Adenoid was initially described by Meyer in 1868 as a nasopharyngeal lymphoid tissue which forms a part of the Waldeyer’s ring [1]. Adenoid Hypertrophy (AH) can result in upper airway obstruction in children [1]. Children with this condition present with symptoms of chronic nasal obstruction, rhinorrhoea, mouth breathing, snoring, recurrent sinusitis and recurrent otitis media with effusion [2,3]. AH is one of the leading causes of obstructive sleep apnea in children. Long-term obstructive sleep apnea due to adenoids can develop serious consequences including cor pulmonale, failure to thrive, permanent neurologic damage, hypersomnolence, behavioural disturbances and developmental delays [4].
Adenoidectomy is one of the most common surgical procedures performed in children, either alone or in conjunction with tonsillec-tomy or grommet insertion. The conventional adenoidectomy using curette was first described in 1885 [1]. This procedure is performed blindly by most surgeons without visualising the nasopharynx; which leads to uncommon complications such as inadequate adenoid tissue removal, eustachian tube scarring, bleeding and nasopharyngeal stenosis. This has led to development of alternate surgical methods, which has been made possible with the advent of rigid nasal endoscopes, cold light source, fiber optics and powered instruments [5,6]. We wish to present our experience with combined conventional and endoscopic microdebrider-assisted adenoidectomy.
Materials and Methods
This was a prospective study of 60 child patients who underwent combined conventional and endoscopic microdebrider-assisted adenoidectomy performed by the surgeon at Department of Otorhinolaryngology, DM WIMS Hospital, Wayanad, Kerala, India. The study was conducted between September 2013 to September 2015. This study included children undergoing conventional and endoscopic microdebrider-assisted adenoidectomy either as a single procedure or along with other procedures like tonsillectomy, septoplasty and myringotomy with grommet insertion [Table/Fig-1]. Informed consent was obtained and study was approved from ethics committee.
Procedures done along with adenoidectomy.
| Procedure | Number of cases | Percentage |
|---|
| Adenoidectomy | 14 | 23.3 |
| Adenoidectomy + Tonsillectomy | 32 | 53.3 |
| Adenoidectomy + Myringotomy with Grommet Insertion | 4 | 6.7 |
| Adenoidectomy + Tonsillectomy +Myringotomy with Grommet Insertion | 8 | 13.3 |
| Adenoidectomy + Septoplasty | 2 | 3.3 |
| Total | 60 | 100 |
The AH was graded as per Celmens and McMurray scale, i.e. grade 1 (< 1/3rd choanal obstruction), grade 2 (1/3rd to 2/3rd choanal obstruction), grade 3 (2/3rd to almost complete choanal obstruction by the adenoid tissue) and grade 4 (complete obstruction). All the children presenting with grade 3 and grade 4 AH, confirmed by diagnostic nasal endoscopy at the beginning of the procedure were included in the study. At the end of conventional adenoidectomy, the AH was graded again and compared to the pre-operative findings. Those children with grade 3 and grade 4 AH were considered to have significant airway obstruction.
These children underwent conventional adenoidectomy by curettage along with endoscopic microdebrider-assisted adenoidectomy. The duration of the surgery was calculated only for the conventional and endoscopic adenoidectomy portion of the procedure. The material collected at the end of the procedure from suction canister was filtered to remove adenoid tissue and the remaining fluid comprising of blood and irrigating fluid was measured. The precise amount of blood loss was calculated by subtracting the quantity of irrigating fluid used from this amount. Nasopharyngeal pack blood soakage was measured by weighing the difference at the beginning and end of the procedure. Intra-operative complications such as injury to adjacent structures, if any were identified and recorded.
All children were reviewed in the Ear Nose and Throat Outpatient Department by clinical examination and diagnostic nasal endoscopy after one week and one month of surgery. Post-operative complications like neck pain, hypernasality and swallowing problems were noted.
Each symptom was given a score of one, 1 for nasal obstruction, 1 for mouth breathing, 1 for snoring, 1 for recurrent sinusitis and 1 for deafness [Table/Fig-2]. Thus, a total score out of 5 was given for these patients prior to surgery, one week and one month after surgery. Their symptom score was reviewed after one year of surgery by telephonic interview.
