Massive Ascites and Pleural Effusion in Preeclampsia
Sezen Bozkurt Koseoglu1, Ruya Deveer2, Aysun Camuzcuoglu3, Burcu Kasap4, Hakan Camuzcuoglu5
1 Medical Doctor, Department of Obstetrics and Gynaecology, Mugla Sitki Kocman Training and Research Hospital, Mugla, Mentese, Turkey.
2 Associate Professor, Department of Obstetrics and Gynaecology, Mugla Sitki Kocman Training and Research Hospital, Mugla, Mentese, Turkey.
3 Assistant Professor, Department of Obstetrics and Gynaecology, Mugla Sitki Kocman Training and Research Hospital, Mugla, Mentese, Turkey.
4 Assistant Professor, Department of Obstetrics and Gynaecology, Mugla Sitki Kocman Training and Research Hospital, Mugla, Mentese, Turkey.
5 Professor, Department of Obstetrics and Gynaecology, Mugla Sitki Kocman Training and Research Hospital, Mugla, Mentese, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sezen Bozkurt Koseoglu, Department of Obstetrics and Gynaecology, Mugla Sitki Kocman Training and Research Hospital, Mugla, Mentese-48000, Turkey.
E-mail: drsezenkoseoglu@gmail.com
Preeclampsia is defined as new onset hypertension and proteinuria after 20 weeks of gestation and complicates approximately 2-8% of all pregnancies. Release of vasoconstrictive agents, endothelial damage, hyperpermeability of the capillaries and microangiopathic haemolysis involves the basic pathophysiology. It has variable clinical presentation. Here, we report a case of severe preeclampsia who developed postpartum massive ascites and pleural effusion. Primigravid patient was admitted to our clinic at 35 weeks of gestation with very high blood pressure. In biochemical analysis, Alanine aminotransferase (ALT) was 401 U/L, Aspartate aminotransferase (AST) was 292 U/L. An emergency caesarean section was performed because of fetal distress. On the 2nd post-operative