Type 2 DM and its associated secondary complications are rapidly becoming the world’s most significant cause of morbidity and mortality [1–3]. DM is basically a metabolic disorder characterized by hyperglycaemia and insufficiency of secretion or action of endogenous insulin [1,2]. Although the aetiology of DM is not fully defined but environmental factors have been implicated [3]. Exogenous insulin and other medications are effective to control many aspects of DM and its associated complications, but still not fully defined, particularly DMN. DMN is a very common heterogeneous disorder associated with a wide range of abnormalities such as severe pain, disability and accounts for the majority of non-traumatic lower extremity deletions [4,5]. DMN may also affect sympathetic or parasympathetic function with serious consequences such as sudden cardiac death and silent myocardial ischemia [5]. In spite of the availability of modern scientific approaches and persisting investigative efforts, a feasible treatment for human type 2 DM and its associated DMN are not available. Therefore, understanding their pathogenesis is critical for a better management of these metabolic disorders.
Oxidative stress plays a central role in the onset of DM as well as its associated complications [5,6]. Various studies have shown that, DM is associated with increased formation of Reactive Oxygen Species (ROS) or Reactive Nitrogen Species (RNS) and decrease in anti-oxidant potential [5–7]. Over-production of ROS and RNS has the ability, either directly or indirectly, to damage proteins, DNA and other cell biomolecules. In fact proteins are their major targets, protein oxidation which results in functional disruption. Number of studies indicates a strong role for increased in protein oxidation as a primary cause of cellular dysfunction observed in many disorders [8]. Abnormal functioning of a wide array of enzyme activities have been reported [9]. Alterations of structural protein can also lead to loss of function [8–11]. Oxidatively modified low density lipoproteins may play a significant role in the aetiology of atherosclerosis [12]. High levels of advanced oxidative-by-products of protein have been linked in the pathogenesis of chronic rheumatic valve disease [13]. These disorders could be due to the abnormal protein aggregates formation due to ROS and RNS induced damage. In DM patients, it is reported that hyperglycaemia can promote ROS and RNS accumulation through different metabolic pathways which increase formation of Advanced Glycation End products (AGEs) [14,15]. Protein glycation in DM patients is basically an end product of glucose auto-oxidation, which is a process initiated mainly by ROS and RNS [15,16]. Over availability of glucose promotes enhanced production of AGEs, these auto-oxidative glycosylation processes are probably the major cause of increased ROS and RNS production in DM patients [15–17]. Importantly, the formation of AGEs primarily leads biomolecular oxidation which further promotes irreversible tissue damage, including the damage of peripheral nerve and vessel wall [4,5]. Research over the last decade suggests that, ROS and RNS plays a role in neuronal pathways as a link between hyperglycaemia and the observed pathophysiological features of DM, associated with the onset and progression of DM late complications, including neuropathy [5,15–17]. Despite of these available knowledge, DM or DMN remains an enigmatic disorders and the agent (or agents) triggering these metabolic response remains to be fully identified. Patients with DM or DMN have a diverse array of ROS and RNS response, but the molecular and cellular mechanisms that are responsible for the production of ROS and RNS in these disorders and the ways through which ROS and RNS contribute in tissue destruction remain highly controversial.
In view of these, we hypothesized that, overproduction of ROS and RNS in DM or DMN leads to a variety of ROS and RNS-mediated modifications of the endogenous proteins, such as increased formation of protein oxidative marker carbonyl contents, which thus, leads to oxidative stress in these patients. To assess this hypothesis and establish a link between protein oxidation and DM or DMN, we examined the levels of biochemical marker of protein oxidation in the sera of type 2 DM and its associated DMN patients, and analysed their relationship to the disease activity biomarkers such as glycosylated haemoglobin, disease duration and patients’ ages. Our results not only support an association between protein oxidation and diabetes or diabetes neuropathy, but also suggest that, protein carbonylation may be important in the evaluation of DM or DMN progression and in the elucidation of the mechanisms of these disorders pathogenesis.