Symptom score for adenoid hypertrophy.
| Symptom | Score |
|---|
| Nasal Obstruction | 1 |
| Mouth Breathing | 1 |
| Snoring | 1 |
| Recurrent Sinusitis | 1 |
| Deafness | 1 |
| Total Score | 5 |
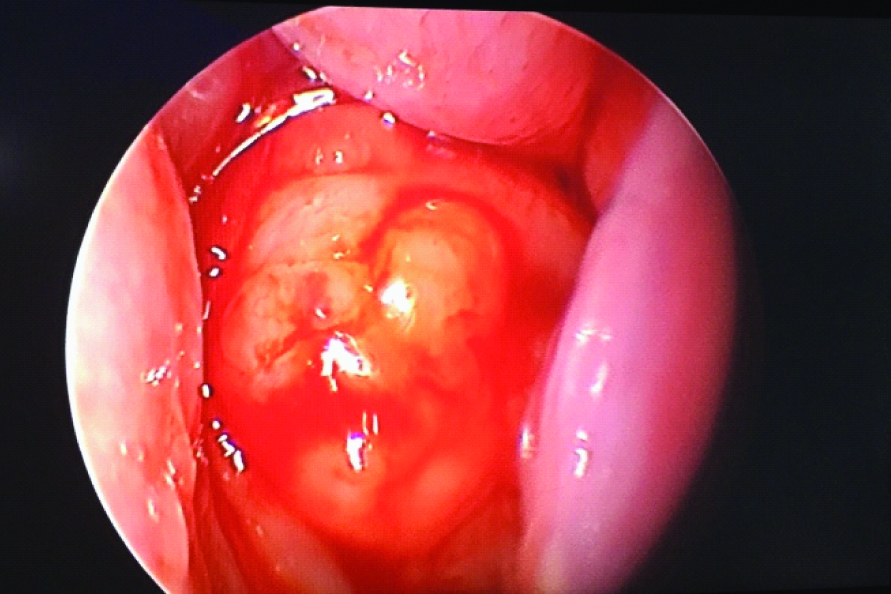
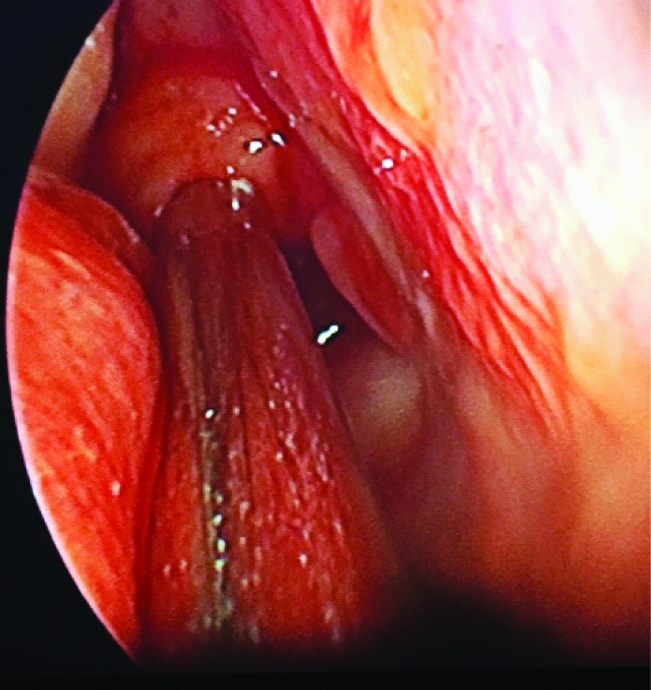
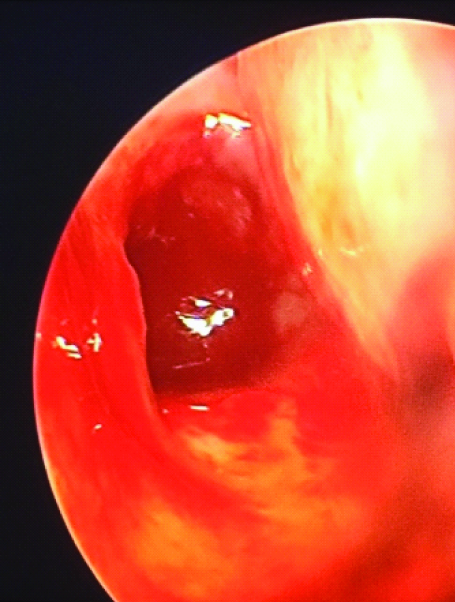
Surgical technique: Patient was subjected to General Anaesthesia (GA) via an orotracheal tube. Both the nasal cavities were decongested by using pledgets soaked in 4% xylocaine with 1:10,000 adrenaline. A 0° 2.7mm or 4mm rigid endoscope was used to visualise the adenoid tissue as per Clemens and McMurray scale. Then the child was placed in supine in the Rose position and Boyle-Davis mouth gag was inserted as in tonsillectomy. Then St. Clair Thompson adenoid curette was used initially to perform a conventional adenoidectomy. Ribbon gauze was placed in the nasopharynx for attaining haemostasis and removed after five minutes. Then the neck extension was removed and the residual adenoid tissue found obstructing the nasal choana and tubaric regions was reassessed as per Clemens and McMurray scale after doing endoscopy [Table/Fig-3] and was compared to the initial findings. Then with a 2.7mm or 4mm 0° Storz rigid endoscope, Stryker microdebrider was used at 3000rpm in oscillating mode to remove the adenoid tissue from the choanal and tubaric regions [Table/Fig-4]. Once all the adenoid tissue was removed [Table/Fig-5], 4% xylocaine with 1:10,000 adrenaline soaked nasal pledgets were put in place for five minutes till bleeding stopped and then removed. No nasal pack was placed in the nasal cavity except in children undergoing septoplasty along with adenoidectomy.
Grade 3 adenoid hypertrophy after conventional adenoidectomy
Endoscopic microdebrider-assisted adenoidectomy.
Complete clearance of adenoid tissue after combined conventional and endoscopic adenoidectomy.