day, abdominal distension and severe abdominal pain occurred. On the 3rd post-operative day, her abdominal distension increased and Ultrasonography (USG) revealed massive ascites. Abdominal drainage was performed and albumin infusion was administered. On postoperative day 4, she still had abdominal distension and concomitant respiratory distress. Computed Tomography (CT) showed ascites and bilateral pleural effusion. Her complaint regressed on the following days.
Hypertension, Peritoneal effusion, Pregnancy
Case Report
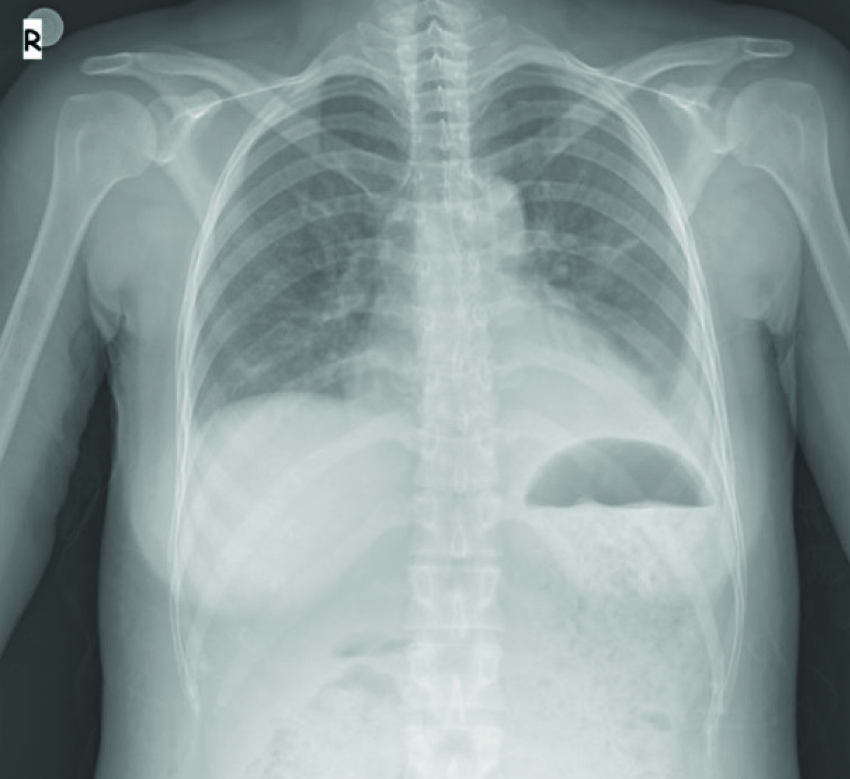
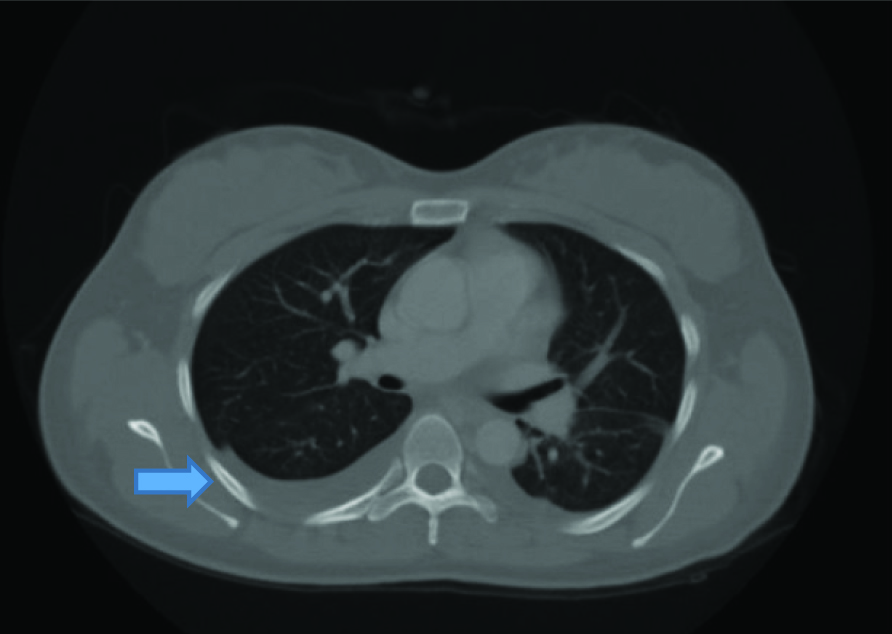
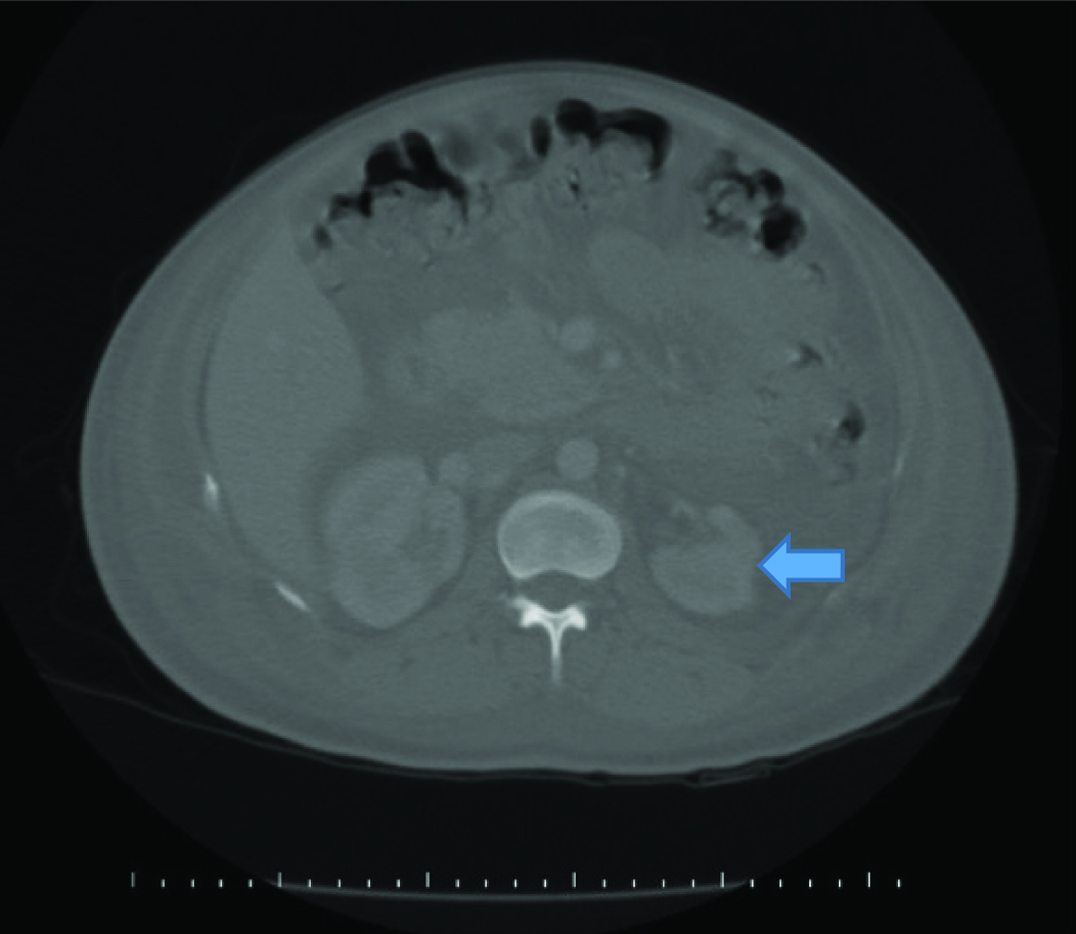
A 27-year-old primigravid female was referred to our clinic with severe preeclampsia at 35 weeks of gestation. Her medical history was uneventful. She was administered 1000 mg/day alpha-methyldopa since, 28 weeks of gestation. On admission, her blood pressure was 180/ 110 mmHg and urinary albumin 2+. Complete Blood Count (CBC) was in normal limits. Her serum biochemical analysis revealed: ALT: 401 U/L, AST: 292 U/L, creatinine: 1.39 mg/dL, urea: 40 mg/dL (16.6-48.5), uric acid: 8 mg/dL (2.4-5.7), total protein: 6.25 g/dL (6.4-8.3) and albumin: 3.3 g/dL (3.5-5.2). Her coagulation profile was within normal limits. A single live fetus of 31 weeks gestation along with 85 mm amniotic fluid index was detected by USG. Colour flow doppler USG revealed increased umbilical artery resistance. There were no subjective symptoms such as headache, epigastric pain and visual symptoms. Late decelerations were detected on cardiotocography trace and she was diagnosed to have fetal distress. An emergency cesarean section was performed and 1450 gm male fetus was delivered with APGAR score of 8/10. Postoperatively, she was given amlodipine 20 mg/day. Her blood pressure recordings were within