A Rare Case of Adenomatoid Odontogenic Tumour with Unicystic Ameloblastoma
Vidya Karnam Sathyanarayana1, Huldah Srigiri2, Mounija Cheemalavagupalli3, Sairam Vankadara4, Geetha Malika5
1 Postgraduate Student, Department of Oral Pathology and Microbiology, G. Pulla Reddy Dental College and Hospital, Kurnool, Andhra Pradesh, India.
2 Postgraduate Student, Department of Oral Pathology and Microbiology, G. Pulla Reddy Dental College and Hospital, Kurnool, Andhra Pradesh, India.
3 Postgraduate Student, Department of Oral Pathology and Microbiology, G. Pulla Reddy Dental College and Hospital, Kurnool, Andhra Pradesh, India.
4 Professor and Head, Department of Oral Medicine, G. Pulla Reddy Dental College and Hospital, Kurnool, Andhra Pradesh, India.
5 Postgraduate Student, Department of Oral Medicine, G. Pulla Reddy Dental College and Hospital, Kurnool, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vidya Karnam Sathyanarayana, GPR Nagar, Nandyal Road, Kurnool-518002, Andhra Pradesh, India.
E-mail: vidyaramana13@gmail.com
Unilocular, Reversal of polarity, Hyaline, Rosettes
Case Report
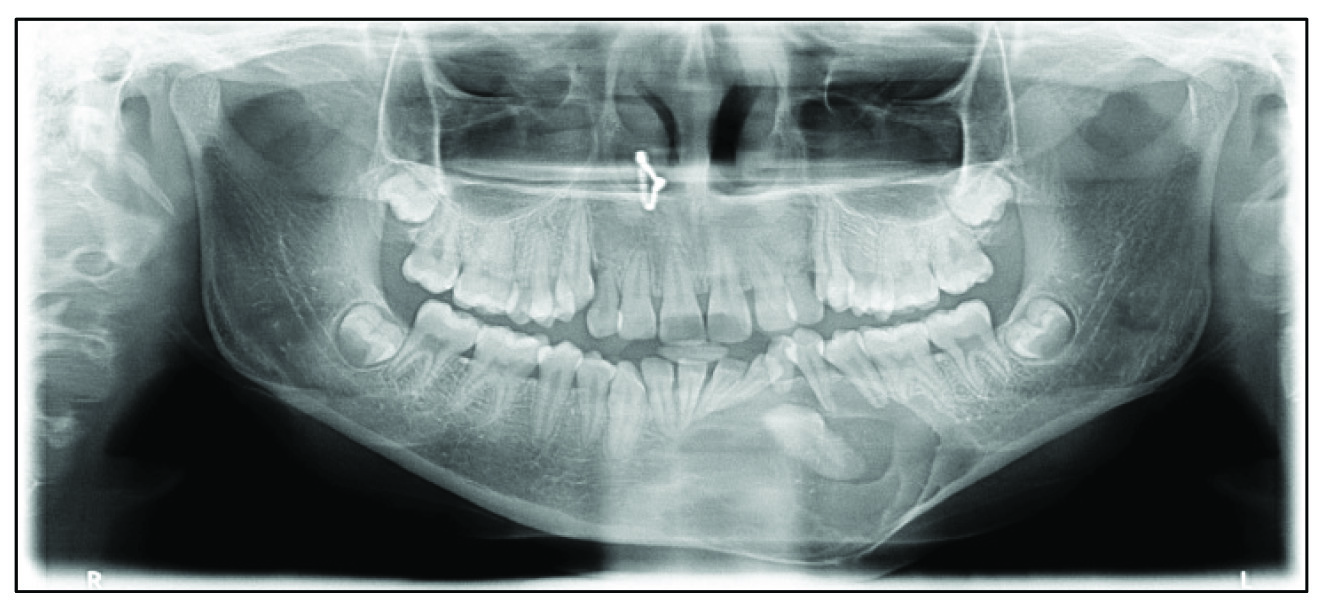
A 16-year-old female patient reported with an asymptomatic swelling on left lower half of the face since two months. On extraoral examination, swelling was present along left lower 1/3 of the face resulting in facial asymmetry [Table/Fig-1]. On intraoral examination, swelling extended from 41 to 36 region involving buccal and labial vestibule with retained 73 [Table/Fig-2]. OPG revealed unilocular radiolucency extending from 41 to 36 with impacted 33 [Table/Fig-3].
