Neonatal Airway Compromise by a Giant Cervicothoracic Venous Haemangioma
Janardhan Shenoy1, Anita Coutinho2, Sowmini P Kamath3, Suresh Pai4, Santosh PV Rai5
1 Associate Professor, Department of Paediatrics, Kasturba Medical College, Mangalore, Karnataka, India.
2 Associate Professor, Department of Paediatrics, Kasturba Medical College, Mangalore, Karnataka, India.
3 Associate Professor, Department of Paediatrics, Kasturba Medical College, Mangalore, Karnataka, India.
4 Professor, Department of Cardiothoracic Surgery, Kasturba Medical College, Mangalore, Karnataka, India.
5 Associate Professor, Department of Radiodiagnosis, Kasturba Medical College, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sowmini P Kamath, Associate Professor, Department of Paediatrics, Kasturba Medical College, Light House Hill Road, Mangalore -575 001, Karnataka, India.
E-mail: kamathsowmini@yahoo.com
Haemangiomas are most common non-malignant vascular tumours of infancy. Here, we describe an antenatally detected mass over the neck causing compressive respiratory compromise at birth requiring resuscitative measures at birth. The mass showed increased vascularity on Contrast Enhanced Computed Tomography (CECT) with extension upto superior mediastinum. Surgical excision was required following failure to medical measures with steroids and propranolol. Histopathology confirmed it to be a venous haemangioma. This case highlights that these benign lesions may reach large sizes and antenatal detection may help in planning effective delivery and resuscitative measures.
Antenatal, Propranolol, Steroids, Superior mediastinum
Case Report
A 25-year-old primigravida was detected to have a cystic lesion with multiple septations measuring 63x55mm in the neck of her baby on a routine ultrasound examination during the eighth month of pregnancy. Previous two ultrasounds at 3rd and 6th months were reported normal. She delivered a female baby with birth weight of 2.54kg by elective caesarean section.
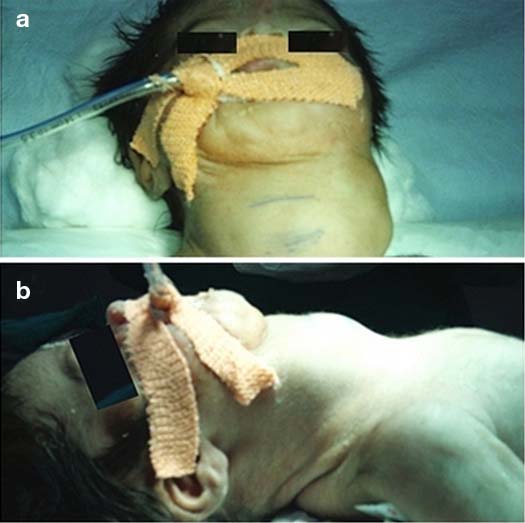
The baby required resuscitation and immediate ventilatory support due to compressive effect of the neck mass. On examination, the mass was approximately 6x5cm size, lobulated, non-pulsatile, compressible, non-reducible, extending between the anterior borders of sternocleidomastoid muscles and the lower border not defined [Table/Fig-1]. There was no bruit. It was opaque on transillumination.
a) Cystic swelling seen over the anterior aspect of the neck extending between the sternocleidomastoids bilaterally with no clear inferior border; b) Lateral view of the mass.
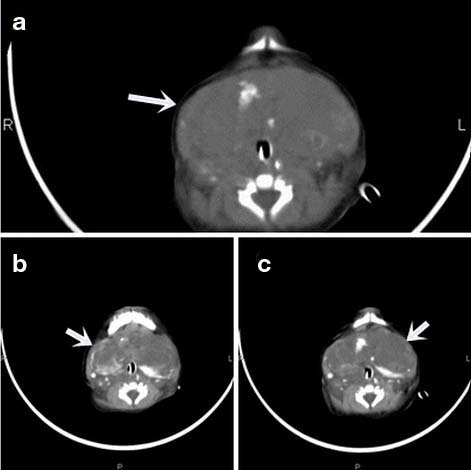
On ultrasound examination, the mass was multi-septated, cystic, vascular and extended into retrosternal area. On Contrast Enhanced Computed Tomography (CECT) scan of neck, the mass was heterogeneously enhancing, cystic, multi-septated, lobulated and involved both anterior neck and parapharyngeal spaces extending inferiorly into the pre-vascular and pre-tracheal regions of superior mediastinum with internal vascularity and pooling of contrast [Table/Fig-2]. The mass did not reduce in size with oral steroids (2mg/kg/day) and propranolol (2mg/kg/day). Recurrent airway bleeding prevented a trial of extubation and was an indication for surgical modality.
CECT axial section of the neck shows a large multicystic lesion with internal vascularity and pooling of contrast on the delayed images. Arrow mark indicates the mass lesion.
