Excision Versus Fixation of the Radial Head: A Comparative Study of the Functional Outcomes of the Two Techniques
Sanath Kumar Shetty1, Ashwin Shetty2, Bijith Balan3, Arjun Ballal4, H.Ravindranath Rai5, Anoop Hegde6
1 Assistant Professor, Department of Orthopaedic Surgery, K.S.Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
2 Associate Professor, Department of Orthopaedic Surgery, K.S.Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
3 Postgraduate, Department of Orthopaedic Surgery, K.S.Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
4 Registrar, Department of Orthopaedic Surgery, ARS Hospital, Tirupur, Tamil Nadu, India.
5 Professor and Head, Department of Orthopaedic Surgery, K.S.Hegde Medical Academy, Deralakatte, Mangalore, Karnataka, India.
6 Registrar, Department of Orthopaedic Surgery, ARS Hospital, Tirupur, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arjun Ballal, Registrar, Department of Orthopaedic Surgery, ARS Hospital, Tirupur, Tamil Nadu-641604, India.
E-mail: 5arjunballal@gmail.com
Introduction
The management of displaced and comminuted radial head fractures has been a matter of debate amongst surgeons for many years. Radial head excision formed the mainstay of surgical management of these injuries. Over the years, there have been improvements in the surgical techniques and availability of better implants and instrumentation techniques, hence, open reduction and internal fixation of these fractures is gaining popularity.
Aim
To compare the outcome of elbow function between radial head excision and open reduction and internal fixation of the radial head with mini screws of Mason Type II and Type III radial head fractures and to assess the complications that occur in both techniques.
Materials and Methods
A prospective study was conducted in the Department of Orthopaedic Surgery of Justice K.S.Hegde Charitable hospital. A total of 40 patients between the age group of 30-50 years with Mason Type II and Type III fresh closed radial head fractures were included in the study.
Group I consisted of 20 patients who underwent radial head excision and Group II consisted of 20 patients who underwent open reduction and internal fixation with mini screws. Patients were reviewed at postoperative week 3, 6 and 24. Radiographs were taken and functional outcome assessment of the elbow was done during all the follow ups. Elbow physiotherapy was started on postoperative week three. Scoring of elbow function was done as per the Disabilities of the Arm, Shoulder and Hand (DASH) scoring system. Results were tabulated, compared and analysed statistically using the ‘chi-square test’.
Results
At the end of six months, the patients of the open reduction and internal fixation group had lower DASH scores (4.82±2.73 points) than the radial head excision group (14.23±5.60 points). This inferred that patients who underwent open reduction and internal fixation had better functional outcomes than the excision group. Complications of proximal radial migration was noted in three patients, elbow osteoarthritis was noted in two and periarticular ossification was noted in six patients who underwent radial head excision.
Conclusion
Open reduction and internal fixation of Mason Type II and Type III radial head fractures is a better management technique as compared to radial head excision for management of Mason Type II and III radial head fractures.
Comminuted fractures, DASH scoring system, Mason classification, Mini screws, Periarticular ossification
Introduction
Radial head fractures account for upto 25-44% of all the elbow fractures. Frequency of these injuries has been noted to be higher in women and between the age group of 30-40 years [1]. These injuries were classified on the basis of their severity by Mason in 1954 [2]. He described four types of radial head fractures. Mason Type I included fractures which were undisplaced or minimally displaced. Type II injuries encompassed fractures with displacement, depression or angulation. Type III included comminuted fractures, and type IV included fractures with comminution and elbow dislocation [2]. Historically, the treatment of choice for Mason Type II fractures was radial head excision in case of failure of nonoperative management. Excision of the radial head with or without prosthetic replacement has been the mainstay in the management of Type III fractures. With the advance of better surgical techniques and instrumentation over the years, open reduction and internal fixation of Type II and Type III injuries are gaining popularity [3,4].
For undisplaced radial head fractures (Mason Type I), conservative management, like an above elbow slab or a compression dressing with a sling is the mainstay of therapy [5]. For partial articular displaced fractures like Mason Type II, conservative management was considered a mainstay of management.