normal limits. On first postoperative day 20-30 cc/hour urine output was detected. Serum transaminases were lowered. On the second postoperative day, she had abdominal distension and severe abdominal pain. The USG showed minimal ascites fluid. CBC was normal and serum albumin level was 2.5 gm/dl. Serum sodium level was normal. She had 320 μg albumin/mg creatinine (albumin:creatinine ratio) on spot urine sample. On the 3rd post-operative day, her abdominal distension increased and USG revealed massive ascites. Abdominal drainage was performed and albumin infusion was administered. Approximately 3000 cc serous fluid was drained. The sample analysis revealed as characteristic of transudate. Abdominal distension regressed but she had pulse of 130/min. X-ray chest showed bilateral minimal pleural effusion [Table/Fig-1]. She had normal echocardiography. Serum creatinine levels regressed (<1 mg/dL) but her urine output exceeded 500 cc/hour. IV hydration was adjusted as less than 1000 cc of total daily urine output. On post-operative day 4, she still had abdominal distension and concomitant respiratory distress. Computed Tomography showed bilateral pleural effusion and minimal ascites and atrophic right kidney [Table/Fig-2,3]. In spite of increased urine output her sodium level remained within normal levels. There was no proteinuria in spot urine sample. On post-operative day 5, she had total of 3000 cc/day hydration and 5000 cc/day urine output. Her complaint regressed on the following days and on post-operative day 7 USG showed no ascites and gap between input and output disappeared. She was discharged on postoperative day 10.
X-ray chest, postpartum day 3, bilateral minimal pleural effusion.
Computed tomography, bilateral pleural effusion and minimal ascites.
Computed tomography, atrophic right kidney.