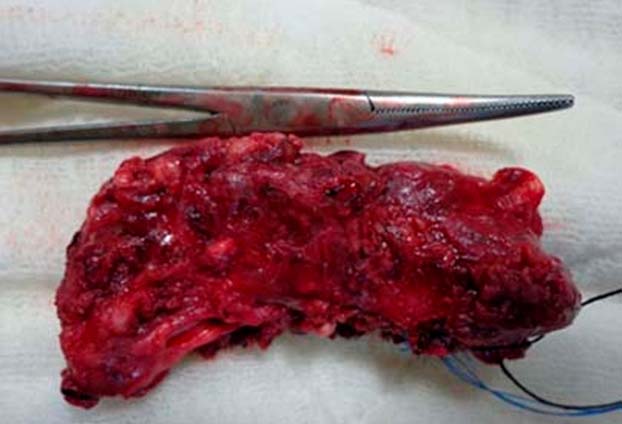
The mass was surgically excised on day 25th through a horizontal incision 2cm above the sternal notch. It was found to be vascular, encasing the trachea and extending inferiorly till parapharyngeal spaces and superior mediastinum. There was lateral displacement of the carotid and jugular vessels. A tracheal dent required suturing and reinforcement. Recurrent laryngeal nerve was secured. The swelling was excised after ligating the feeding vessels [Table/Fig-3]. Histopathology confirmed venous haemangioma with infiltration into thyroid, parathyroid and adjacent muscles [Table/Fig-4]. Post-operatively weaning was attempted over next one week along with orogastric feeding. She developed post-operative sepsis with respiratory distress and succumbed despite advanced resuscitative measures.
Lesion removed surgically along with its ligated feeding vessels.
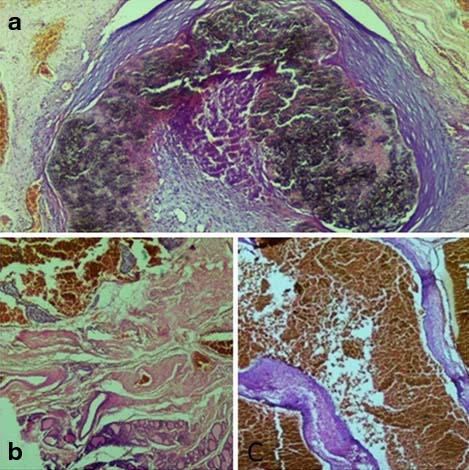
a) Dilated vascular space filled with organizing thrombus with calcification (H&E, x40). b) Upper half of picture showing cavernous vascular space and lower half showing thyroid parenchyma (H&E, x40). c) Haemangioma showing dilated irregular vascular spaces surrounded by thick and thin wall having smooth muscle fiber (H&E, x100).
Discussion
Haemangiomas are most common benign vascular tumours of infancy [1–3] characterized by a rapid, proliferative phase lasting 8 to 10 months, followed by slow, spontaneous involution over a period of several years. More than half of the cases are affected at birth, rest of them develop in the first weeks of life. They have a heterogenous clinical presentation, with variations in size, depth and differing stages of evolution. Few lesions can effect functions of nearby organs or cause permanent disfigurement [1]. A close differential diagnosis is vascular malformations which are developmental defects derived from arterial, venous, capillary and lymphatic vessels; however, these grow parallel as the child grows. Thus, a clear diagnosis is mandatory, since, the course, prognosis is different in both [1]. Haemangiomas greater than 4cm are defined as giant haemangiomas [4,5]. This case was detected to have cervicothoracic haemangioma. Venous haemangioma affects more often females, pre-mature infants and low birth weight babies [1–3]. Our case also was a pre-mature female neonate but had birth weight >2.5kg.
Antenatal detection of this large lesion over the region of the neck by ultrasound prepared us to deliver the baby by elective caesarean section in anticipation of a probable airway compromise at the time of delivery. Hence, antenatal detection is important as it allows optimising the mode and time of delivery. Prenatal MRI of the fetus also helps in effective delivery strategies [6]. Ultrasonogram of the neck postnatally confirmed the large cystic lesion as a vascular malformation however could not describe the intra-thoracic extension. Magnetic Resonance Imaging (MRI) is useful to confirm the diagnosis of deep lesions and to monitor response of the lesion to treatment [7]. CECT imaging of the neck and thorax was done revealing an inferior extension to superior mediastinum with internal vascularity and pooling of contrast. Face, nose and forehead are the usual sites of affection [1]. Giant haemangioma arising in the region of neck is rare with few cases reported in the literature [2,5].
Spontaneous resolution occurs in most cases [8,9]. Non-surgical therapy includes systemic steroids and propanolol [10,11]. Oral steroids usually are started at 2 to 3mg/kg/day, with tapering every two to four weeks with discontinuation before one year of age [12]. Tabatabaii SA et al., reported eight subglottic haemangiomas with one third having complete recovery with steroids. Corticosteroid treatment, although recognized worldwide as a treatment of haemangiomas cannot control the growth of haemangiomas in the proliferative phase or causing life threatening complications [3]. Propranolol controls growth of haemangiomas by vasoconstriction, triggering apoptosis and decreasing expression of vascular growth factor. Leaute- Labreze C et al., reported 11 infants with capillary haemangiomas responding to propranolol [13]. Oral propranolol to be initiated at a dose of 0.5mg/kg/day in three divided doses and escaled slowly to a maximum of 2mg/kg/day and could be continued for 6-12 months [14].
