Case Report
A 55-year-old (para 3 living 3) postmenopausal female (menopause attained 10 years back) presented to the out-patient gynaecology clinic with the chief complaints of a long standing, painless yet gradually increasing in size, abdominal lump along with heaviness in abdomen for last two years and significant weight loss (almost 50%) over the past one year. There was history of loss of appetite and constipation. No significant risk factors for malignancy could be elicited from her past medical history or family history.
General physical examination was unremarkable except for mild pallor and low (15) BMI. There was an abdomino-pelvic mass corresponding to 30 weeks size gravid uterus, occupying all quadrants of abdomen. It was a non-tender, variegate consistency lump with restricted mobility. Pelvic examination confirmed the same mass felt through the anterior and left fornix and a retroverted atrophic uterus was felt separately from the mass. Movements of the mass could not be transmitted to the cervix and the pouch of Douglas appeared free.
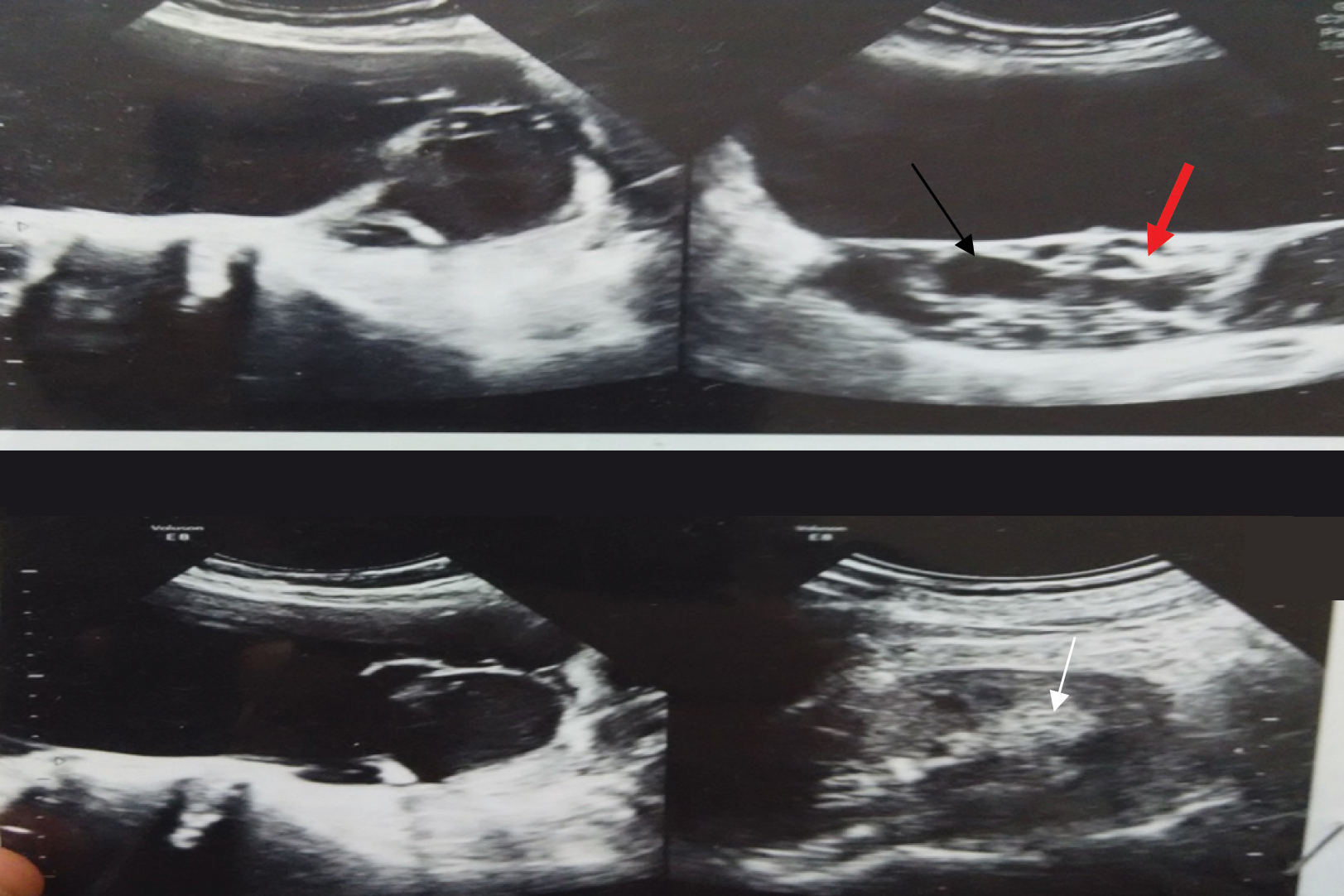
Haematological investigations revealed mild anaemia (Hb-9.5 gm%). Other routine tests including thyroid function tests and HIV were normal. Serum level of CA 19-9 was 1999 U/ml, while CA-125, LDH, AFP, β-hCG were within normal ranges. Transabdominal ultrasonography [Table/Fig-1] showed a 27 cm x 15.5 cm x 12.3 cm multiloculated cystic mass with occasional solid areas with thick septae and few internal echoes arising from left ovary. Uterus was atrophic, retroverted with endometrial thickness of 2 mm. Right ovary appeared normal and no ascites could be noted. Risk of Malignancy Index (RMI) was 270 (UxMxCA-125=3x3x30) which was a high risk RMI.
