When ascertaining the manner of death, the forensic pathologist should be careful, because in some instances, attempts are made by the criminals to conceal homicides as suicides. The case under discussion highlights the contribution of the forensic pathologist in the ascertainment of the manner in firearm deaths.
The deceased was a poacher and his dead body was found in a cashew land with his shotgun lying over him. The shirt had a roughly circular defect with muzzle mark, and burnt and blackened margin. Beneath that, on front of the left upper chest a 2cm diameter circular, perforated laceration, with muzzle imprint and, burnt and blackened margin was found. Shelving was found at the upper margin. Chest X-ray showed the downward pellet distribution. Cause of death was chest injuries due to pellets discharged from a smooth bore weapon. Length of the upper arm reach was 65cm (25 inches) and the length from the muzzle to the trigger was 79cm (31 inches).
In conclusion, it was found to be a fabricated suicide scene and the manner of death was ascertained as homicide. This reiterates that the postmortem investigation of firearm deaths should be performed or conducted under direct supervision of forensic specialist to deliver justice.
Case Report
The deceased was a poacher and he worked for an ex-police officer, guarding his land of cashew and paddy. He lived in a house located in the above mentioned land. A day before his death, his mother received several calls from him stating that, he had shot down an elephant to obtain tusks and now he is afraid that he would be caught by police. Further, at night, he had told his mother that he shot himself ones but failed and by next trigger he would kill himself. People believed that, he might have been disturbed by those incidents and killed himself.