Laser surgery using carbon dioxide was the most common technique for the treatment of haemangiomas until 2002. Few experiences using diode laser, Potassium Titanyl Phosphate (KTP), Neodymium + Yttrium Aluminium – Garnet (Nd: YAG) have been described [3,15]. Bitar MA et al., in his systematic review [15], reported multimodalities of treatment like laser therapy with carbon dioxide, tracheostomy, steroid therapy (systemic and intralesional). Open surgery is required in extensive subglottic haemangiomas causing airway compromise.
This patient did not respond to systemic steroids and propranolol, due to proliferative phase of the haemangioma. The lesion was successfully removed surgically.
Conclusion
Infantile haemangiomas are common and usually resolve spontaneously. Extensive and deeply situated haemangiomas can be life threatening and require early identification and intervention. Multimodality treatment may be essential in such cases to have a favourable outcome.
[1]. Conlon JD, Drolet BA, Skin lesions in the neonatePediatr Clin North Am 2004 51(4):863-88. [Google Scholar]
[2]. Hussain A, Mahmood H, Almusawy H, Moderate size infantile heamangioma of the neck-conservative or surgical treatment?: A case reportJ Med case Rep 2008 2:52available from: http://www.jmedicalcasereports.com/content/2/1/52 [Google Scholar]
[3]. Tabatabaii SA, Khanbabaii G, Khatami AR, Sharifnia SA, Characteristic and follow-up of subglottic haemangiomas in Iranian childrenJ Res Med Sci 2010 15(4):235-39. [Google Scholar]
[4]. Suma V, Marini A, Gamba PG, Luzzatto C, Giant haemangioma of the thigh: prenatal sonographic diagnosisJ Clin Ultrasound 1990 18(5):421-24. [Google Scholar]
[5]. Uehara S, Hasegawa T, Okuyama H, Kawahara H, Kabota A, Osuga K, Prenatally detected giant congenital haemangioma of the fetal neckJ Ped Surg Case Reports 2013 1:29-31. [Google Scholar]
[6]. Shiraishi H, Nakamura M, Ichihashi K, Uchida A, Izumi A, Hyodoh H, Prenatal MRI in a foetus with a giant neck haemangioma: A case reportPrenat Diagn 2000 20(12):1004-07. [Google Scholar]
[7]. Greenspan A, McGahan JP, Vogelsang P, Szabo RM, Imaging strategies in the evaluation of soft-tissue haemangiomas of the extremities: Correlation of the findings of plain radiograph, angiography, CT, MRI and ultrasonography in 12 histologically proven casesSkeletal Radiol 1992 21(1):11-18. [Google Scholar]
[8]. Ceisler EJ, Santos L, Blei F, Periocular haemangiomas: What every physician should knowPediatr Dermatol 2004 21(1):1-9. [Google Scholar]
[9]. Picard A, Soupre V, Diner PA, Buis J, Goga D, Vazquez MP, Early surgery of immature haemangiomas with the aid of an ultrasonic scalpelApropos of 81 cases Rev Stomatol Chir Maxillofac 2002 103(1):10-21. [Google Scholar]
[10]. Dourmishev LA, Dourmishev AL, Craniofacial cavernous haemangioma:Succesful treatment with methylprednisoloneActa Dermatovenerol Alp Panonica Adriat 2005 14(2):49-52. [Google Scholar]
[11]. Uysal KM, Olgun N, Erbay A, Sarialioglu F, High-dose oral methylprednisolone therapy in childhood haemangiomasPediatr Hematol Oncol 2001 18:335-41. [Google Scholar]
[12]. Marler JJ, Mulliken JB, Current management of haemangiomas and vascular malformationsClin Plast Surg 2005 32(1):99-116. [Google Scholar]
[13]. Leaute-Labreze C, Dumas de la Roque E, Hubiche T, Boralevi F, Thambo JB, Taïeb A, Propranolol for severe haemangiomas of infancyN Engl J Med 2008 358:2649-51. [Google Scholar]
[14]. Drolet BA, Frommelt PC, Chamlin SL, Haggstrom A, Bauman NM, Chiu YE, Initiation and use of propranolol for infantile haemangioma: Report of a consensus conferencePediatrics 2013 131(1):128-40. [Google Scholar]
[15]. Bitar MA, Moukarbel RV, Zalzal GH, Management of congenital subglottic haemangioma: Trends and success over the past 17 yearsOtolaryngol Head Neck Surg 2005 132(2):226-31. [Google Scholar]