Discussion
The precise etiology of preeclampsia has not been clarified, but it is associated with immunologic, inflammatory, genetic factors and impaired trophoblast invasion of uterine vessels [1]. Preeclampsia may have variable clinical presentation. Although the cause of ascites in preeclampsia is obscure, most probable explanation is generalized capillary leak due to endothelial cell dysfunction and reduced intravascular oncotic pressure [2]. Cong KJ and Weng TT, have reported that, the incidence of ascites in severe preeclampsia was 21.6/1000 during antenatal period [3]. Woods JB et al., have reported 10% incidence of massive ascites in HELLP syndrome [4]. Most of previous studies regarding massive ascites in preeclampsia were of antenatal period. Vaijyanath AM et al., reported massive ascites in preeclampsia which resulted with termination of pregnancy [5]. Another case with development of ascites in antenatal period and postpartum renal failure after pregnancy termination was reported by Tan A et al., [6]. Pradhan P et al., have reported massive ascites in antenatal period and development of pleural effusion in postpartum period [7]. Similar to our case Kumar R and Dey M, have reported massive ascites and bilateral pleural effusion in a postnatal case of severe preeclampsia. In their case, ascites developed on first post-operative day and worsened on second postoperative day as it was in our case [8]. Our case also had polyuria which has not been mentioned in previous reports. Serum sodium levels of the patient were within normal levels. Her serum albumin levels remained in low-normal range. Polyuria may be part of this unexplained complication of preeclampsia.
There are limited number of reports in literature about severe preeclampsia complicated by intra-abdominal hypertension [9,10]. In contrast to our case oliguria was reported in those reports. We obtained intravesical pressure in order to assess intra-abdominal pressure and found within normal limits (110 mm H2O). According to a study from Turkey, abdominal hypertension rate is very high in patients with pre-eclampsia and they emphazised that abdominal hypertension may have an additional role in preeclampsia [11]. Diagnosis of intra-abdominal hypertension and abdominal compartment syndromes were ruled out in our case.
Conclusion
Postpartum development of massive ascites and pleural effusion in severe preeclampsia is a rare event and there are very limited number of reports in literature. Management of severe preeclampsia should be multidisciplinary. The cause of postpartum ascites in severe preeclampsia is obscure. Obstetricians must be aware of postpartum complication of severe preeclampsia including the rare ones.
[1]. Sibai B, Dekker G, Kupferminc M, Pre-eclampsiaLancet 2005 365:785-99. [Google Scholar]
[2]. Brown MA, Zammit VC, Lowe SA, Capillary permeability and extracellular fluid volumes in pregnancy-induced hypertensionClin Sci 1989 77:599-604. [Google Scholar]
[3]. Cong KJ, Wang TT, Complication of ascites in pregnancy-induced hypertensionZhonghua Fu Chan Ke Za Zhi 1994 29:7-9.:58 [Google Scholar]
[4]. Woods JB, Blake PG, Perry KG, Magann EF, Martin RW, Martin JN, Ascites: a portent of cardiopulmonary complications in the preeclamptic patient with the syndrome of hemolysis, elevated liver enzymes, and low plateletsObstet Gynecol 1992 80:87-91. [Google Scholar]
[5]. Vaijyanath AM, Nayar B, Malhotra N, Deka D, Massive ascites in severe pre-eclampsia: a rare complicationJ Obstet Gynaecol Res 2002 28:199-202. [Google Scholar]
[6]. Tan A, Ma J, Deng X, Tang G, Severe ascites as the primary symptom of fulminant postpartum HELLP syndrome: a case reportClin Exp Obstet Gynecol 2015 42:685-87. [Google Scholar]
[7]. Pradhan P, Sherpa K, Joshi A, Pathak S, Massive ascites in severe pre-eclampsia: a rare complicationNepal Med Coll J 2012 14:342-44. [Google Scholar]
[8]. Kumar R, Dey M, Massive ascites and bilateral pleural effusion causing respiratory embarrassment in a postnatal case of severe preeclampsiaMed J Armed Forces India 2014 70:290-92. [Google Scholar]
[9]. Dart BWt, Cockerham WT, Torres C, Kipikasa JH, Maxwell RA, A novel use of recombinant factor VIIa in HELLP syndrome associated with spontaneous hepatic rupture and abdominal compartment syndromeJ Trauma 2004 57:171-74. [Google Scholar]
[10]. Richter CE, Saber S, Thung SF, Eclampsia complicated by abdominal compartment syndromeAm J Perinatol 2009 26:751-53. [Google Scholar]
[11]. Unsal MA, Ince U, Cengiz S, Karahan CS, Aran T, The Relationship Between Intraabdominal Hypertension and PreeclampsiaGynecol Obstet Reprod Med 2016 :22(Article in Press) [Google Scholar]