Cannon Ball Lung Metastases from a Previously Unreported Primary
Arjun Lakshman1, Ram V. Nampoothiri2, Vikas Suri3, Subhash Varma4
1 Senior Resident, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
2 Senior Resident, Department Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
3 Associate Professor, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
4 Professor and Head, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vikas Suri, Associate Professor, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh-160012, India.
E-mail: 2pgimedicine2015@gmail.com
Cannon ball metastases, Follicular neoplasm, Thyroid malignancy
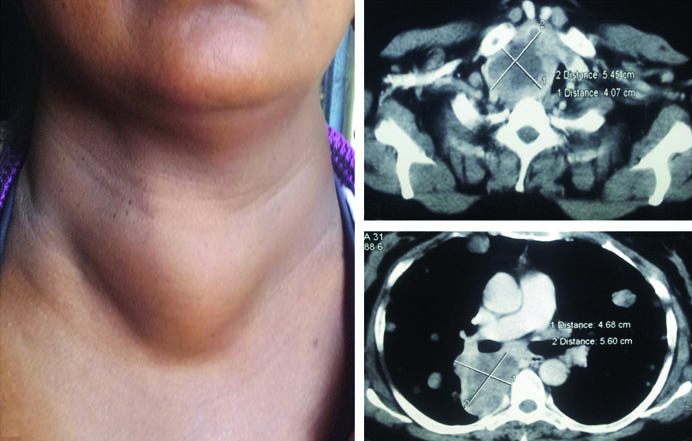
Well defined and large, rounded multiple shadows in lung fields on chest imaging are commonly caused by metastatic cancer and are called cannon ball shadows. A 46-year-old female presented to us with history of thyroid swelling for 10 years. She had been investigated four years back and was handed a diagnosis of colloid goitre. The swelling was neglected and she never underwent surgery. Her present problems were shortness of breath, dysphagia and retrosternal chest pain. Evaluation showed a hard goitre with retrosternal extension [Table/Fig-1]. Chest X-ray and contrast enhanced tomography scan of chest showed multiple cannon-ball lung shadows [Table/Fig-2]. Fine needle aspiration from thyroid nodule and from the lung lesions both showed follicular neoplasm of the thyroid. Patient was referred for total thyroidectomy followed by radioiodine therapy. Total thyroidectomy was done and the histopathology of the same confirmed the diagnosis of follicular carcinoma thyroid.
a) Clinical photograph showing swelling in the anterior aspect of neck; b) Contrast enhanced computed tomography scan section at T1 vertebral level showing mass arising from thyroid gland; c) Section at level of T4 vertebra showing extension of the mass into posterior mediastinum.
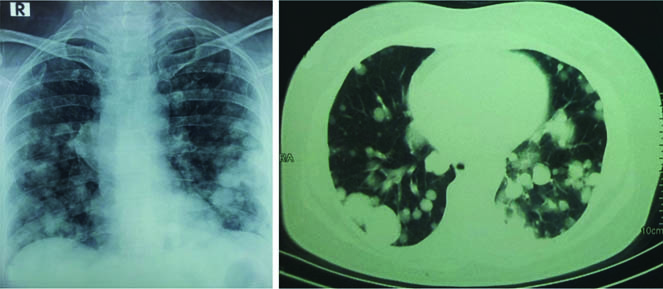
a) Chest roentgenogram showing multiple cannon ball shadows; b) Computed tomography scan of chest with lung window settings showing multiple nodules consistent with cannon ball metastases.
Cannon ball lung metastatses have been classically described with urogenital tract malignancies (renal cell carcinoma and gestational and non-gestational choriocarcinoma), gastrointestinal tumours and sarcomas [1]. Even though lung metastases can occur in follicular carcinoma of thyroid, cannon ball metastases from follicular carcinoma has not been reported. In general, presence of cannon ball metastases indicate advanced disease and portend poor prognosis [1,2]. However, cases have been reported where patients with such a presentation had good outcome [3]. This is possible when the tumour is chemosensitive or is amenable to ablative therapy as with thyroid malignancy using radioiodine.
Learning Points
Neglected colloid goitre can transform into follicular carcinoma and hence, a close follow up is essential if the patient is not being operated for goitre.
Follicular carcinoma of thyroid is a rare primary causing cannon ball metastases to lung.
If the tumour is sensitive to ablative therapy, patients with cannon ball lung metastasis can still have good survival.
[1]. Agarwal R, Mukhopadhyay J, Lahiri D, Biswas A, Maity P, Cannon-ball pulmonary metastases as a presenting feature of stomach cancerLung India 2015 32(3):300-02. [Google Scholar]
[2]. Chao CM, Lai CC, Cannon ball pulmonary metastasesQJM 2015 108(10):843 [Google Scholar]
[3]. Singh RK, Thangakunam B, Isaac B, Christopher DJ, Cannon ball shadow in the lungs and pulmonary embolism in a young manBMJ Case Rep 2013 2013(pii):bcr2012007541 [Google Scholar]