Anxiety and depression are important co-morbid conditions, often under-diagnosed, that influences quality of life and prognosis in Chronic Obstructive Pulmonary Disease (COPD) [1]. The Global Initiative for Chronic Obstructive Lung Disease, GOLD (updated 2015) has given tremendous emphasis on assessment of these disease conditions as a part of evaluation of stable COPD patients. Depression and anxiety symptoms are related to age, gender, poor quality of life and more severe symptoms [2,3]. The Indian studies published so far have revealed high prevalence of depression (50-72%) among stable COPD patients based on a self-administered questionnaire, physical health questionnaire (PHQ-9) [4,5]. Another study from the Northern India reported that 44.8% of patients suffering from stable chronic respiratory illness (that includes asthma, COPD, Diffuse Parenchymal Lung Disease (DPLD), allergic rhinitis with/without asthma) have mental illness as compared to 24.3% among healthy adults based on a computer-assisted semi-structured interview system, the Global Mental Health Assessment Tool, Primary Care Version (GMHAT/PC) [6]. Anxiety (20.6%), depression (13.2%) and Obsessive Compulsive Disorders (4.6%) were the most frequently identified mental disorders in the respiratory disease group [6]. Though depression in COPD patients was associated with more symptoms and reduced six-minute walk distance as compared to non-depressed COPD subjects in a study by Marco FD et al., it was not found as an independent factor for reduced number of daily steps [7]. The early identification of these conditions and early initiation of therapy is essential before enrolling in pulmonary rehabilitation program for a comprehensive care of COPD patients.
The present study was aimed at assessment of depression and/or anxiety among stable COPD patients in a sub-urban locality of Eastern India, based on a questionnaire which is reliable, practicable and also affordable in a clinical setting and to identify the factors contributing to reduced functional capacity as assessed by six-minute walk distance with special emphasis on patients’ mental health.
Materials and Methods
It was a descriptive cross-sectional study, conducted in the out-patient Department of Pulmonary Medicine in a tertiary care hospital in a sub-urban area in Eastern India for a period of six months (March 2014 – September 2014).
The patients diagnosed with COPD in the Chest OPD or receiving treatment for COPD from other department of the hospital or private practitioners were entered in a COPD register. Subsequently, those satisfying all inclusion criteria were enrolled in the study.
The inclusion criteria for the study were stable COPD with no history of exacerbation in last two months [8] irrespective of smoking status. The exclusion criteria were those suffering from acute exacerbation (admitted in hospital for worsening of respiratory symptoms/attended out-patient clinic or emergency department and were prescribed antibiotic with escalation of doses of inhalation medications and/or systemic corticosteroids) within last 1 month, those already on antidepressant or anti-anxiety medication, suffering from mania, co-morbid conditions like uncontrolled diabetes, uncontrolled hypertension, chronic liver disease, malignancy, HIV/AIDS, chronic renal disease undergoing regular dialysis, those using walking-aids or severe arthritis that may hamper their walking capacity. After obtaining the consent, they were interviewed by designated interviewers to assess the physical and psychological health and basic investigations that include clinical examination and spirometry were done. The co-morbid conditions like diabetes, hypertension and ischemic heart disease were assessed by the standard investigations. All the patients were given appointment for six-minute walk test within 1 week of the day of recruitment. The study design was approved by the Institutional Ethics Committee.
Diagnosis and assessment of respiratory symptoms: COPD was diagnosed as per GOLD guideline with post-bronchodialator FEV1/FVC < 70 and severity was assessed by dyspnea scale (mMRC score), Clinical COPD Questionnaire (CCQ), spirometry parameters (Spirobank II; MIR—Via Maggiolino, Roma, Italy) and history of prior exacerbation or hospitalization in last 1 year as per recommendation by GOLD guideline [1].
Clinical COPD Questionnaire (version – for week, English and Hindi version) - It is a self-administered questionnaire specially developed to measure clinical control in patients with COPD. The questions are divided into three domains i.e., symptoms, functional and mental state (scale: 0 = best, 6 = worst). This was preferred as it was easier and faster to complete than St George Respiratory Questionnaire (SGRQ) even in patients with low education level [9].
Calculation of scores: CCQ total score = (item 1 + 2 + 3 + 4 + 5 + 6 + 7 + 8 + 9 + 10)/10; Symptom = (item 1 + 2 + 5 + 6)/4; Functional state = (item 7 + 8 + 9 + 10)/4; Mental state = (item 3 + 4)/2.
Psychological assessment: Psychological assessment was done by well-validated questionnaire as described below by a designated interviewer.