Lindenhovius et al., concluded that for long term management of partially displaced radial head fractures open reduction and internal fixation had favourable outcomes but the complication rate was also 44% [6]. Kaas et al., concluded in his nine retrospective series that there was insufficient evidence as to which method of management of radial head fractures was superior [7]. For comminuted radial head fractures, Pearce., and Gallannaugh., reported good results after open reduction and internal fixation of comminuted radial head fractures [8]. Chen et al., concluded that replacement arthroplasty of the radial head had better functional outcomes as compared to the open reduction internal fixation group after two years follow up [9].
To compare the outcome of elbow function between radial head excision and open reduction and internal fixation of the radial head with mini screws of Mason type II and type III radial head fractures and to assess the complications that occur in both techniques.
Materials and Methods
A prospective study was conducted from June 2013 to October 2015 in the Department of Orthopaedic Surgery, Justice K.S. Hegde Charitable Hospital, Mangalore after obtaining clearance from the ethical committee and informed consent from all the patients. A total of 40 diagnosed cases of fresh closed Mason Type II and Type III radial head fractures, between the age groups of 30-50 years were included in the study. Mason Type I and IV fractures were excluded from the study. Skeletally immature patients, pathological fractures, patients with associated ipsilateral upper limb injuries, head injuries and solid organ injuries, patients with systemic complaints like diabetes, hypertension etc., and patient who refused were excluded from the study. Patients with associated osteoarthritis of the elbow, associated neurovascular injuries were excluded from the study. The patients were divided into two groups. The first Group included 20 patients who underwent radial head excision and the second Group included 20 patients who underwent open reduction and internal fixation with mini screws. The patients were explained in detail regarding the advantages and complications of both the techniques taking into consideration, the nature of injury, degree of comminution, financial status of the patients, day to day activities of the patient and professional status etc.
Preoperative antibiotics were started six hours before the surgery after attaining medical fitness. The patient was positioned supine on the fluoroscopic table with elbow in 90 degree flexion and internal rotation of arm and mid pronation of elbow under general anaesthesia or regional block. Surgical exposure for both the techniques employed a Kocher’s approach to the radial head, the interval between extensor carpi ulnaris and anconeus muscle [10–12] [Table/Fig-1] was made.
Intraoperative image showing exposure of the radial head using the Kocher’s approach with excision from right elbow.
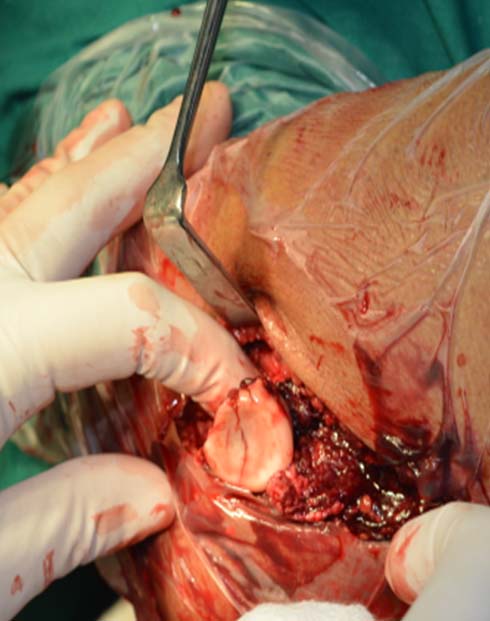
After exposure, the comminuted fragments were removed and using an osteotome the radial head was osteotomised and removed for the patients in the excision group [Table/Fig-1]. In the open reduction and internal fixation group, the fractured fragments were reduced and stabilized with reduction clamps and fixed with mini screws [13] [Table/Fig-2]. At above elbow plaster of paris slab was applied postoperatively and was maintained for three weeks. Intravenous antibiotics were maintained till postoperative day three and then switched over to oral antibiotics till postoperative day six. Suture removal and discharge was done on postoperative day 10.
