clinical Pedodontics” 4th ed, Finn SB, ed 1973 PhiladelphiaSaunders Co:59-70. [Google Scholar]
[13]. Nurko C, Ranly DM, Garcia-Godoy F, Lakshmya KN, Resorption of a calcium hydroxide/iodoform paste (Vitapex®) in root canal therapy for primary teeth: a case reportPaediatr Dent 2000 22:517-20. [Google Scholar]