Extraoral photograph showing asymmetry of face due to swelling on left lower 1/3 of face.

Intraoral swelling along the labial and buccal vestibule.

Unilocular radiolucency with impacted left mandibular permanent canine.
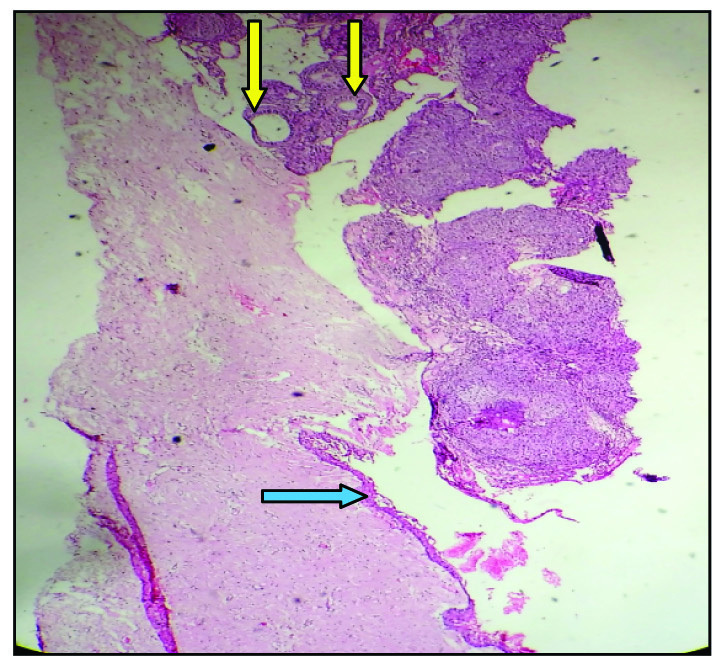
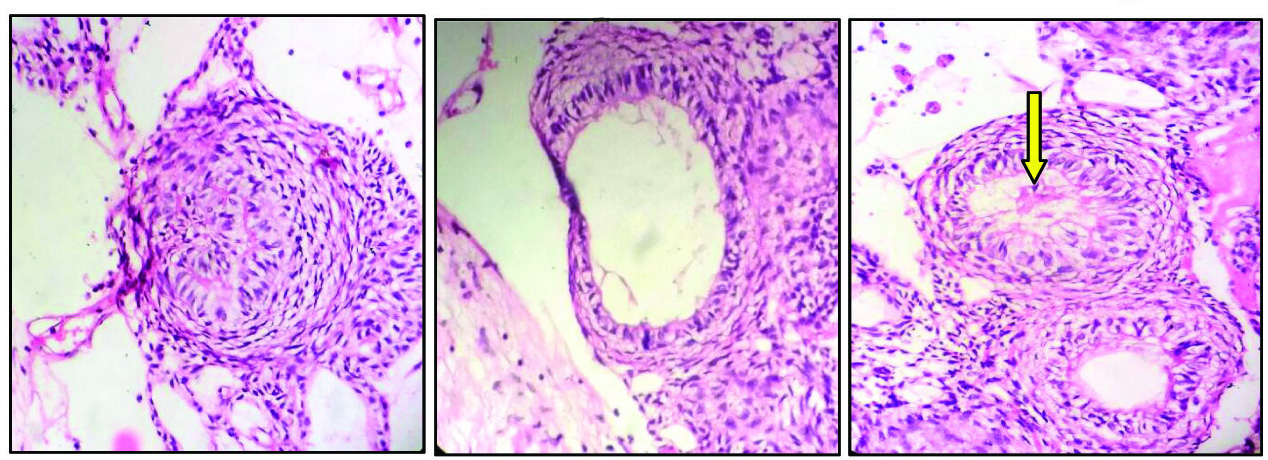
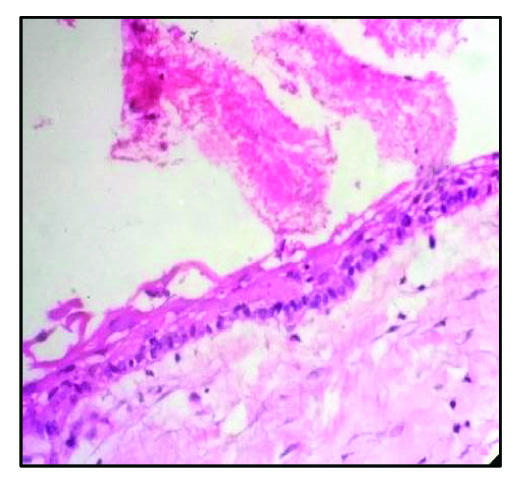
The Haemotoxylin and Eosin (H&E) stained incisional biopsy section showed odontogenic epithelium arranged in the form of nodules and sheets. The epithelial cells were arranged in rosette pattern and ducts with central lumen filled with hyaline material [Table/Fig-4]. Ducts lined by tall columnar cells with hyperchromatic nucleus away from the lumen were evident [Table/Fig-5]. In between the nodules, ducts and rosettes, spindle and stellate shaped cells were present in the form of sheets. In a focal area, a large cystic space lined by basal tall columnar cells with palisading, hyper chromatic nucleus arranged with reversal of polarity were evident and suprabasal cells were stellate reticulum like cells [Table/Fig-6]. These features were suggestive of Adenomatoid Odontogenic Tumour (AOT) with Unicystic Ameloblastoma (UA). The lesion was treated by complete excision and on one year follow up, the lesion healed uneventfully.
Rosettes and ductal pattern of AOT (yellow arrow) and cystic lining of odontogenic epithelium of UA (blue arrow) (H&E, 4X).
High power view showing (a&b) rosettes & duct like features of AOT (H&E, 40X); (c) hyaline material (arrow) in the centre (H&E, 40X).
Unicystic Ameloblastomatous lining - basal columnar cells with hyperchromatic nucleus and reverse of polarity and suprabasal cells resembling stellate reticulum cells (H&E, 40X).
Discussion
AOT and UA both are odontogenic epithelial tumours, which are frequently associated with impacted tooth and occur in 2nd decade of life [1]. The present case is unique as incisional biopsy showed one area of AOT features and another area showed UA. Its location in the anterior region of mandible with impacted permanent mandibular canine, which is not a common site of occurrence of AOT or UA makes it unusual.