Intraoperative image showing exposure of the radial head using the Kocher’s approach and fixation with Mini screws.

Antero-posterior and lateral radiographs of the right elbow at postoperative week six after radial head excision.

Reviews were done at weeks 3, 6 and 24. Slab removal and rehabilitation of elbow was started on week three. X-rays were done on all reviews [Table/Fig-3,4]. Range of motion and elbow function was assessed and scored as per the Disabilities of the Arm, Shoulder and Hand (DASH) scoring system [14] during all the reviews. The results were tabulated, compared and analysed statistically using the ‘chi-square test’. The ‘p<0.05’ was considered significant.
Antero-posterior and lateral radiographs of the left elbow at postoperative week six after radial head open reduction and internal fixation with mini screws.

Results
Majority of the patients were between the age group of 30-40 years. A total of 50% of the patients were males and 50% were females. Eighteen patients (45%) presented with Type II Mason radial head fractures and remaining 22 patients (55%) presented with Type III fractures. There was an equal distribution of patients with Mason Type II and Mason Type III fractures in both the excision and the open reduction and internal fixation group.
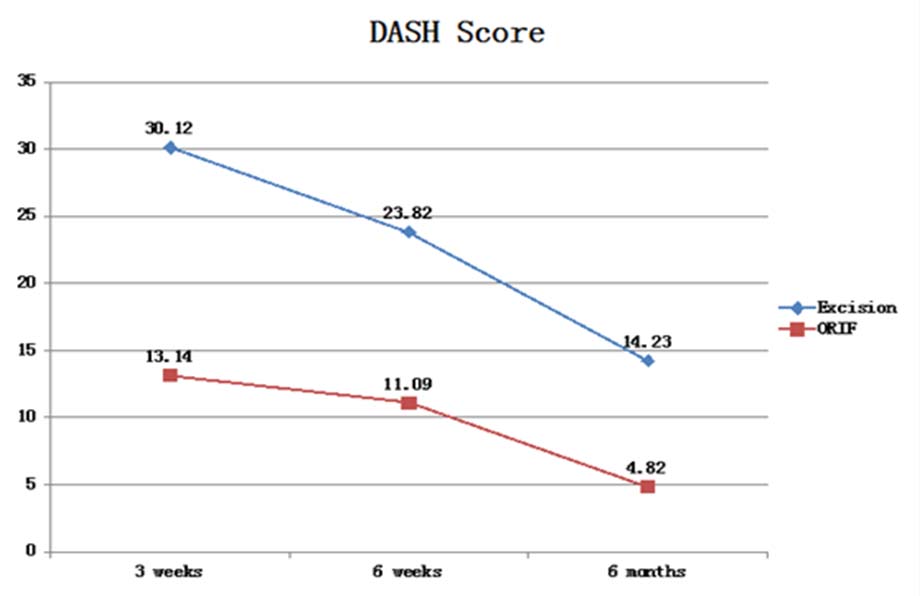
All fractures united at week six. At six months the DASH score was noted to be 14.23±5.60 points for the excision group and 4.82±2.73 points for the open reduction and internal fixation group with a significant ‘p-value’ (p<0.05) [Table/Fig-5].
Line graph showing the DASH score of both the groups during all the reviews. Note that the mean of the open reduction and internal fixation group was lower (13.14 points) than the excision group (30.12 points) during the reviews at post-operative week three and also during the final review at 24 weeks.
Two of the 20 patients who underwent radial head excision were noted to have developed osteoarthritis of the elbow during the final review. Periarticular ossification was noted in six of the 20 patients of the radial head excision group. Three of the 20 patients in the radial head excision group were noted to have proximal radial migration [Table/Fig-6]. One of the 20 patients who underwent open reduction and internal fixation were noted to have early osteoarthritic changes with limitation of motion in the elbow radiographs during the final review [Table/Fig-6].
