Extramedullary Haematopoiesis Presenting as an Adrenal Mass
Subramanian Kannan1, Prashant Kulkarni2, Akhila Lakshmikantha3, Karthik Gadabanahalli4
1 Consultant, Department of Endocrinology, Diabetes and Metabolism, Narayana Health City, Bengaluru, Karanataka, India.
2 Consultant, Department of Urology, Narayana Health City, Bengaluru, Karnataka, India.
3 Consultant, Department of Pathology, Narayana Health City, Bengaluru, Karanataka, India.
4 Consultant, Department of Radiology, Narayana Health City, Bengaluru, Karanataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Subramanian Kannan, 258/A Bommasandra Industrial Area, Hosur Road, Bengaluru-560099, Karanataka, India.
E-mail: subramanian.kannan@gmail.com
Adrenalectomy, Biopsy, Haemoglobinopathy
A 21-year-old female presented with right upper quadrant abdominal pain for duration of a week with intermittent nausea and low grade fever. She was evaluated in a local hospital where, Ultrasonography (USG) revealed a large right adrenal mass. Computed Tomography (CT) examination demonstrated an 8 cm x 7 cm heterogenous right adrenal mass which showed uneven contrast enhancement and a moderate mass effect with the inferior displacement and deformity of the right kidney. There is no evidence of invasion of the renal vein or inferior vena cava [Table/Fig-1]. The mass was well defined, heterogenous with hypodense areas and showed minimal enhancement with contrast. The left adrenal gland was normal.
Post-contrast CT scan (saggital) shows a heterogeneous well defined right adrenal mass with minimal contrast enhancement displacing the right kidney inferiorly (arrow). Also noted is a normal left adrenal gland (circle) and splenomegaly (star).

She was referred to us for right adrenalectomy. On evaluation, her original abdominal symptoms had subsided. She did not have any spells or syncopal events and her blood pressure and previous potassium levels all were normal. On examination, she was pale and icteric. Her blood pressure was normal at 110/70 mmHg. Her liver was palpable 2 cm below the right costal margin and her spleen tip was palpable. Her Haemoglobin (Hb) was 5.3 gm/dl and MCV was 59 fl. Rest of the blood counts were normal. Haemoglobin electrophoresis revealed a double heterozygous HbE-Thalassaemia (HbE: 72%; HbF: 15%; HbA2: 7.7%). Twenty four hour urine metanephrines and catecholamines were normal.
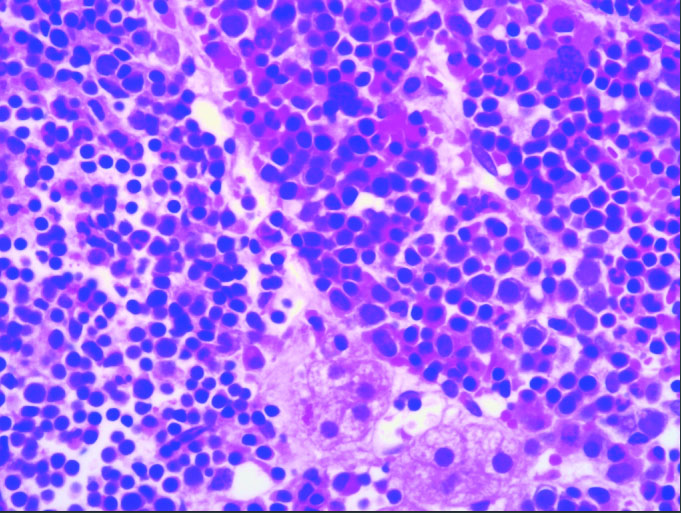
CT guided biopsy of the adrenal mass was undertaken. The histopathology showed adrenocortical tissue along with haematopoietic elements, mostly erythroid precursors in various stages of maturation with a few myeloid and megakaryocytic lineage cells [Table/Fig-2] and no adipose tissue consistent with a final diagnosis of adrenal extra-medullary haematopoiesis. She is being managed conservatively with blood transfusions and hydroxyurea and we plan to repeat imaging in six months.
H&E stain at magnification (40X) shows adrenocortical tissue along with haematopoietic elements. It mostly shows erythroid precursors in various stages of maturation. Also seen are a few myeloid and megakaryocytic lineage cells. No adipose tissue is seen. This was consistent with a diagnosis of extra-medullary haematopoiesis.
The spleen and liver are the primary sites for Extramedullary Haematopoiesis (EMH); however, other tissues and organs like the adrenal gland, lymph nodes, heart, mediastinum, lung, breast, kidneys, skin, spinal and para-spinal regions, thyroid, gastrointestinal tract and endometrium may also be involved. The factors leading to EMH include abnormal release of marrow precursors into distorted bone marrow sinusoids and then into the circulation, differentiation of pleuripotent stem cells to haematopoietic stem cells forming bone marrow elements [1]. There are published reports of incidentally detected adrenal masses in patients with haematological disorders including thalassaemia, hereditary spherocytosis, myeloid metaplasia [2]. While in a few cases adrenalectomy resulted in the histological surprise of EMH, in the others pre-operative CT/USG guided biopsy resulted in diagnosis of adrenal EMH and authors chose conservative management [3]. Adrenal EMH should included in the differentials of adrenal masses particularly in those with haemoglobinopathies or marrow disorders.
[1]. O’Keane JC, Wolf BC, Neiman RS, The pathogenesis of splenic extramedullary haematopoiesis in metastatic carcinomaCancer 1989 63(8):1539 [Google Scholar]
[2]. Sekar S, Burad D, Abraham A, Paul MJ, Adrenal incidentaloma caused by extramedullary haematopoiesis: conservative management is optimalBMJ Case Rep 2015 2015:piibcr2015211014 [Google Scholar]
[3]. Al-Thani H, Al-Sulaiti M, El-Mabrok G, Tabeb A, El-Menyar A, Adrenal extramedullary haematopoiesis associated with beta-thalassaemia trait in an adult woman: a case report and review of literatureInt J Surg Case Rep 2016 24:83-87. [Google Scholar]