Achondroplasia with Polydactyly: A Case Report
Caroline Frank1, Sameeya Shariff2, Muddepalle Pavani3, Balasubramanian Karthika4, Sridhar Thathekalva5
1 Intern, Department of Oral Medicine and Radiology, Priyadarshini Dental College and Hospital, Tiruvallur, Tamil Nadu, India.
2 Intern, Department of Oral Medicine and Radiology, Priyadarshini Dental College and Hospital, Tiruvallur, Tamil Nadu, India.
3 Assistant Professor, Department of Oral Medicine and Radiology, Priyadarshini Dental College and Hospital, Tiruvallur, Tamil Nadu, India.
4 Associate Professor, Department of Oral Medicine and Radiology, Priyadarshini Dental College and Hospital, Tiruvallur, Tamil Nadu, India.
5 Professor, Department of Oral Medicine and Radiology, Priyadarshini Dental College and Hospital, Tiruvallur, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Caroline Frank, Department of Oral Medicine and Radiology, Priyadarshini Dental College, VGR, Pandur-631203, Tiruvallur, Tamil Nadu, India.
E-mail: drcarlynfrank@gmail.com
An eight-year-old girl child reported to the Department of Oral Medicine and Radiology with the chief complaint of unerupted permanent teeth for past two years. The child presented features like disproportionately short stature, rhizomelic shortening of arms and legs, long face, frontal bossing and saddle nose. Based on the findings of chest and spine radiographs and ultrasound the case was diagnosed as a rare bone disorder “Achondroplasia”. This case also presents a unique feature of polydactyly. Polydactyly is a manifestation in clinical medicine because it can serve as an indicator for a plethora of congenital anamolies. This case gained dental interest because of its characteristic craniofacial features. This article highlights the peculiar manifestations of this anamoly.
Delayed eruption, Dental caries, Short stature
Case Report
An eight-year-old Indian female child, born to 3rd degree consanguineous parents, reported to the Department of Oral Medicine and Radiology, Priyadarshini Dental College, Thiruvallur, Tamilnadu, with complaint of unerupted permanent teeth for the past two years.