Grayscale transabdominal ultrasonographic picture showing multiloculated (black arrow), solid cystic mass (black and white arrow) with thick septae (red arrow) arising from left ovary.
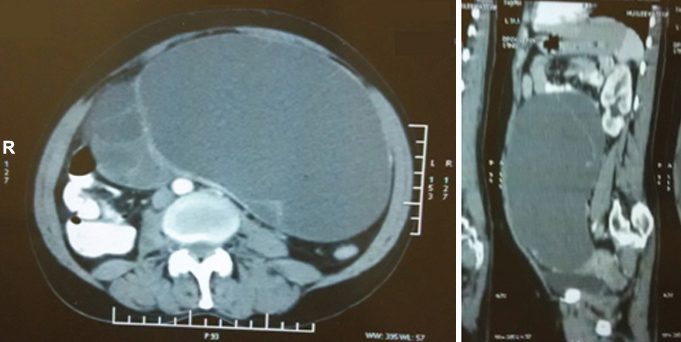
Magnetic Resonance Imaging (MRI) of abdomen and pelvis (axial and sagittal view) [Table/Fig-2] showed large multiloculated cystic tumour arising from left adnexa with thick septations with varying density of loculations. Uterus and opposite adnexa along with other abdominal organs were unremarkable.
MRI of abdomen, saggital and axial view showing large multiloculated cystic tumour arising from left adnexa with thick septations.
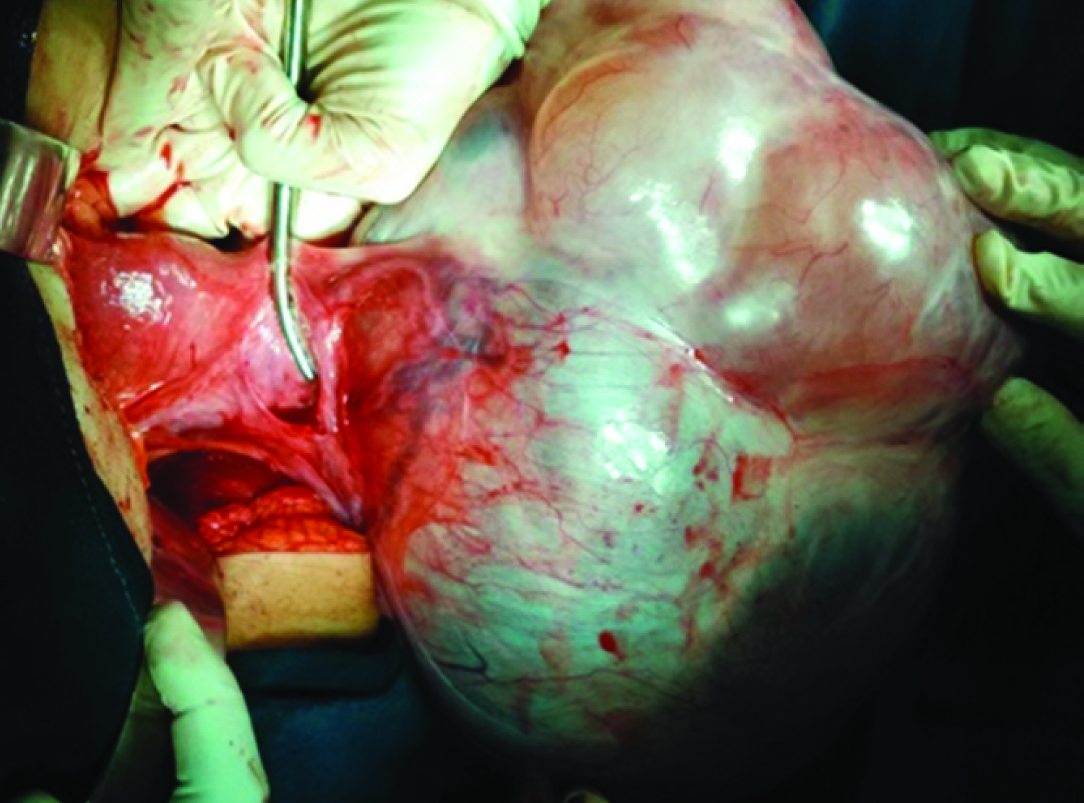
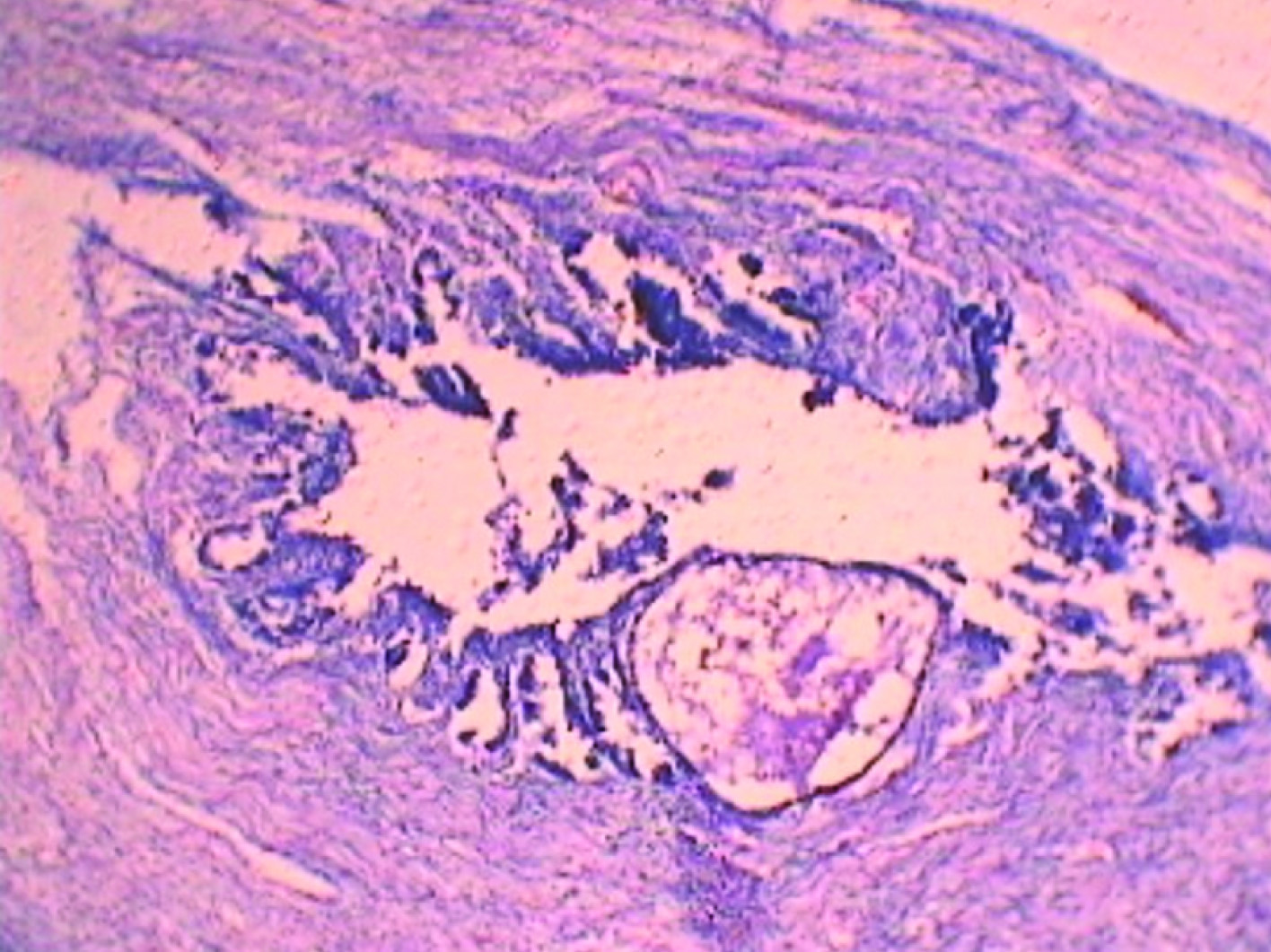
In view of the large tumour and abnormally high tumour marker CA 19-9, the patient was taken up for staging laparotomy. A large lobulated ovarian cyst with bosselated surface with overlying congested vessels but no extra-capsular or surface extension, replacing the left ovary was noted [Table/Fig-3]. Apart from peritoneal washings, a thorough exploration of abdominal and pelvic cavities, palpation for para-aortic lymph nodes and omental biopsy, total abdominal hysterectomy along with bilateral salpingo-oopherectomy was performed considering the possibility of malignancy in this postmenopausal woman. All other abdominal and pelvic organs were normal and para-aortic lymph nodes were not palpable. The 26 cm x 16 cm x 11 cm lobulated tumour weighing 5.4 kg had a thick wall with solid and cystic areas filled with mucinous fluid. Histopathology revealed it to be a benign mucinous cystadenoma of the ovary with no evidence of atypia or stromal invasion [Table/Fig-4]. In view of such high CA 19-9 