Materials and Methods
This retrospective study has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for human samples and has been approved by the regional Ethical Committee of Ministry of Health (Approval # MERC 45/44/1320). The study group included 42 diabetes mellitus type 2 patients (19 male and 23 female), 37 diabetes neuropathy patients (18 male and 19 female). The control group comprised 21 healthy human subjects (11 male and 10 female). The mean ages of all studied patients and healthy controls were not significantly different between the groups (p>0.05). The average (±SD) of post prandial blood sugar level for 42 diabetes patients and 37 diabetes neuropathy patients were 334±79 mg/dl and 342±44 mg/dl, respectively, while for 21 healthy subjects it was 110±8.3 mg/dl. The average (±SD) glycosylated haemoglobin (HbA1C) for diabetes and diabetes neuropathy patients was 8.0±1.9 and 8.5±0.91 respectively, whereas, for healthy subjects it was 4.7±0.42. Diabetic neuropathy was assessed by physical examination and nerve conduction studies. The clinical characteristics of the subjects recruited are summarized in [Table/Fig-1]. Venous blood from all subjects was collected, sera were separated and stored in small aliquots at -20°C until analysed.
Clinical characteristics of diabetes patients.
| Parameters | DM patients | DMN patients | Healthy controls |
|---|
| n | 42 | 37 | 21 |
| Sex (M/F) | 19M/23F | 18M/19F | 11M/10F |
| Age (years) | 46±23* | 49±27* | 45±22 |
| Blood glucose (mg/dl) | 334±79§ | 342±44§ | 110±8.3 |
| HbA1C | 8.0±1.9† | 8.5±0.91† | 4.7±0.42 |
| Disease duration (years) | 10.8±7.1 | 11.3±6.5 | - |
Abbreviations: DM, Diabetes Mellitus; DMN, Diabetes Mellitus Neuropathy; n, number of serum samples tested; HbA1C, Glycosylated Haemoglobin. *p>0.05 versus age of healthy controls; §p<0.001 versus blood glucose of healthy controls; †p<0.001 versus HbA1C of healthy controls.
Assay of protein oxidation: Protein oxidation in the serum samples of all studied subjects were estimated by protein carbonyl contents using Protein Carbonyls Colorimetric Assay Kits (catalog # 10005020; Cayman Chemical, Ann Arbor, MI, USA) according to the manufacturers’ instructions using 2, 4-dinitrophenylhydrazine (DNPH). The carbonyl contents using a molar absorption coefficient of 22,000 M−1cm1 and were expressed in nmol/mg protein as described previously [18,19].
Isolation of albumin from diabetes patients and fluorescence measurements: Human Serum Albumin (HSA) was isolated from patients and also from healthy human subjects by ammonium sulphate fractionation followed by gel exclusion chromatography on Sephacryl S-200 HR column as previously described [20]. Isolated protein samples were then subjected for fluorescence measurements by exciting the protein samples at 285 or 280 nm and intrinsic fluorescence intensities were recorded using Anthos Zenyth 3100 Multimode Detectors (Salzburg, Austria) as described previously [21].
Statistical Analysis
All measurements were performed in duplicates using age-matched patients and control samples. Comparisons were performed by Graph Pad Prism-5 (San Diego, CA, USA) using one-way ANOVA followed by Tukey’s post-hoc analysis. The p-values less than 0.05 were considered significant, and p-values less than 0.001 were considered highly significant. Values shown are mean±SD unless stated otherwise.