Hamilton depression rating scale (HAM-D) – This is one of the most widely used and accepted questionnaire to identify and assess severity of depression. It is designed to be administered by a trained professional using a semi-structured interview based on 21-point questionnaire [10]. It usually took 20 min to complete the interview. Eight items are scored 0 – 4, nine items are scored 0 – 2 and last four are not scored. The sum total of the 17 items is the total score and severity of the disease is classified as: normal 0–7, mild 8–13, moderate 14–18, severe 19–22 and very severe ≥23.
State Trait Anxiety Inventory (STAI) – It is a reliable and validated cross-cultural assessment tool for anxiety. Both state anxiety and trait anxiety was assessed by a trained professional. It is a 20 – item self-report assessment device appropriate for research and clinical purpose. STAI is not a diagnostic tool. There is controversy regarding the cut-off value to determine clinically significant anxiety as it varies widely with age, underlying disease condition and presence of mental disorders. However higher score is associated with higher level of anxiety. Since our study includes mostly elderly population with chronic illness, we considered 39 -40 as cut-off value to define clinically significant anxiety disorder [2,11].
The questionnaires used in the study were double translated and validated in Hindi and Bengali by three bilingual researchers.
Statistical Analysis
Statistical analysis was performed using Minitab software (version16.1). The data was summarized as mean±SD for normal distributed data and the median (5th and 95th percentile) for non-parametric data. The paired t-test or Mann-Whitney tests were done to assess any significant difference between the two groups. Finally a regression analysis was done with functional capacity as dependent variable and anthropometric parameters, disease severity and presence of co-morbid conditions like depression and anxiety as predictor variable.
Results
There were 75 stable COPD patients (68 male, 7 female), with age range 45-82 years. The clinical profile of the patient population is shown in [Table/Fig-1].
The clinical profile of the COPD patient population in the study.
| COPD patients (N = 75) |
|---|
| Male (N=68) | Female (N=7) | Overall (mean) |
|---|
| Age, yrs* | 62.13 (9.23) | 61.71 (8.98) | 62.09 (9.15) |
| Smoking index* | 624.3 (550.1) | 414 (584) | 604.7 (552.7) |
| BMI* | 19.676 (3.791) | 22.33 (4.92) | 19.923 (3.947) |
| FEV1, L* | 1.1803 (0.4561) | 0.8229 (0.2462) | 1.1469 (0.4519) |
| FEV1 % pred* | 51.16 (18.13) | 50.29 (12.46) | 51.08 (17.61) |
| CCQ score* | 21.559 (7.632) | 25.86 (7.67) | 21.96 (7.687) |
| mMRC* | 1.8235 (0.7715) | 2.0 (0.577) | 1.84 (0.7541) |
*Mean±SD
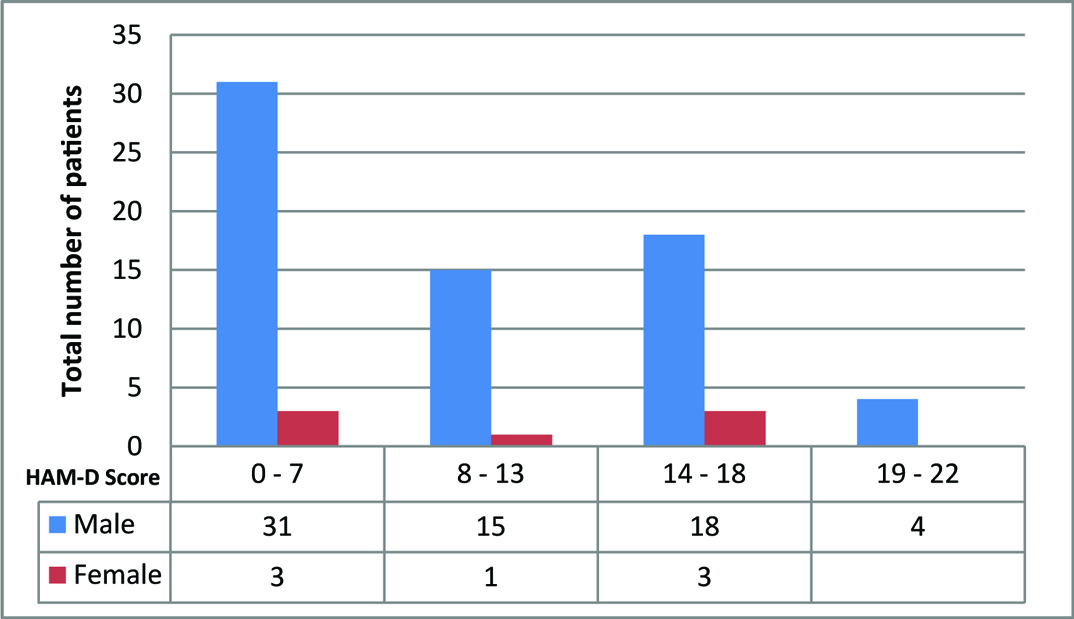
Most of the patient population were in COPD group D (N= 35, 46.67%), followed by group A, B and C (N= 17,22.67%; N= 17, 22.67%; and N = 6, 8% percent respectively). 32 out of 75 patients (42.6%) had depression and anxiety both, 37 out of 75 (49.3%) had mild to moderate depression, whereas 4 out of 75 (5.3%) were detected with severe depression with HAM-D score above 19 [Table/Fig-2]. Overall, 37 out of 68 male patients and 4 out of 7 female patients (overall 54.7%) with stable COPD were diagnosed with depression. Chi-square test showed that patients with GOLD severity group A had no significant difference in occurrence of depression in GOLD severity group D (p = 0.118). The depression was not dependent on the gender distribution of the study population (p = 0.890) [Table/Fig-3]. A total of 28 patients, all men, were unemployed, 5 female were homemakers and rests were employed or self-employed. The employment status and history of smoking had no correlation with the occurrence of depression among stable COPD patients (p-values 0.635, and 0.755 respectively).