Table showing the complication rates in Group I and II. Note the complication rates were more in Group I as compared to Group II.
| Complications | Radial head excision (Group I) | Radial head fixation (Group II) |
|---|
| Osteoarthritis | 2 | 1 |
| Periarticular ossification | 6 | 0 |
| Proximal radial migration | 3 | 0 |
| No complications | 9 | 19 |
| Total no. of patients | 20 | 20 |
Discussion
The main modality of management of Mason Type II and Type III fractures in the 1970s was radial head resection whenever conservative management failed [1,2,15]. Reconstruction of the radial head saw the light of day in the 1980s when radial head was published as a secondary stabilizer of the elbow [16]. The 1990s saw the improvement in surgical techniques and instrumentation, hence fixation of radial head gained importance [17]. Few authors reported a sequence of events of lateral elbow instability, increase in carrying angle and chronic strain of medial collateral ligament. These changes led to increase in the incidence of osteoarthritis of the elbow, which lead to worsening of symptoms such as elbow pain, loss of strength, range of motion and also neurovascular symptoms [18]. Several studies reported complications of proximal migration of radius, residual elbow pain, degenerative osteoarthritis and also development of periarticular ossification after radial head excision [2,15,16,19,20].
In our study, on comparison of the DASH scores of elbow function between the open reduction and internal fixation group and the radial head excision group was done at 3, 6 and 24 weeks. We noted that the DASH scores were considerably lower in the open reduction and internal fixation group as compared to the radial head excision group. This showed that patients who underwent open reduction and internal fixation of the radial head had better outcomes in terms of elbow function as compared to the radial head excision group.
These results were comparable to the studies by Zarattini et al., who in their series of 59 patients with isolated Type II Mason’s radial head fractures; 24 of whom who underwent excision and 35 of who underwent open reduction and internal fixation, noted that the dash score was 21.82 points in the excision group and 2.81 points in the open reduction and internal fixation group [21].
Ikeda et al., in their series of 28 patients with Mason Type III radial head fractures of radial head resection versus open reduction and internal fixation, concluded that there was greater loss of strength, range of supination and pronation movements in the radial head resection group as compared to the open reduction and internal fixation group [22].
Twelve(60%) of the 20 patients in the radial head excision group were noted to have proximal radial migration as a complication in the follow up, seven of who were symptomatic. Six (30%) of the twenty patients developed osteoarthritis of the elbow, periarticular ossification was noted in six (30%) of the 20 patients in the radial head excision group. These results are comparable to those of mikic and colleagues who reported proximal radial migration in 47% of their patients, osteoarthritis in 52% of the patients and periarticular ossification in 57% of the patients [21].
Khalfayan et al., reported a good to excellent outcome of elbow function in 90% of the patients in their series after open reduction and internal fixation of radial head [4]. Ring and colleagues reported a success rate of 93% of excellent results after open reduction and internal fixation of radial head [16].
Limitation
The sample size of the study was small, only 20 patients per group. The follow up was limited only for only 24 weeks. Longer follow up would be required. Longer follow up could not be accomplished as many patients did not turn up after 24 weeks as they were from distant places from the hospital.
Conclusion
Open reduction and internal fixation of Mason Type II and Type III radial head fractures have better functional outcome and reduced complication rates as compared to radial head excision. Hence, radial head fixation is a better technique of management of Type Mason II and III radial head fractures.