Results
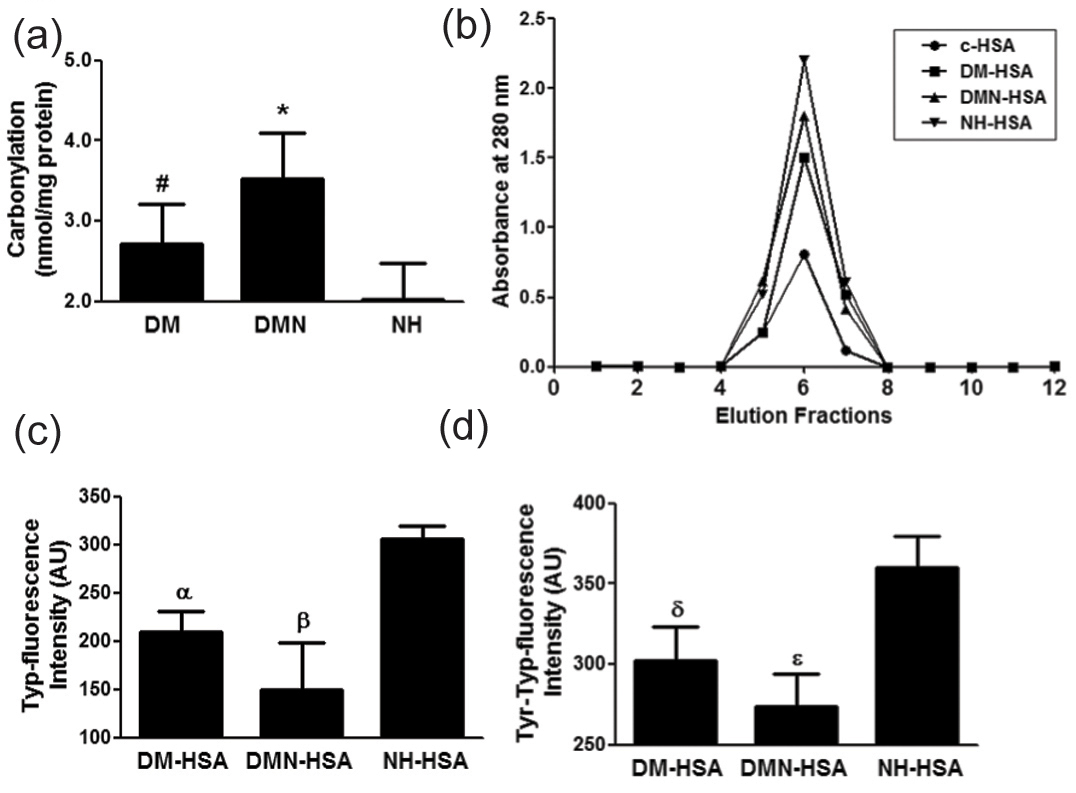
Protein oxidation in patients with diabetes and diabetes associated neuropathy: Protein oxidation characteristically results in an increase in carbonyl contents, therefore, increase in protein carbonylation is considered to be a most reliable biomarker of protein oxidation [18,22]. Results showed significant increase in serum protein carbonyl contents in 42 diabetes mellitus patients compared with 21 normal human subjects (p<0.01). The average carbonyl contents (±SD) in studied subjects of DM serum proteins and Normal Human (NH) proteins were 2.72±0.49 and 2.02±0.46 nmol/mg proteins, respectively [Table/Fig-2a]. Importantly, we have also determined the role of protein carbonylation in patients with diabetic neuropathy. Our novel data showed that, protein carbonyl content was significantly higher in diabetes neuropathy patients compared with non-DMN patients (p<0.05). The average protein carbonyl contents (±SD) in the sera with DMN (n=37) and DM (n=42) patients were 3.52±0.50 and 2.72±0.49 nmol/ml, respectively [Table/Fig-2a]. These oxidative serum proteins modifications were validated by fluorescence studies using most abundant serum protein HSA. For that HSA was isolated from 7 most active diabetes patients (DM-HSA) and from 7 most active DMN patients (DMN-HSA) and also from 7 normal healthy subjects (NH-HSA) by ammonium sulphate fractionation followed by gel exclusion chromatography. The purified HSA was found to elute in a single symmetrical peak using Sephacryl S-200 HR column [Table/Fig-2b]. The oxidative-induced alterations in tryptophan residue of DM-HSA, DMN-HSA and NH-HSA were studied by tryptophan intrinsic fluorescence using excitation wavelengths of 285 nm and 280 nm. Our novel data showed that, oxidation of tryptophan residue of DM-HSA or DMN-HSA was evident by the significant loss of intrinsic fluorescence intensity compared with NH-HSA, when the protein was excited at 285 nm (p<0.05). The average tryptophan-fluorescence intensity (±SD) of seven independent assays of DM-HSA, DMN-HSA and NH-HSA were 210±20.6, 150±48.8 and 305.7±13.5 AU, respectively [Table/Fig-2c]. Importantly, a p-value of 0.05 indicates significant difference in the tryptophan-fluorescence intensity of DM-HSA and DMN-HSA. Moreover, we further confirmed this oxidative protein by tyrosine-tryptophan fluorescence intensity. The average tyrosine-tryptophan fluorescence intensity (±SD) of seven independent assays of DM-HSA, DMN-HSA and NH-HSA were 302.5±20.7, 274±20.2 and 360±19.6 AU, respectively [Table/Fig-2d]. The results were similar to those obtained with tryptophan-fluorescence measurements. Data indicate that serum protein oxidation in diabetic neuropathy patients was significantly higher compared with non-neuropathic diabetes patients.