levels, multiple sections from the specimen were evaluated to rule out possibility of malignancy. All other specimens taken preoperatively were also disease free. Immunohistochemical staining for CA 19-9 was not available at our centre and hence was not performed. The patient fared well through her postoperative period.
Peroperative image showing a large lobulated ovarian mass with bosselated surface with overlying congested vessels replacing the left ovary.
Low power (100x magnification) of the ovarian tumour showing the non-ciliated lining, mucin-secreting, columnar epithelium (H&E stain).
Two months following the surgery, the CA 19-9 levels had regressed to normal range. The patient has been symptom-free thereafter and the CA 19-9 levels have also remained normal until date, i.e., six months past the surgery.
Discussion
Carbohydrate antigen 19-9 (CA 19-9) (a sialylated lewis glycoprotein antigen), a commonly used marker of benign and malignant hepatobiliary and pancreatic conditions [1], has also been found to be raised in some ovarian neoplasms.
Ovarian mucinous cystadenomas, accounting for 8%-10% of surface epithelial neoplasms of the ovary, are multiloculated, cystic ovarian tumours with mucin-secreting epithelium, derived from primitive mesoderm with capability to undergo metaplasia and resemble those of endocervix, gastric pylorus, or intestine.
Although CA 19-9 has been found to be raised in borderline mucinous tumours and malignant mucinous carcinoma [2], but there are only a few reports with such high serum levels of this marker in an intact benign ovarian mucinous cystadenoma [3,4]. In our case, ovarian neoplasm in a 55-year-old postmenopausal female, appeared to be malignant clinico-radiologically and biochemically due to very high serum CA 19-9 levels, but ultimately turned out to be a benign mucinous cystadenoma of the ovary.