[1]. Karlsson KM, Herbertsson P, Nordqvist A, Besjakov J, Josefsson OP, Hasserius R, Comminuted fractures of the radial head, Favourable outcome after 15–25 years of follow up in 19 patientsActa Orthop 2010 81(2):224-27. [Google Scholar]
[2]. Mason ML, Some observations on fracture of the head of the radius with a review of one hundred casesBr J Surg 1954 42:123-32. [Google Scholar]
[3]. Miller G, Humadi A, Unni R, Hau R, Surgical management of mason type III radial head fracturesIndian J Orthop 2013 47(4):323-32. [Google Scholar]
[4]. Khalfayan EE, Culp RW, Alexander AH, Mason type II radial head fractures: operative versus non operative treatmentJ Orthop Trauma 1992 6(3):283-89. [Google Scholar]
[5]. Mahmoud SS, Moideen AN, Kotwal R, Mohanty K, Management of mason type 1 radial head fractures: a regional survey and a review of literatureEur J Orthop Surg Traumatol 2014 24(7):1133-37. [Google Scholar]
[6]. Lindenhovius AL, Felsch Q, Ring D, Kloen P, The long-term outcome of open reduction and internal fixation of stable displaced isolated partial articular fractures of the radial headJ Trauma 2009 67(1):143-46. [Google Scholar]
[7]. Kaas L, Struijs PA, Ring D, van Dijk CN, Eygendaal D, Treatment of Mason type II radial head fractures without associated fractures or elbow dislocation: a systematic reviewJ Hand Surg Am 2012 37(7):1416-21. [Google Scholar]
[8]. Pearce MS, Gallannaugh SC, Mason type II radial head fractures fixed with Herbert bone screwsJ R Soc Med 1996 89(6):340P-44P. [Google Scholar]
[9]. Chen X, Wang SC, Cao LH, Yang GQ, Li M, Su JC, Comparison between radial head replacement and open reduction and internal fixation in clinical treatment of unstable, multifragmented radial head fracturesInt Orthop 2011 35(7):1071-76. [Google Scholar]
[10]. Hall JA, McKee MD, Posterolateral rotatory instability of the elbow following radial head resectionJ Bone Joint Surg Am 2005 87:1571-79. [Google Scholar]
[11]. Adams JE, Steinmann SP, Nerve injuries about the elbowJ Hand Surg [Am] 2006 31:303-13. [Google Scholar]
[12]. Diliberti T, Botte MJ, Abrams RA, Anatomical considerations regarding the posterior interosseous nerve during posterolateral approaches to the proximal part of the radiusJ Bone Joint Surg Am 2000 82:809-13. [Google Scholar]
[13]. Perez AE, Fractures of the shoulder, arm and forearmCampbell’s Operative Orthopaedics 2013 12(3):2871-72. [Google Scholar]
[14]. Hudak PL, Amadio PC, Bombardier C, Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The upper extremity collaborative group (UECG)Am J Ind Med 1996 29(6):602-08. [Google Scholar]
[15]. Morrey BF, Radial head fractureIn: The elbow and its disorders. Morrey BF. (ed.) 1993 PhiladelphiaW.B. Saunders:383-404. [Google Scholar]
[16]. Ring D, Jupiter JB, Monteggia fractures in adultsJ Bone Joint Surg 1998 80:1733-44. [Google Scholar]
[17]. Morrey BF, Askew L, Chao EY, Silastic prosthetic replacement for the radial headJ Bone Joint Surg 1981 63:454-58. [Google Scholar]
[18]. Kleinman WB, Stability of the distal radioulna joint: biomechanics, pathophysiology, physical diagnosis, and restoration of function what we have learned in 25 yearsThe J hand surg Am 2007 32(7):1086-106. [Google Scholar]
[19]. Hotchkiss RN, Displaced fractures of the radial head: Internal fixation or excision?J Am Acad Orthop Surg 1997 5:1-10. [Google Scholar]
[20]. Morrey BF, Instructional course lectures, the american academy of orthopaedic surgeons. Current concepts in the treatment of fractures of the radial head, the olecranon, and the coronoidJ Bone Joint Surg 1995 77-A2:316-27. [Google Scholar]
[21]. Zarattini G, Galli S, Marchese M, Di Mascio L, Pazzaglia UE, The surgical treatment of isolated Mason type 2 fractures of the radial head in adults: comparison between radial head resection and open reduction and internal fixationJ Orthop Trauma 2012 26:229-35. [Google Scholar]
[22]. Ikeda M, Sugiyama K, Kang C, Takagaki T, Oka Y, Comminuted fractures of the radial head. Comparison of resection and internal fixationJ Bone Joint Surg Am 2006 87:76-84. [Google Scholar]