Next day evening, by 3:00 pm his dead body was found in the same land with his shotgun lying over him. Near dead body there was a cellular phone, a lighting torch, an empty cartridge, and a live cartridge [Table/Fig-1]. A carcass of an elephant with two-day-old putrefaction was also found about 300 m away from the body but the tusks were intact.

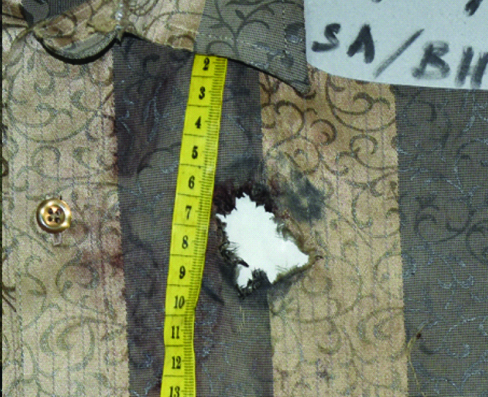
Autopsy revealed an average built, nourished body. He was clad in stripped short sleeved cotton-nylon shirt with a roughly circular about 3cm x 2cm defect with burnt and blackened margin, on the left upper chest area. Around the fabric defect, a faint mark of the muzzle was found [Table/Fig-2].
Tear of the shirt with burnt and blackened margin with faint muzzle imprint.
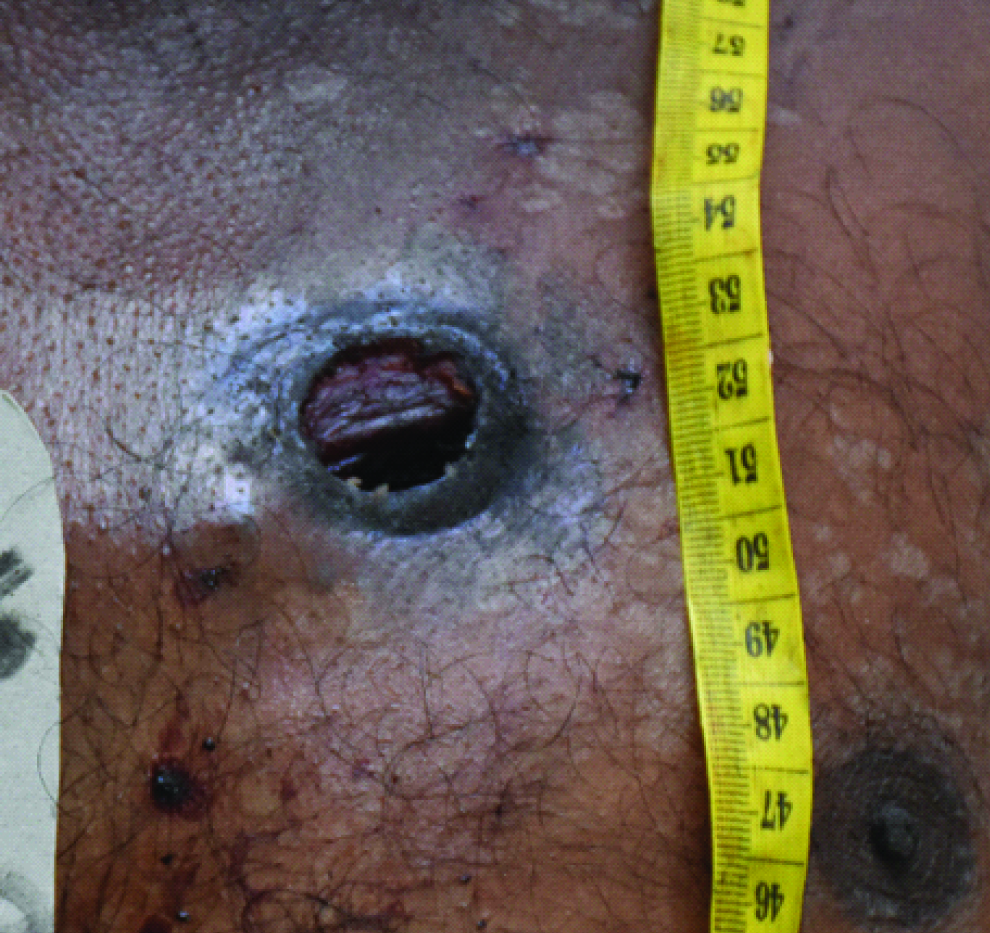
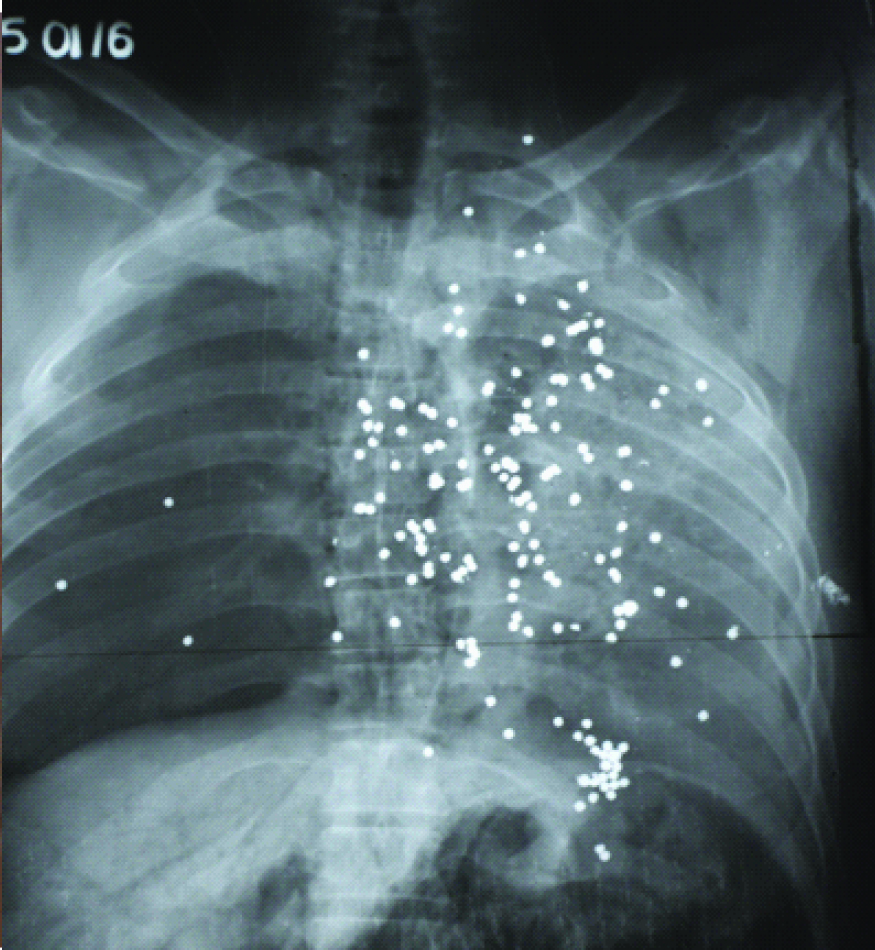
External examination showed an underlying 2 cm diameter circular shaped, perforated laceration, on the front aspect the left upper chest. The center was 6cm below the clavicle, 3 cm to the midline and 134 cm from heel. It was associated with burnt and blackened margin and surrounded by a 0.5 cm circumscribed muzzle imprint. Shelving was found at the upper margin and under cutting was at the lower margin. Blood dripped vertically downwards [Table/Fig-3]. The perforation entered in to the left chest cavity between 2nd and 3rd ribs fracturing the 3rd rib close to the costo-chondral junction. The pellets entered the left chest cavity in downwards and backwards lacerating the arch of aorta, both left and right atria, and fracturing the 4th to 7th ribs at the back of the chest cavity. Wad was recovered from left lung. Chest X-ray, which was taken before the autopsy showed downward distribution of pellets [Table/Fig-4].