Total number of patients with anxiety and depression in the study population.
| No anxiety | Anxiety | Total |
|---|
| No depression | 25 | 9 | 34 |
| Depression | 9 | 32 | 41 |
| Total | 34 | 41 | 75 |
Distribution of HAM-D score among COPD patients.
All 75 patients participated in 6MWT. However, nine of them had to stop during the test, mainly due to shortness of breath, maximum up to five times. There was no significant difference in distance walked in six minutes among patients with depression and without depression (p = 0.4186). Mann-Whitney Test confirmed that there was no significant difference in distance walked in six minutes between male and female COPD patients (p = 0.1719). The CCQ score was found to be significantly high among COPD patients with depression as compared to patients with no depression (25 vs. 18, p =0.003) [Table/Fig-4]. However, there was no definite correlation between CCQ score and HAM-D score (r = 0.447).
Characteristics of patients with stable COPD with reference to depression.
| Depression (N=41) | No depression (N=34) | p -value |
|---|
| Age * | 62 | 65 | 0.0906†** |
| BMI * | 18.1 | 20.4 | 0.3799** |
| Smoking index * | 560 | 550 | 0.9321** |
| FEV1 % pred * | 47 | 54.5 | 0.1782** |
| FEV1, L | 1.104 | 1.199 | 0.377*** |
| CCQ score * | 25 | 18 | 0.003** |
| HAM-D score * | 15 | 7 | <0.0001** |
| 6MWD | 412.79 | 430.7 | 0.351*** |
*median value, **Mann-Whitney test and *** 2 Sample t-test
† Significant at Alpha =0.1
[Table/Fig-4,5] describes the summary of 6MWT among the stable COPD patients in the study. The change in heart rate and respiratory rate among patients with depression as compared to those without depression by Mann-Whitney test were not found to be significant (p = 0.219 and 0.41 respectively). However, the patients with depression were significantly more short of breath after the walk test as compared to those without depression (p = 0.003) by Mann-Whitney test. There was no significant difference in the distance walked in six minutes between patients with depression (N = 41, 420 Median) as compared to the patients without depression (N = 34, 425.2 Median) (p=0.4186), as also with patients with higher STAI score compared to low STAI score (N= 41, 411.4±89.4 vs. N=34, 432.5±77.5, p=0.276). 6 out of 34 patients without depression and 9 out of 41 with depression had a drop in SpO2 >4%. However, none required oxygen supplementation during the test.
Details of six-minute walk test among COPD patients.
| No depression | Depression |
|---|
| Pre-testMean (SD) | Post-testMean (SD) | p-value | Pre-testMean (SD) | Post-testMean (SD) | p-value |
|---|
| HR | 86.1 (14.1) | 98.8 (16.5) | <0.001 | 93.2(14.8) | 110.2(17.2) | <0.001* |
| RR | 18.6 (2.98) | 27.6 (4.5) | <0.001 | 19 (3.66) | 29.8 (5.3) | <0.001* |
| SpO2 | 97.7 (1.16) | 95.9 (4.11) | 0.003 | 97.8 (.79) | 95.6 (3.2) | <0.001* |
| BORG scoreDyspnea | 0.1471 (.4357) | 1.5(1.477) | | 0.36 (.689) | 2.61 (1.595) | |
| BORG scoreLeg fatigue | 0 | 0.58 (1.373) | | 0 | 1.256 (1.736) | |
| Leg cramp | - | 2 (5.9%) | | - | 11 (26.8%) | 0.016** |
| Need to stop | - | 3 (8.8%) | | - | 6 (14.6%) | |
| 6MWD | - | 430.87 (76.29) | | - | 412.79 (90.57) | 0.351*** |
*Paired t-test **2 Proportion test ***2 Sample t-test
HR – Heart Rate
RR – Respiratory Rate
SpO2 – Blood oxygen saturation level
Finally, a regression analysis with 6MWD as dependent variable and age, BMI, FEV1, mMRC, CCQ score, presence of depression and anxiety as predictor variable shows poor relationship with variability of 38.41% and only CCQ score was found to have significant influence (with p = 0.008) on 6MWD in patients with stable COPD.