Protein oxidation in patients with Diabetes Mellitus (DM) and Diabetes Mellitus Neuropathy (DMN). (a) Levels of protein carbonyl contents in the sera of DM patients (n=42), DMN patients (n=37) and in Normal Human sera (NH, n=21). #p<0.01 versus NH; #p<0.05 versus DMN; *p<0.0001 versus NH. (b) Purification of Human Serum Albumin (HSA) from patients and NH subjects. Elution profiles of purified HSA from DM patients (DM-HSA), DMN patients (DMN-HSA) and Normal Humans Subjects (NH-HSA) on Sephacryl S-200 HR column. Commercial HSA (c-HSA) was also eluted from the same column and was used as a marker. (c) Tryptophan fluorescence (Typ-fluorescence) measurements in DM-HSA (n=7), DMN-HSA (n=7) and in NH-HSA (n=7). Protein was excited at 285 nm. αp<0.001 versus NH; βp<0.05 versus DMN; βp<0.001 versus NH. (d) Tyrosine-Tryptophan fluorescence (Tyr-Typ-fluorescence) measurements in DM-HSA (n=7), DMN-HSA (n=7) and in NH-HSA (n=7). Protein was excited at 280 nm. δp<0.01 versus NH; εp<0.05 versus DMN; εp<0.001 versus NH. Comparison analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test.
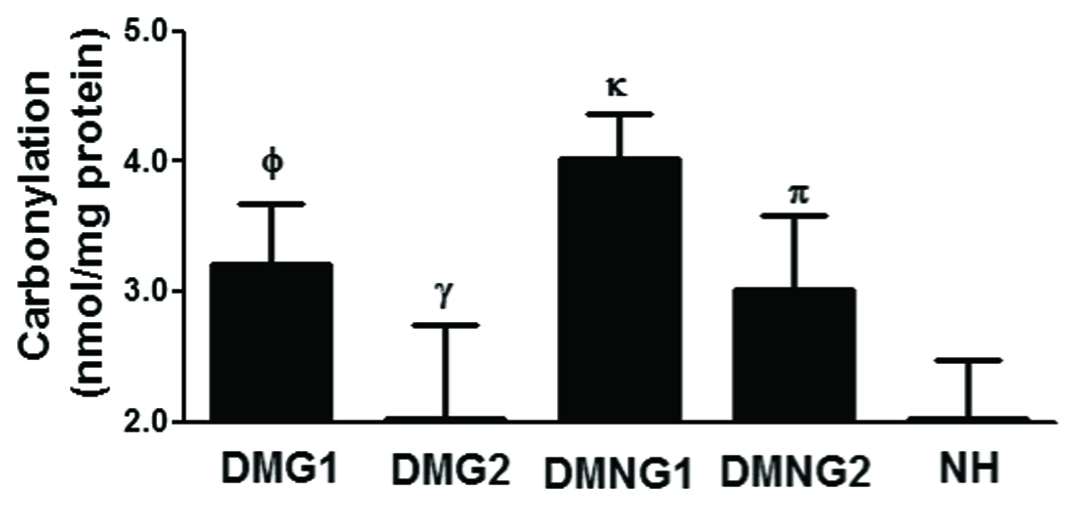
Glycosylated haemoglobin (HbA1C) - related increased of protein oxidation in patients with diabetes and diabetes associated neuropathy: To validate our central hypothesis, we assessed the increase in protein oxidation by HbA1C as a function of the diabetes activity index. For that protein carbonyl contents were estimated in accordance with the following patients groups: Diabetes patients group 1 (DMG1; HbA1C ≥8.8; n=20), diabetes patients group 2 (DMG2; HbA1C <8.8; n=22), diabetes neuropathy patients group 1 (DMNG1; HbA1C ≥8.8; n=18), diabetes neuropathy patients group 2 (DMNG2; HbA1C <8.8; n=19) and also in normal humans (NH; HbA1C <4.7; n=21). The average carbonyl contents (±SD) in the patients’ sera with DMG1, DMG2, DMNG1, DMNG2 and NH were 3.21±0.47, 2.23±0.53, 3.91±0.45, 3.10±0.67 and 2.02±0.46 nmol/mg protein, respectively. As evident in [Table/Fig-3], levels of carbonyl contents in all of the diabetes patients (both those with HbA1C levels ≥8.8 and those with HbA1C levels <8.8) were significantly higher in comparison with healthy controls (p<0.001). Interestingly, levels of carbonyl contents in diabetic neuropathy patients groups (both in those with HbA1C levels≥8.8 and in those with