Antenatal history revealed no history of fever, rashes, hypertension, diabetes or medications during pregnancy. Natal and post natal history revealed that patient was delivered via naturalis at 33 weeks and six days of gestation. Her birth weight was 2.5 kilograms. The child had a small patent foramen ovale and patent ductus arteriosus at birth which was found to be consistent with age.
Baby developed icterus on the third day of life and was kept under phototherapy in view of rising serum bilirubin levels. The level normalized slowly and was brought to anicterus state.
Chest, spine X-ray, ultrasonogram of brain, were taken after birth. X-ray suggested a probable diagnosis of short rib polydactyly syndrome. Ultrasonogram of brain showed normal features.
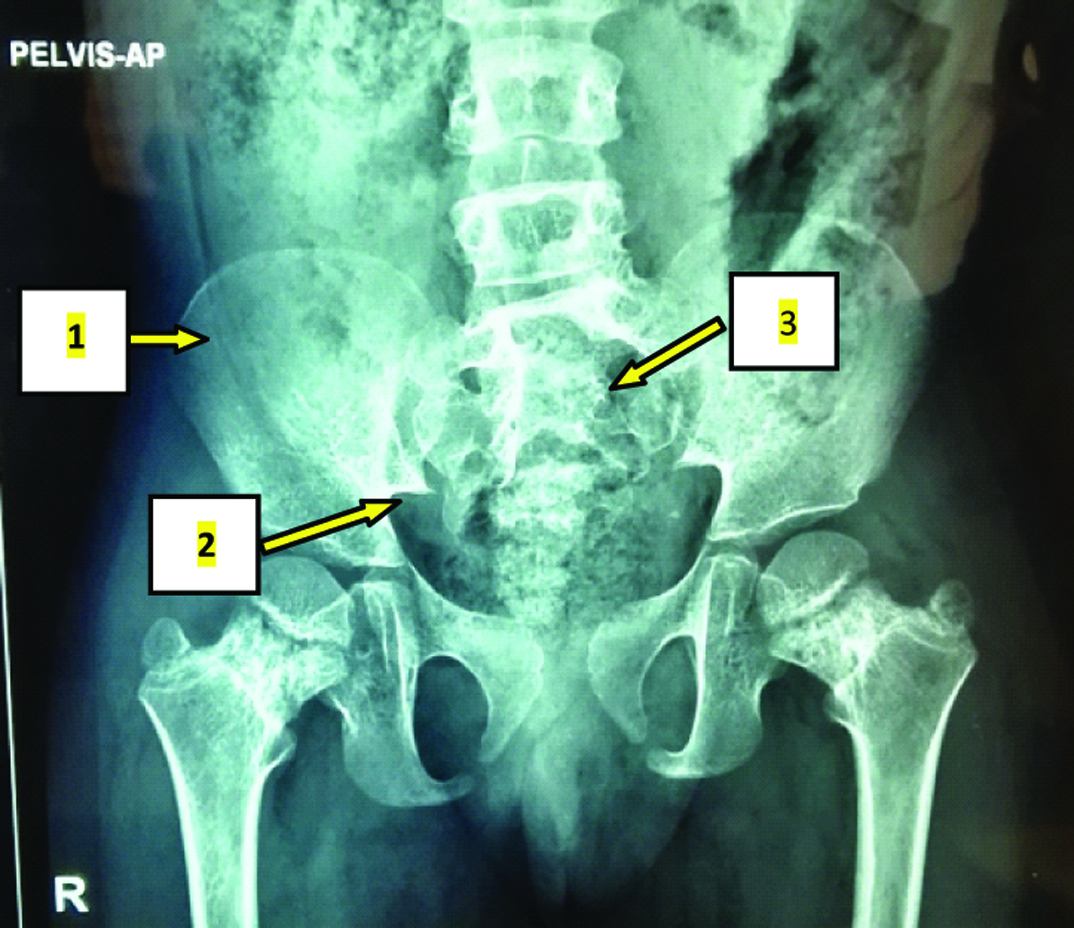
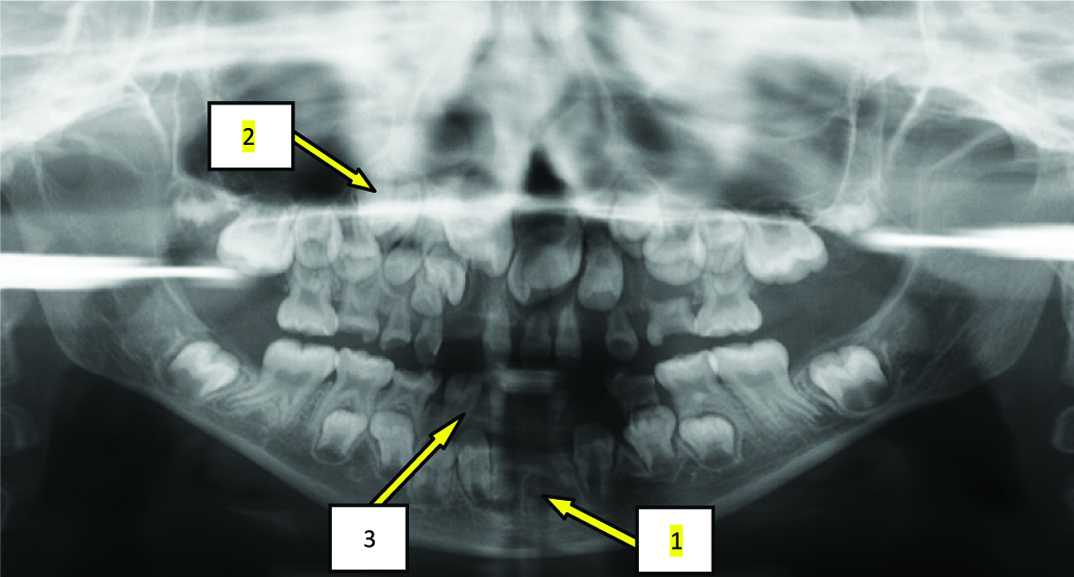
The cardinal features noted in this case were disproportionately short stature, rhizomelic shortening of the arms and legs [Table/Fig-1], thoracolumbar protuberance, lumbar lordosis [Table/Fig-2], limitations in joint movement, long face, frontal bossing, convex profile, midfacial hypoplasia, saddle nose [Table/Fig-3], trident hands [Table/Fig-4] and polydactyly [Table/Fig-4,5]. Short and round iliac bones, narrow greater sciatic notch (greater sciatic notch is a notch in the ilium, one of the bones that form the human pelvis) and decreased interpedicular distance from L1 to L5 were seen [Table/Fig-6]. Despite this mis-shapen appearance, the child had normal intelligence. On intraoral examination, generalized microdontia, congenitally missing permanent lower central incisors, left lateral incisor and supernumerary tooth in first quadrant in between canine and first premolar, fusion of primary lower right lateral incisor and canine [Table/Fig-7], and high frenal attachment were observed. Multiple teeth were found to be carious [Table/Fig-7].