Entry wound with verticle blood drips.
Chest X-ray showed downward distribution of pellets.
Postmortem ant bites, 0.5cm x 0.5cm in size were found on the medial aspect of the right arm and 10cm x 1cm on the back of the right upper leg. Neck was free of injuries.
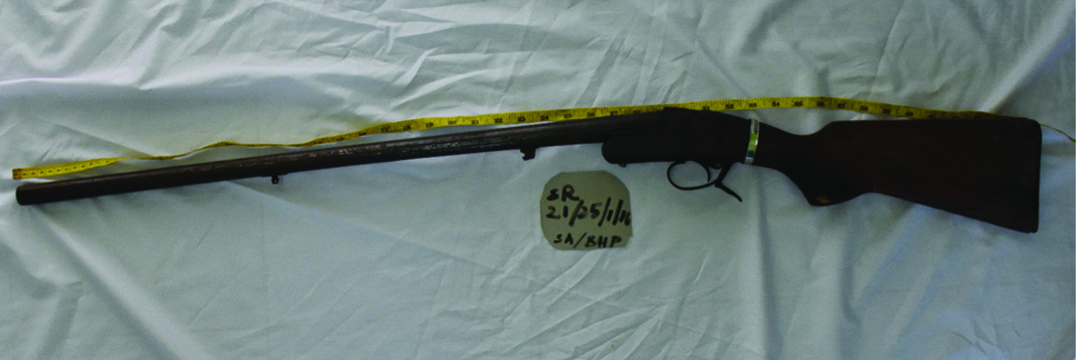
The upper arm reach from the base of the neck to the tip of the middle finger was 65 cm (25 inches) [Table/Fig-5] and the length from the muzzle to the trigger of the weapon was 79 cm (31 inches) [Table/Fig-6]. The diameter of the muzzle end was 2.5 cm. Finally, the cause of death was given as chest injuries due to pellets discharged from a smooth bore weapon.
The upper arm reach was 25 inches (65cm).

Muzzle to trigger length was 31 inches (79cm).
Discussion
Manner of deaths due to firearms can be accidental, suicidal or homicidal. Accidental firearms deaths are rare and are usually due to careless handling of the weapon [1]. But suicidal and homicidal firearm deaths are not uncommon. When ascertaining the manner of death, the forensic pathologist should be careful, because in some instances, attempts are made by the criminals to conceal homicides as suicidal deaths. In forensic practice, fabrication of circumstances of fatal events is not uncommon [2]. Therefore, complete postmortem investigation including sufficient history, complete scene visit, meticulous autopsy, and ancillary investigations should be performed. The forensic pathologist must have instincts to identify fabricated scenes made by smooth operators. The case under discussion highlights the contribution of the forensic pathologist in the ascertainment of the manner in firearm deaths.
The victim was a poacher possessing a smooth bore firearm. In the literature, it was discussed whether there is an association between possessing a firearm and suicide, but existing studies have failed to account for that possibility [3].
Presence of the firearm at the scene usually suggests suicide. Without the immediate collection of evidence at the scene, the objective re-construction of the event becomes impossible [4].
Muzzle imprint marks are formed on the clothes when perforated by fire [5]. In this case also there was a faint muzzle imprint on the clothes. When the muzzle is in contact with a clothed part of the body, ring mark is caused by the heated muzzle of the barrel. Along the margin of the defect, the fibers are blackened by gun smoke and in synthetic clothes, such as cotton-nylon shirt found in this case; the edges are burnt and melted. Soot was not deposited around the bullet hole and that depends on how tight the gun was held against the body [4].
There was only one entry wound but there were no exit wounds. Shotgun pellets exit in head or thin parts, but at other places usually do not exit even with contact or close range fires [6].
When deciding the range of fire, several factors should be considered. The contact wounds will not usually demonstrate features of ‘secondary projectiles’ on the external side of the body such as wad marks, injuries due to metal fragments of the cartridge case, burns due to flame, soot, tattooing and discolouration due to combustion gases, unless there is loose contact. In the current case, in the absence of secondary projectile injuries on the outer side suggests a contact entry wound. Further, there was a circumscribed muzzle imprint. The presence of muzzle imprint is generally accepted as a sign of a contact shot [5]. In shot gun contact entry wounds, except on head, the diameter is equal to the barrel [1] and in this case, the diameter of the muzzle and the entry wound was equal. Therefore, the range of the fire was ascertained as contact.