HbA1C levels<8.8) were significantly higher than diabetes patients groups of similar HbA1C levels, respectively (p<0.05). Remarkably, increase in levels of protein carbonyl contents in patients groups (both diabetes neuropathy and diabetes) with HbA1C levels≥8.8 were greater in comparison with those in patients with HbA1C levels<8.8, suggesting a positive association between the protein oxidation and HbA1C levels.
Glycosylated haemoglobin (HbA1C)-related increased of protein oxidation in patients with Diabetes Mellitus (DM) and Diabetes Mellitus Neuropathy (DMN). Levels of protein carbonyl contents in the serum samples of patients with DM group 1 (DMG1; HbA1C ≥8.8), DM group 2 (DMG2; HbA1C <8.8), DMN group 1 (DMNG1; HbA1C ≥8.8), DMN group 2 (DMNG2; HbA1C <8.8) and Normal Humans (NH). Φp<0.01 versus NH; Φp<0.05 versus γ; κp<0.05 versus π; κp<0.001 versus NH. Comparison analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test.
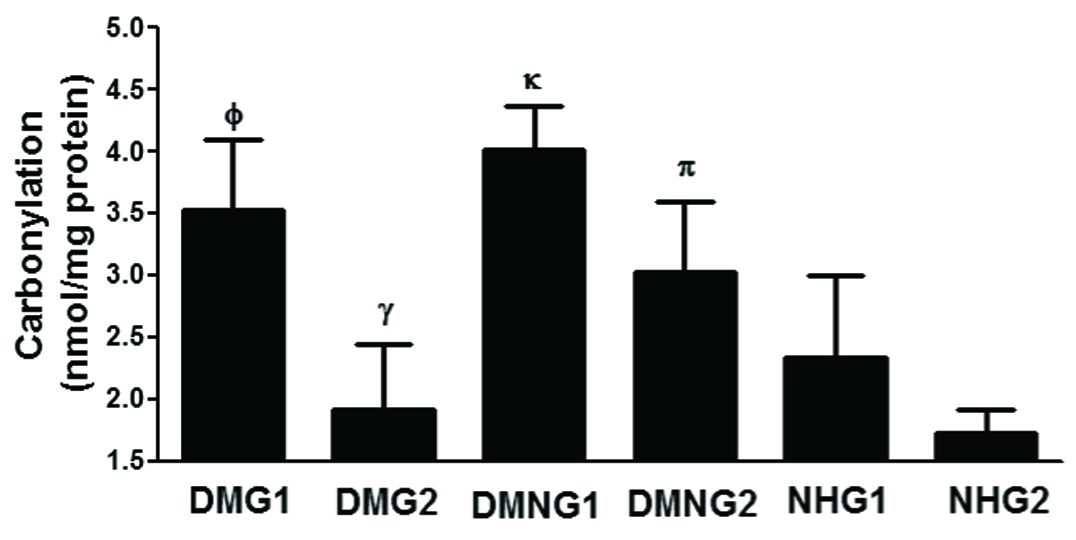
Patients’ ages - related increased of protein oxidation in patients with diabetes and diabetes associated neuropathy: To investigate the role of patients’ ages in the occurrence of protein oxidation, we assessed the increase in protein carbonylation as a function of increase patients’ ages. For that protein carbonyl contents were estimated in accordance with the following patients groups: Diabetes Mellitus patients Group 1 (DMG1; patients age≥60 years; n=17), Diabetes Mellitus patients Group 2 (DMG2; patients age<60 years; n=25), Diabetes Mellitus Neuropathy Group 1 (DMNG1; patients age≥60 years; n=15), Diabetes Mellitus Neuropathy Group 2 (DMNG2; patients age<60 years; n=22) and also in Normal Humans Group 1 (NHG1; age≥ 60 years; n=10) and Normal Humans Group 2 (NHG2; age<60 years; n=11). The average carbonyl contents (±SD) in the patients’ sera with DMG1, DMG2, DMNG1, DMNG2, NHG1 and NHG2 were 3.52±0.67, 1.92±0.73, 4.02±0.35, 3.62±0.56, 2.34±0.66 and 1.72±0.20 nmol/mg protein, respectively. As shown in [Table/Fig-4], levels of carbonyl contents in all of the diabetes patients were significantly higher in comparison with healthy controls with respect to their similar age groups (p<0.05). Importantly, levels of carbonyl contents in diabetic neuropathy patients groups (both in those with age≥60 years and in those with age<60 years) were