Hybrid tumours consist of two or more different histologic types and occur rarely. But their combination has been noticed well in odontogenic tumours [2]. In the literature, two cases of AOT with UA were reported by Raubenheimer EJ et al., who studied infrequent clinicopathological findings in 108 ameloblastomas [3]. Another case was reported by Jivan V et al., showing existence of extra follicular AOT and UA [4]. Few other hybrid tumours like AOT with calcifying epithelial odontogenic tumour, AOT arising from calcifying odontogenic cyst, AOT developing in an ameloblastoma have also been reported in the literature [4].
It is important to report rare cases of such hybrid tumours like AOT with UA as treatment for each entity differs. AOT requires only surgical excision. But when it is present in association with UA or hybrid tumours, treatment may be radical excision and long term follow up may be required. UA present at one corner of the section may be overlooked. So, it is important to examine the full tissue specimen. Prognosis will be good, if complete excision is done with close follow up. We have done follow up for one year and the lesion healed uneventfully.
[1]. Peter A. Reichart, Hans P. Philipsen, Odontogenic Tumours and Allied Lesions 2004 [Google Scholar]
[2]. Yamazaki M, Maruyama S, Abe T, Babkair H, Fujita H, Takagi R, Hybrid ameloblastoma and Adenomatoid odontogenic tumour: report of a case and review of hybrid variations in the literatureOral Surg Oral Med Oral Pathol Oral Radiol 2014 118(1):e12-18. [Google Scholar]
[3]. Raubenheimer EJ, Heerden WF, Noffke CE, Infrequent clinicopathological findings in 108 ameloblastomasJ Oral Pathol Med 1995 24:227-32. [Google Scholar]
[4]. Jivan V, Altini M, Meer S, Mahomed F, Adenomatoid Odontogenic Tumour (AOT) originating in a unicystic ameloblastoma: a case reportHead and Neck Pathology 2007 1(2):146-49. [Google Scholar]