Discussion
The prevalence of depression and anxiety among COPD patients varies widely (12% – 57%) in different studies reported from western countries [3,12,13]. There is paucity of data from Indian subcontinent. However, a summary of some recent publications in this regard is given in [Table/Fig-6] [4–6,14,15]. The frequency of major depressive episodes, panic disorders, substance abuse and other psychiatric problems was found to be significantly higher in COPD patients as compared to healthy adults [15]. In the present study almost two third of the patients of stable COPD were suffering from either depression and/or anxiety. However, it was not related to age, sex distribution, disease severity, smoking history or employment status of the patient. Age and gender were probably not the determinant of depression in COPD because; COPD is a disease of elderly population and there is male predominance in the study population, which is in accordance with other studies from India [5]. The depressed COPD patients had similar BMI, smoking history and lung function status as non-depressed COPD patients but former were more symptomatic with higher CCQ score (p = 0.0003) as evident in other previous studies [7]. However, Negi H et al., found significant association of depression and level of education, occupational status, FEV1, dyspnea and activity level of SGRQ [5]. Waseem SMA et al., found male gender, lower education level, higher socio-economic class and single marital status were associated with more depression whereas female, single, with higher education and higher socio-economic class were found to be more anxious [14].
Summary of different publications from India on mental illness in patients with respiratory diseases.
| Reference | Total number of patients, age range | Study tools | Conclusion |
|---|
| Sajal De, [4]Bhopal, India | 100 COPD, 61.7±9.6 years | PHQ-9 | Overall 72%, stages I, II, III and IV were 83.3%, 56.3%, 72.5% and 86.4%, respectively and prevalence of depression increases with the severity of COPD (p=0.024) |
| Waseem SMAet al., [14]Aligarh, India | 121 COPD patients, 43.15±13.04 yrs | BDI, HAS | 57.02% had depression, 36.37% had anxiety |
| Sharma BB, [6]Jaipur, India | 391 stable chronic respiratory illness, male 37.52±15.11yrs and female 35.85±10.99 yrs | GMHAT/PC interview | Anxiety (20.6%), depression (13.2%) and obsessive compulsive disorders (4.6%) |
| Negi Het al., [5]India | 126 COPD, 62.69±0.84 | PHQ-9 | Overall 49.2%, 20.6% had moderately severe to severe depression or major depressive disorder, 12.7% moderate depression, 15.9% mild depression |
| Chaudhary SC et al. [15]Lucknow, India | 74 COPD, 56.97±10.11 years | MINI version 6.0.0 | Major depressive episodes 2.7%, Panic disorder 4.05%, generalized anxiety disorder 4.4% |
However, there was no significant difference in walk distance between COPD patients with depression and without depression. This may be due to presence of co-existing anxiety in most of them as suggested by Nguyen HQ et al., [16]. Nguyen HQ et al., concluded that the decreased physical activity in COPD patients is associated with depression while anxiety is associated with increased physical activity and that higher level of anxiety lessen the negative effect of depression on physical activity [16]. However, there is difference in opinion regarding association of anxiety with poor exercise performance in stable COPD patients with predominant moderate to severe emphysema [17]. The present study was similar to the findings by Orlandi Lde C et al., who found no association between depression and functional exercise capacity among patients with moderate to severe COPD, though the diagnostic tools were different, namely MINI (Mini International Neuropsychiatric Interview Plus), 6MWT and UULEX (unsupported upper-limb exercise test) [8]. The narrow difference in walk distance among the two subsets of COPD patients in the present study could also be due to the fact that those with more severe depression refused to walk and hence been excluded from the study.
Limitation
There may be factors other than depression and anxiety, related to functional capacity of the COPD patients which has not been considered in the present study like altered walking pattern in the form of intensity, pace and walking variability [18], nutritional status, respiratory and skeletal muscle strength [19], habitual physical activity [20] and level of hypoxemia if any [21].
Conclusion
In the current study, depression and functional exercise capacity in stable COPD patients has more association with high symptom score, rather than demographic profile, employment status or disease severity as assessed by GOLD guideline. Hence all COPD patients who are more symptomatic, irrespective of the GOLD category should be screened for psychiatric symptoms and early initiation of specific therapy may be beneficial for better quality of life.
*Mean±SD
*median value, **Mann-Whitney test and *** 2 Sample t-test
† Significant at Alpha =0.1
*Paired t-test **2 Proportion test ***2 Sample t-test
HR – Heart Rate
RR – Respiratory Rate
SpO2 – Blood oxygen saturation level