Disproportionately short stature (110 cm, 3.6 feet), rhizomelic shortening of the arms and legs.

Thoracolumbar protuberance and lumbar lordosis.

Long face, frontal bossing, convex profile, midfacial hypoplasia, saddle nose.

Polydactyly and trident hands.


1) Short and round iliac bones; 2) Narrow greater sciatic notch and; 3) Decreased interpedicular distance from L1 to L5.
OPG showing: 1) Congenitally missing lower central incisors, left lateral incisor and; 2) Supernumerary tooth in first quadrant in between canine and first premolar; 3) Fusion of deciduous lower right lateral incisor and canine.
Discussion
Achondroplasia is a nonlethal form of chondrodysplasia and is the most prevalent form of skeletal dysplasia with characteristics of short limb dwarfism [1]. Prevalence in population is about 1:10,000 to 1: 50,000 [2]. It is an autosomal dominant disorder with complete penetrance [1]. A 90% of cases occur due to de novo mutations in the gene for Fibroblast Growth Factor Receptor-3 (FGFR-3) [3]. This causes decrease in endochondral ossification, inhibited proliferation of chondrocytes in growth plate cartilage, decreased cellular hypertrophy and decreased cartilage matrix production. Within the first few months of life, homozygous form is usually life threatening because of respiratory insufficiency caused by very severe rib cage deformity. In heterozygous state, the child is of normal life span and Intelligence Quotient (IQ) [4]. In this case, additional feature of polydactyly was present. Polydactyly results from defective patterning of anterior–posterior axis of the limb during development [5]. Clinical features and orofacial manifestations and dental management protocol is presented in [Table/Fig-8,9] [1–4,6].
Clinical features and orofacial manifestations of patients with achondroplasia.
| Clinical Features | Orofacial Manifestations |
|---|
Disproportionately short stature. Girls grow to a height of about 126 cm (4 ft 2 inch) and boys to a height of 131(4 ft 4 inch) [4].
| Macrocephaly, frontal bossing, midfacial hypoplasia, relative mandibular prognathism, flat nasal bridge [3].
|
Rhizomelic shortening of the arms and legs with trident configuration [6]. Polydactyly may be present.
| Retarded eruption of permanent teeth [2].
|
Thoracolumbar protuberance, lumbar lordosis, limitations at the elbow joint [1].
| Crowding, narrow maxilla leading to skeletal and dental Class III malocclusion and crossbite [2].
|
Short and round iliac bones, narrow greater sciatic notch and decreased interpedicular distance from L1 to L5 are seen [1].
| |
Normal intelligence [1].
| |
Dental management protocol.