Results
Out of the 60 patients, 30(50%) were males and 30(50%) were females. The youngest child who underwent the procedure was 3 years while the oldest child was 16 years. The mean age of patients was 9 years.
In our study 14 (23.3%) patients underwent adenoidectomy alone, 32 (53.3%) patients underwent adenotonsillectomy, 4 (6.7%) patients underwent adenoidectomy and myringotomy with grommet insertion, 8 (13.3%) patients underwent adenotonsillectomy and myringotomy with grommet insertion, while only 2 (3.3%) patients underwent adenoidectomy with septoplasty [Table/Fig-1].
The diagnostic nasal endoscopy done to visualise the adenoid tissue obstruction of the choana as per Clemens and McMurray scale showed that, out of 26 children who had grade 3 AH at the beginning of the procedure, two (7.7%) of them had grade 1, sixteen (61.5%) of them had grade 2 while eight (30.8%) of them had grade 3 AH after conventional adenoidectomy. Out of 34 children who had grade 4 AH initially, only 9 (26.5%) of them had grade 2, 20 (58.8%) of them had grade 3 while 5 (14.7%) of them had grade 4 AH after conventional adenoidectomy [Table/Fig-6]. In this study after conventional adenoidectomy, 33 out of 60 (55%) had significant airway obstruction (grade 3 and grade 4 AH).
Diagnostic nasal endoscopy findings as per Clemens and McMurray scale for adenoid hypertrophy.
| Pre-operative | After conventional adenoidectomy |
|---|
| Grade 3: 26 | Grade 1: 2 (7.7%) |
| Grade 2:16 (61.5%) |
| Grade 3: 8 (30.8%) |
| Grade 4: 34 | Grade 2: 9 (26.5%) |
| Grade 3: 20 (58.8%) |
| Grade 4: 5 (14.7%) |
With the help of combined conventional adenoidectomy by curettage along with endoscopic microdebrider-assisted adenoidectomy, we were able to get complete clearance of adenoid tissue in all 60 (100%) cases, along with better surgeon satisfaction.