significantly higher than diabetes patients groups of similar ages, respectively (p<0.05). Moreover, increase in levels of protein carbonyl contents in patients groups (both diabetes neuropathy and diabetes) with age≥60 years were greater in comparison with those in patients with age<60 years, suggesting a positive correlation between the protein oxidation and patients ages.
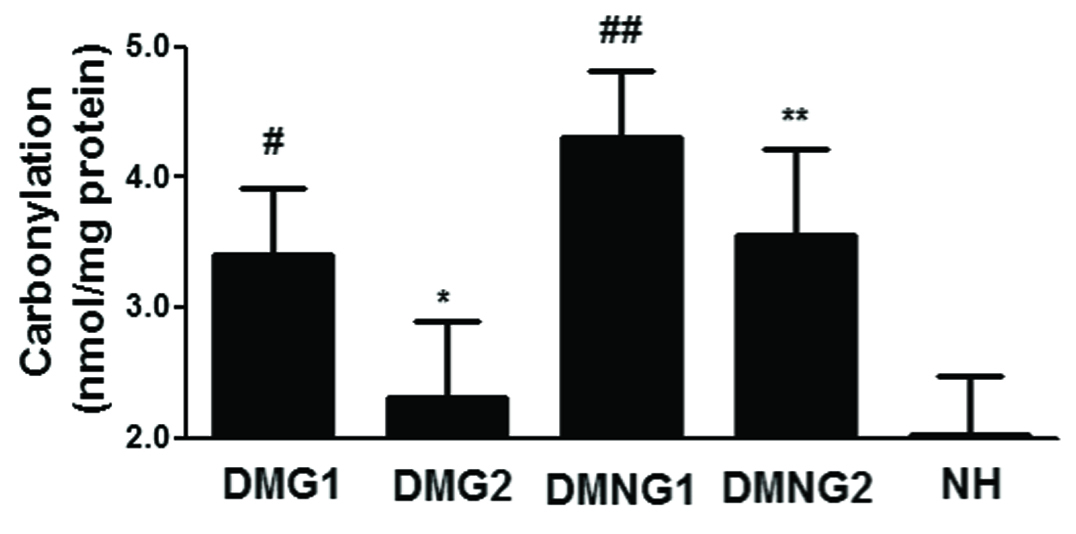
Disease duration - related increased of protein oxidation in patients with diabetes and diabetes associated neuropathy: We assessed the increases in protein oxidation by disease duration as a function of the disease activity. For that protein carbonyl contents were estimated in accordance with the following patients groups: Diabetes Mellitus patients Group 1 (DMG1; disease duration≥15 years; n=16), Diabetes Mellitus patients Group 2 (DMG2; disease duration<15 years; n=26), Diabetes Mellitus Neuropathy patients Group 1 (DMNG1; disease duration ≥15 years; n=12), Diabetes Mellitus Neuropathy patients Group 2 (DMNG2; disease duration<15 years; n=25) and also in normal humans (NH; n=21). The average carbonyl contents (±SD) in the patients’ sera with DMG1, DMG2, DMNG1, DMNG2 and NH were 3.41±0.50, 2.31±0.59, 4.30±0.51, 3.55±0.56 and 2.02±0.46 nmol/mg protein, respectively. As indicated in [Table/Fig-5], levels of carbonyl contents in all of the diabetes patients (both those with disease duration ≥15 years and those with disease duration <15 years) were significantly higher in comparison with healthy controls (p<0.01). Interestingly, levels of carbonyl contents in diabetic neuropathy patients groups (both in those with disease duration ≥15 years and in those with disease duration <15 years) were significantly higher than diabetes patients groups of similar disease duration, respectively (p<0.05). Remarkably, increase in levels of protein carbonyl contents in patients groups (diabetes neuropathy or diabetes) with disease duration ≥15 years were greater in comparison with those in patients with disease duration <15 years, suggesting a positive association between the protein oxidation and disease duration in studied patients groups.