Transvaginal sonography along with serum levels of CA 125 helps in early diagnosis of primary epithelial ovarian neoplasm, but it is found normal in most of the primary mucinous ovarian neoplasms, where CA19-9 is used instead [5].
CA 19-9 is a tumour associated mono-sialo-ganglioside glycoprotein antigen related to the Lewis blood group protein. The reference range of serum CA 19-9 is less than 37 U/mL. The antigen is present in epithelial tissues of the pancreas and hepatobiliary tree, and is often secreted by mucinous tumours of the gastrointestinal tract, including the pancreas and hepatobiliary tract [1,2].
CA 19-9 has been cited as more specific marker than CA 125 in the diagnosis of advanced cases of ovarian malignancy [6]. It has been widely studied and reported in association with mature cystic teratomas of the ovary where unusually high levels have been reported [7–9].
However, only a few studies have shown that this tumour marker may also be elevated in benign primary ovarian mucinous neoplasms [2].
Kelly DJ et al., demonstrated markedly elevated serum CA 19-9 in borderline mucinous tumours and mucinous carcinomas. They also established a weak but statistically significant correlation between tumour’s maximum dimension and CA 19-9 level [2]. Thus high CA 19-9 levels are commoner with malignant and borderline mucinous cysts. Similar to our finding, Kelly PJ et al., has suggested that CA 19-9 cannot be used to predict the histological type of ovarian tumour [2]. In our case too, multiple specimen sections were examined and malignancy and borderline lesion were ruled out.