| 1. Detailed case history should be taken. |
| 2. Special psychological behaviour management is mandatory [4]. |
| 3. Conductive hearing loss may be present [4]. Hearing aid should be adjusted to prevent amplification of sounds in dental operatory. |
| 4. Delayed eruption of permanent teeth may be seen [4]. Investigation is warranted to determine whether the teeth are missing or eruption is delayed. All children with this condition should be evaluated for orthodontic needs by five or six years as Class III malocclusion is of concern [8]. |
| 5. Shunt placed due to hydrocephalous causes difficulty in head control during dental treatment. Precaution should be taken before dental treatment to stabilize the head as there is a possibility of foramen magnum stenosis, limitation in neck extention which can lead to respiratory complication. Antibiotic prophylaxis before treatment becomes necessary [4]. |
| 6. It is advised to perform dental treatment under local anaesthesia, because general anaesthesia poses certain complications due to anteriorly placed epiglottis, small nasal pharynx and larynx, difficulty in intubation, lumbar lordosis, narrowing of spinal cord and small chest [7]. |
| 7. Based on the treatment needs of the patient, dental procedures can be carried out. |
Prenatal diagnosis of homozygous achondroplasia is possible at 10-12 weeks by mutation detection as compared to ultrasound examination which detects only by 16-20 weeks. DNA based methods on chorionic villi is used in prenatal diagnosis [3].
Differential diagnosis includes hypochondroplasia, thanatophoric dysplasia, and non syndromic craniosynostosis and crouzon’s disease with acanthosis nigricans [4]. Hypochondroplasia is distinguished by the presence of less severe radiographic features. Thanatophoric dysplasia is more severe and extremely lethal [7].
In this case, oral prophylaxis, restoration of the carious teeth and prosthetic rehabilitation of the congenitally missing permanent lower central incisors and left lateral incisor was planned. Patient was also motivated for regular follow up for the intervention and correction of anticipated malocclusion.
Achondroplastic children are at a high risk of persistent or recurrent otitis media which may lead to conductive hearing loss [8]. This may be linked to midface hypoplasia, shortened eustachian tubes, small pharynx, and relative enlargement of the tonsils and adenoids. Concurrence among clinicians is that this should be treated by adenotonsillectomy and insertion of ventilation tubes to prevent conductive hearing impairement. Medications are being developed to decrease the complications of this condition. C-Natriuretic Peptide (CNP) which is found to antagonize the downstream effects of the aberrant FGFR-3 signal is under Phase II clinical trials [6]. The parents of the child should be counselled to help the child to cope up with medical problems and confront the psychological behavior of the child.
Conclusion
This article reports the association of polydactyly with achondroplasia. There is no evidence of prevalence of dental caries with achondroplasia; however in this case, carious primary teeth were reported which may be attributed to poor oral hygiene. Studies on this aspect can provide a further insight on this subject.
[1]. Sethi RS, Kumar L, Chaurasiya OS, Gorakh R, Case report: AchondroplasiaCurr Pediatr Res 2011 15(2):137-40. [Google Scholar]
[2]. Chawla K, Lamban AK, Faraz F, Tandon S, Achondroplasia and periodontal diseaseJ Indian Soc Periodontol 2012 16:138-40. [Google Scholar]
[3]. Celenk P, Arici S, Celenk C, Oral findings in a typical case of achondroplasiaJ Int Med Res 2003 31:236-38. [Google Scholar]
[4]. Rohilla S, Kaushik S, Vinod VC, Tanwar R, Kumar M, Case report: Orofacial manifestations of AchondroplasiaEXCLI J 2012 11:538-42. [Google Scholar]
[5]. Leslie Biesecker G, Polydactyly: How many disorders and how many genes: 2010 updateDev Dyn 2012 240(5):931-942. [Google Scholar]
[6]. Ireland PJ, Pacey V, Zankl A, Edwards P, Johnston LM, Savarirayan R, Optimal management of complications associated with achondroplasiaAppl Clin Genet 2014 7:117-25. [Google Scholar]
[7]. Al-Saleem A, Al-Jobair A, Achondroplasia: Craniofacial manifestations and considerations in dental managementSaudi Dent J 2010 22:195-99. [Google Scholar]
[8]. Hunter AGW, Bankier A, Rogers JG, Sillence D, Scott Jr CI, Medical complications of achondroplasia: A multicentre patient reviewJ Med Genet 1998 35(9):705-12. [Google Scholar]