Patients’ ages-related increased of protein oxidation in patients with Diabetes Mellitus (DM) and Diabetes Mellitus Neuropathy (DMN). Levels of protein carbonyl contents in the serum samples of patients with DM group 1 (DMG1; Age≥60 years), DM group 2 (DMG2; Age<60 years), DMN group 1 (DMNG1; Age≥60 years), DMN group 2 (DMNG2; Age<60 years), Normal Humans Group 1 (NHG1, Age≥60 years) and Normal Humans Group 2 (NHG2, Age<60 years). ξp<0.01 versus NHG1; ξp<0.05 versus ψ; Ωp<0.05 versus δ; Ωp<0.001versus NHG1. Comparison analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test.
Disease duration-related increased of protein oxidation in patients with Diabetes Mellitus (DM) and Diabetes Mellitus Neuropathy (DMN). Levels of protein carbonyl contents in the serum samples of patients with DM group 1 (DMG1; disease duration≥15 years), DM group 2 (DMG2; disease duration<15 years), DMN group 1 (DMNG1; disease duration≥15 years), DMN group 2 (DMNG2; disease duration<15 years) and normal humans (NH). #p<0.01 versus NH; #p<0.05 versus *; ##p<0.05 versus **; ##p<0.001versus NH. Comparison analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test.
Discussion
Diabetes mellitus type 2 is the most common form of diabetes, which is a complex and multifactorial chronic metabolic disorder and its prevalence has been increasing gradually in all over the world. Because of this trend, it is fast becoming an epidemic in all over the globe with the number of people affected expected to double in the next 10 years due to increase in aging population [1–3]. Till date no cure has yet been found. Uncontrolled chronic hyperglycaemia in DM patients leads to several complications particularly neuropathy. This diabetes neuropathy is a most common complication, affecting more than 60% of DM patients [23]. As type 2 DM is associated with an increased production of ROS or RNS and decreased anti-oxidants. This oxido-nitrosative stress has been postulated as a possible mechanism which might contribute to defective nerve blood supply and endoneurial oxidative damage [24]. Now, it has been well established from animal or invitro studies that, during hyperglycemic conditions balance between pro- and anti-oxidants becomes disturb which can lead to ROS and RNS-mediated oxido-nitrosative molecular damage [5–7,25]. In this study, we demonstrated the roles of protein oxidation in the progression of type 2 DM and its associated DMN patients using disease activity parameters HbA1C, patients ages and disease duration.