Engelen MJ et al., observed raised CA 19-9 levels in 46% borderline ovarian tumours. In patients with mucinous tumours preoperative CA 19-9 was more frequently elevated (57%) than CA 125 (15%) or CEA (11%). Thus, they suggested that if one chooses to use serum markers in follow-up of mucinous borderline ovarian tumours, CA 19-9 should be included [7].
Our patient had unusually raised serum levels of CA-19-9 with a big benign tumour. When interpreted in context with her alarming weight loss, large size of the tumour with multiloculations, thick septations and internal echoes and RMI (270) suggesting high risk for malignancy, we harboured a very high clinical suspicion of malignancy preoperatively for our case. Preoperatively too, the presence of focal solid areas in the tumour added to our presumption. The weight loss could have been because reduced appetite and dyspepsia she had owing to the big size of the tumour. We undertook a staging laparotomy and in addition to the routine protocol, performed total abdominal hysterectomy and bilateral sapingo-oopherectomy, since the patient was 10 years postmenopausal and harbouring a suspicious ovarian mass. The procedure was in accordance with current RCOG recommendations [10]. Level of the tumour marker however helped us in postoperative follow up.
Brain O et al., and Pyeon SY et al., described markedly high levels of 2880 U/ml and 2753 U/ml in a case with ruptured ovarian mucinous cyst adenoma associated with ascites [3,4].
In our patient the level was elevated to 1990 U/ml probably contained by the intact cyst wall. In our patient we reassessed CA 19-9 level after eight weeks to assess the completeness of surgery and it returned to normal. Thus, the use of tumour markers is more for follow up, rather than diagnosis where its role is limited.
Conclusion
Marked increase in serum levels of CA 19-9 is possible in benign ovarian mucinous cystadenomas. Preoperative use of tumour marker for prediction of ovarian malignancy should be avoided as it adds to patient’s anxiety and clinician’s dilemma about benign nature of the disease.
Consent
A written informed consent was obtained from the patient for publication of this case report.
[1]. Steinberg WM, Gelfand R, Anderson KK, Glenn J, Kurtzman SH, Sindelar WF, Comparison of the sensitivity and specificity of the CA19-9 and carcino-embryonic antigen assays in detecting cancer of the pancreasGastroenterology 1986 90(2):343-49. [Google Scholar]
[2]. Kelly PJ, Archbold P, Price JH, Cardwell C, McCluggage WG, Serum CA19.9 levels are commonly elevated in primary ovarian mucinous tumours but cannot be used to predict the histological subtypeJ Clin Pathol 2010 63(2):169-73. [Google Scholar]
[3]. Brain O, Brown LHW, Suvarna S, Chapman R, Markedly elevated CA19-9 associated with benign ovarian cyst and ascitesBMJ Case Rep 2009 2009:piibcr11.2008.1219 [Google Scholar]
[4]. Pyeon SY, Park JY, Ki KD, Lee JM, Abnormally high level of CA-19-9 in a benign ovarian cystObstetrics and Gynecology Science 2015 58(6):530-32. [Google Scholar]
[5]. Cho HY, Kyung MS, Serum CA19-9 as a predictor of malignancy in primary ovarian mucinous tumours: a matched case-control studyMed Sci Monit 2014 20:1334-39. [Google Scholar]
[6]. Al-Hadithi HS, Al-Derzi AR, CA19-9 tumour marker in comparison with CA 125 in patients with gynecological diseasesIOSR Journal of Dental and Medical Sciences (IOSR-JDMS) 2014 13(2):01-04. [Google Scholar]
[7]. Engelen MJ, de Bruijn HW, Hollema H, ten Hoor KA, Willemse PH, Aalders JG, Serum CA 125, carcinoembryonic antigen, and CA 19-9 as tumour markers in borderline ovarian tumoursGynecol Oncol 2000 78(1):16-20. [Google Scholar]
[8]. Kyung MS, Choi JS, Hong SH, Kim HS, Elevated CA 19-9 levels in mature cystic teratoma of the ovaryInt J Biol Markers 2009 24(1):52-56. [Google Scholar]
[9]. Coskun A, Kiran G, Ozdemir O, CA 19-9 can be a useful tumour marker in ovarian dermoid cystsClin Exp Obstet Gynecol 2008 35(2):137-39. [Google Scholar]
[10]. Royal college of Obtetricians and Gynaecologists. Ovarian cysts in postmenopausal women. Guideline no. 34. Oct 2003 Reviewed 2010 [Google Scholar]