None of the children complained of neck pain as major duration of the surgery, (i.e. endoscopic microdebrider-assisted adenoidectomy) was performed without neck extension. There were 2 (3.3%) children with grade 4 adenoid hypertrophy who had developed nasal regurgitation which lasted only for 3 to 4 days after undergoing the procedure. There were 7 (11.6%) children who developed hypernasality for the first week. Both these symptoms subsided completely within 1 week to 10 days of the procedure. There were no other major complications like late post-operative haemorrhage, nasopharyngeal stenosis or velopharyngeal insufficiency in our study.
The mean pre-operative symptom score for AH was 3.7, which improved to 0 after one month of combined conventional and endoscopic microdebrider-assisted adenoidectomy. All children were symptom-free at the end of one month and one year.
The duration of conventional adenoidectomy was 5 minutes 12 seconds while total duration of the combined conventional and endoscopic microdebrider-assisted adenoidectomy was 14 minutes 45 seconds. There was no significant blood loss (15±3 ml approximately) though initially there was more bleeding due to the increased raw area exposure after debriding adenoid tissue.
Discussion
Conventional adenoidectomy with St. Clair Thompson curette being a blind procedure leads to residual tissue being found close to the nasal choana and adjacent torus tubaris. This has been confirmed by Havas and Koltai in their respective studies [5,6]. Our study also shows that there was residual tissue in the nasal choana in children undergoing conventional adenoidectomy. This could explain why most patients have partial relief of symptoms on long term follow-up. The reason for failure of conventional adenoidectomy is due to inability of the curette to reach these regions.
After conventional adenoidectomy, 39% of patients had moderate residual disease which might later re-grow and cause airway obstruction as per study by Havas [5]. In the study by Pagella, 48.9% of patients had significant obstructing adenoid tissue after conventional curette adenoidectomy [7]. As per our study; there was significant airway obstruction in 55% of patients due to AH.
In 1997, Koltai et al., had introduced power-assisted adenoidectomy with adenoid resection being visualised using a laryngeal mirror [6]. The transnasal approach using endoscopic guided microdebrider assisted adenoidectomy was first reported by Yanagisawa and Weaver in 1997 [8]. Constantini had used a 70° endoscope with video attachment introduced through the mouth to visualise the nasopharyngeal cavum, while he used a 40° microdebrider blade to remove the adenoid tissue [9].
The advantages of endoscopic microdebrider-assisted adenoidectomy include improved visualisation of the surgical field, continuous suction of blood and thereby, enabling complete and precise removal of adenoid tissue from the choanal and tubaric regions [10]. There is also no need to extend the neck during the endoscopic procedure. The high definition monitor display enables training residents and recording for documentation. There was also high degree of surgeon satisfaction due to improved plane of dissection [10].
The combined adenoidectomy approach was initially reported by Pagella et al., in 2009 [7]. The combination of conventional method of adenoidectomy along with endoscopic microdebrider-assisted adenoidectomy helps to avoid the need for angled endoscopes and angled microdebrider blades. The difficulty in manoeuvring endoscopes and microdebrider tips through the same nostril can be overcome by using the endoscope through one nostril with microdebrider shaver blade passed through the other nostril [11].
The duration of this combined procedure was approximately 14 minutes 45 seconds. This was due to increased organisation and preparation time. As per the study by Somani et al., endoscopic adenoidectomy had operating time of 12 minutes 30 seconds, which was shorter by 2 minutes when compared to conventional adenoidectomy [12].
Endoscopic microdebrider-assisted adenoidectomy is technically more difficult to perform than conventional adenoidectomy [13,14]. But it is easy to learn for those who are routinely performing endoscopic sinus surgery [15].
Limitation
The main limitation of microdebrider include high cost of the devise, the replacement cost of blades and lack of resected tissue for histopathological examination [16]. Other limitation of our study includes lack of control group. By this study we wish to establish the safety and efficacy of this procedure currently being routinely carried out at our institution.
Conclusion
The combined approach of conventional curette along with endoscopic microdebrider-assisted adenoidectomy is a safe and effective method. The microdebrider under endoscopic guidance helps to attain controlled complete adenoid tissue resection thereby, minimising blood loss and complications.