Biological systems are continually exposed to endogenous and exogenous ROS and RNS and proteins are their major targets due to abundance, relatively long half-lives and high rate of reactions [26]. However, overall biology of oxido-nitrosative protein modifications remains complex and is not completely defined, but protein carbonylation is quite well characterized [22]. Protein carbonylation is an irreversible, non-enzymatic modification of proteins. The carbonyl groups are introduced into proteins by a variety of oxidative/nitrosative pathways. ROS and RNS can react directly with the protein and generating products such as Reactive Carbonyl Species (RCS) then react with the proteins. Direct oxidation of proteins by ROS and RNS yields highly RCS derivatives resulting from oxidation of lysine, arginine, proline, and threonine amino acid residues [27,28]. Carbonyl groups can also be generated by the reaction of the primary amino group of lysine with RCS such as ketoamines, ketoaldehydes, deoxyosones and eventually leading to the formation of AGEs [22,25,27]. Now it is well accepted that oxidation/nitration of proteins typically results in an increase in carbonyl contents. This increase is due to the oxido-nitration of lysine, arginine, proline and threonine residues. In short, protein carbonyl groups are the most reliable biomarker of oxidative/nitrosative stress [18,22,27–29].
This study was hypothesized to investigate the role of overproduction of free radicals on protein oxidation in the progression of type 2 DM and its associated DMN. To assess this, we have demonstrated the levels of protein carbonyl contents in the sera of type 2 DM and its associated DMN patients, and analysed their relationship with glycosylated haemoglobin, disease duration and patients’ ages. Our data showed significant increase of serum protein carbonyl contents in type 2 DM patients compared with normal human subjects. Interestingly, we also found that, protein carbonyl contents were significantly higher in DMN patients compared with non-neuropathic DM patients. These data indicating that lysine, arginine, proline and threonine residues were oxidatively modified in the sera of DM patients and their levels of oxidation were more in DMN patients. These novel protein oxidations in the serum of patients were further confirmed by tryptophan and tyrosine fluorescence studies. For these studies, HSA the most abundant blood protein was isolated from patients and also from normal human subjects and then isolated protein samples were excited at 285 nm and 280 nm. Our fluorescence studies show that tryptophan and tyrosine residues were oxidatively modified in DMN or DM patients and the oxidative modification of these amino acids of albumin was significantly more in DMN patients as compared with DM patients. These results not only suggest that protein oxidation was increased more in DMN patients compared with DM patients, but also indicate the potential role of hyperglycaemia-induced protein oxidation in the pathogenesis of DM patients and/or progression to diabetes neuropathy.
To validate our central hypothesis that initiation of hyperglycaemia may be mediated by increased formation of protein carbonyl contents following excessive ROS and RNS generation and oxidative stress in DM or DMN patients, increased in protein oxidation were assessed in the sera of DM or DMN patients with varying levels of disease activity markers including HbA1C, patients’ ages and disease durations. Our study findings indicate that the formation of protein carbonyl contents is increased more in DMN and is associated with increased DM disease activity. The increased levels of protein carbonylation observed in the diabetes patients in the present study, together with HbA1C, patients’ ages or disease durations provide strong evidence of the involvement of oxidative stress in these patients.
Conclusion
Our results demonstrate the role of protein carbonyl formation in type 2 diabetes and in diabetic neuropathy, which might play an active part in the progression of disease. Our findings support an association between these protein oxidation and type 2 diabetes as well as their positive association with neuropathy. The stronger response observed in serum samples from patients with higher HbA1C levels, higher patients’ ages or higher disease duration suggest that protein carbonyl contents may be useful in evaluating the progression of diabetes neuropathy and in elucidating the mechanisms of disease pathogenesis.
Authors’ Contributions
EA and NR conceived of the study, its design, experimentation, co-ordination, data collection, data interpretation and manuscript drafting. Both authors have read and approved the final manuscript.
Abbreviations: DM, Diabetes Mellitus; DMN, Diabetes Mellitus Neuropathy; n, number of serum samples tested; HbA1C, Glycosylated Haemoglobin. *p>0.05 versus age of healthy controls; §p<0.001 versus blood glucose of healthy controls; †p<0.001 versus HbA1C of healthy controls.