Patterned muzzled imprint marks can provide clues to the type of the firearm [5]. In this case, the shape and size (2.5cm diameter) of the muzzle imprint was compatible with the muzzle end of the smooth bore weapon.
The period of survival after shotgun wound depends mainly upon the range of fire. Contact or close range injuries usually result in massive destruction, and the wounds involving the head or thorax result in instantaneous or rapid death [1]. Therefore, in this case, with lacerated arch or aorta and heart an instantaneous or rapid death is expected.
Victims of suicides usually pull the clothes aside to bare the skin before shooting themselves [6]. But in this case, the clothes seem to be not moved at all. It aroused the suspicion as to the manner of death.
When considered the entry wound, the presence of shelving in the upper margin and the undercutting in the lower margin indicates that the direction of fire within the body [7] is downward and backwards. It was further confirmed by the distribution of pellets in the postmortem chest-X-ray.
When suicide deaths due to firearms are concerned, for the identification of the shooter, an integral medico-legal assessment of all the facts including the autopsy findings and the investigation results is essential. However, the morphological findings alone do not allow safe diagnosis. To ascertain manner as suicide, not only autopsy features but also ascertaining gunshot residues are important for the doubtless identification of the shooter for confirming the suicide [4]. Those morphological features are the site of entry, close or contact range and accessible path of the fire. In this case, the selection of an elective site and the contact range, suggest suicide, but the downward direction of fire was inaccessible without improvisation and is unexpected in suicide. Rather than holding the weapon upwards, the proximity of the weapon to the body is also a good marker of suicide [8].
But in this case, the trigger of the weapon should be held above the victim’s head to achieve the downward direction of the fire. In such situation, we should see whether this person could operate this trigger by himself at this posture. It was found that, the upper arm reach from base of the neck to the tip of the middle finger was 65cm (25 inches) was much shorter than the length from the muzzle to the trigger of the weapon, which was 79cm (31 inches). In some suicides, fabricated gunshot devices are used [9]. However, an improvised apparatus was not found at the scene for triggering the gun in a downward and backward direction. Usually, in suicides, triggering is done by the feet and the weapon is kept close to the body and the direction of the fire is upwards. But in this case, the fire directed downwards and it is impossible to operate the trigger of this smooth bore weapon obviously from legs or even by the hands. Therefore, self-infliction is impossible.
Conclusion
It was found to be a fabricated suicide scene and the manner of death was ascertained as homicide. This reiterates that the postmortem investigation of firearm deaths should be performed or done under direct supervision of a forensic specialist to deliver justice.
[1]. Werner US, Daniel JS, Spits and Fisher’s Medico-legal investigation of death 2006 4th edSpringfieldCharles C ThomasInjury by gunfire. In: Spitz WU; Pp. 607-746 [Google Scholar]
[2]. Hiss J, Kahana T, Fabricated homicides in Israel in light of the IntifadaJ Clin Forensic Med 1995 2(4):189-93. [Google Scholar]
[3]. Miller M, Swanson SA, Azrael D, Are we missing something pertinent? A bias analysis of unmeasured confounding in the firearm-suicide literatureEpidemiol Rev 2016 38(1):62-69. [Google Scholar]
[4]. Padosch SA, Schmidt PH, Schyma C, Hirsch RD, Kröner LU, Dettmeyer RB, Medicolegal aspects of witnessed suicide due to gunshot to the head. II. Legal medicine aspects and examination of the firing handArch Kriminol 2004 214(5-6):149-62. [Google Scholar]
[5]. Geserick G, Vendura K, Wirth I, Werkgartner’s muzzle imprints mark-a literature studyArch Kriminol 2009 224(5-6):145-57. [Google Scholar]
[6]. Rao D. Firearm injuries in Forensic pathology, e-book. Available from: http://www.forensicpathology online.com/E-Book/injuries/firearm-injuries [Google Scholar]
[7]. Saukko PJ, Knight B, Knight’s forensic pathology 2015 4th edLondonCRC press [Google Scholar]
[8]. Mason JK, Purdue BN, The pathology of trauma 2000 3rd edLondonArnoldSmooth bore firearm injuries. In: Cassidy M; Pp. 61-74 [Google Scholar]
[9]. Karger B, Teige K, Brinkmann B, 2 suicides with self-fabricated gunshot devices: technical forensic and morphologic ballistic characteristicsArch Kriminol 1995 195(5-6):147-52. [Google Scholar]