Pseudoangiomatous Stromal Hyperplasia: A Rare Cause of Breast Lump in a Premenopausal Female
Zeeshan Kareem1, Sandhya Iyer2, Mansha Singh3
1 Registrar, Department of General Surgery, Lokmanya Tilak Municipal Medical College and Sion Hospital, Mumbai, Maharashtra, India.
2 Associate Professor, Department of General Surgery, Lokmanya Tilak Municipal Medical College and Sion Hospital, Mumbai, Maharashtra, India.
3 Assistant Professor, Department of General Surgery, Lokmanya Tilak Municipal Medical College and Sion Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Zeeshan Kareem, Registrar, Department of General Surgery, 1st Floor, College Building, LTMMC and Sion Hospital, Sion, Mumbai-400022, Maharashtra, India.
E-mail: zeeshankareem570@gmail.com
Pseudoangiomatous Stromal Hyperplasia (PASH) of the breast is a rare benign proliferating breast condition. We report a case of a 26-year-old female who was being worked up for infertility and was incidentally noted to have a well defined lump in the left breast. Fine Needle Aspiration Cytology (FNAC) and core needle biopsy of the lump were suggestive of benign breast disease. Patient underwent excision of the lump. Histopathology report of which was suggestive of PASH of the breast.
Benign breast disease, Chocolate cysts Endometriona
Case Report
A 26-year-old female presented to the gynaecology Outpatient Department (OPD) with complaint of infertility. She was admitted and was being worked up for the same. Incidentally, a left breast lump was found for which she was referred to surgery OPD. Patient gave a history of lump being present since one year, which had gradually increased in size. She did not have any family history of similar lump in breast. She was married since three years and had not conceived till presentation. Patient gave history of irregular menstrual cycle associated with pain in abdomen on and off since four years. Magnetic Resonance Imaging (MRI) pelvis was done which was suggestive of bilateral multicystic ovarian lesion with haemorrhage within-chocolate cysts/endometriomas.
On examination, a well defined lump of around 10 cm x 8 cm x 6 cm size was palpable in the left breast below the nipple areola complex. It was mobile, firm and non tender on palpation. Patient did not have any axillary lymphadenopathy. Rest of the physical examination were unremarkable. Provisional diagnosis on clinical examination was either a giant fibroadenoma or a phylloides tumour.
On investigation, biochemical parameters were within normal limits. Ultrasonography (USG) of left breast showed a large, oval, hypoechoic lesion measuring 12.8 cm x 4.9 cm in size, wider than taller with smooth margins, in upper outer quadrant of right breast. It appeared benign.
Core needle biopsy of the lump was performed and the histopathology report showed few benign acini in sclerosed stroma, suggestive of benign breast tissue.
Patient underwent wide local excision of the lump using an inframammary incision [Table/Fig-1], which revealed a 15 cm x 12 cm x 6 cm well encapsulated, smooth lump, with regular margins, weighing 600 grams in the left breast [Table/Fig-2]. Procedure was uneventful, subcutaneous drain was placed after closure, and patient was discharged after removal of subcutaneous drain after three days.
Intraoperative Picture of lump being excised using an inframammary incision (left);

The lump, as seen after excision, measuring 15x12x6cm, and weighing 600 grams (middle);

Patient was regularly followed up after excision for six months and had no significant complaints. Histopathology, report of the lump revealed mammary hamartoma with PASH with no evidence of malignancy [Table/Fig-3,4 and 5].
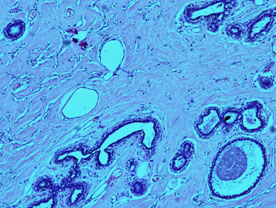
Histopathology slide showing the characteristic growth pattern of inter-anastomosing, angulated, slit like, empty channels separated by dense, keloid-like, wavy, acellular collagenous stroma (right).
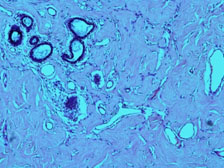
Histopathological slide of PASH.
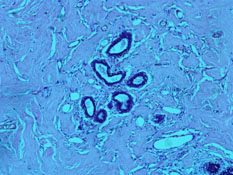
Stromal fibrotic proliferation with anastomosing slit-like pseudovascular spaces, that is lined with spindle cells.
Discussion
PASH of the breast is a rare condition typically found incidentally. It typically occurs in pre-menopausal women but is also reported to be found in 24-47% of men with gynaecomastia [1]. Histologically, it resembles a low grade angiosarcoma or a phylloides tumour, from which it needs to be differentiated. Most of the patients are asymptomatic and are found to have a palpable, mobile, firm, painless lump in the breast while presenting with some other chief complaint, as in this case.
The differential diagnosis include fibroadenoma, especially in a young patient and a phylloides tumour in older women [2]. On USG, PASH tends to be an oval, round hypoechoic mass or can present as a heterogeneous mass with cystic areas [3]. On mammography, it most commonly shows a well defined, uncalcified mass with regular borders and margins [3]. MRI of the breast can also be performed, as it gives a precise determination of the extent of disease, including the presence of multifocal or multicentric disease [4].
FNAC is often inconclusive, and core needle biopsy is needed to diagnose this condition, although in some cases, diagnosis is made only after excision. It is histologically defined as a complex network of slit-like spaces lined by endothelial-like spindle cells against a background of stromal hyperplasia [5]. On immunohistochemistry, it is positive for CD34 and vimentin and negative for Factor VIII-related antigen and cytokeratin [6].
Treatment is usually surgical, although non-surgical management has also been reported in selected cases. If the diagnosis of PASH is made on core biopsy or if lesion is less than 2 cm, surgical excision may not be indicated and close observation with serial mammography to assess interval growth is adequate treatment [7]. However, if the diagnosis is still doubtful after biopsy, then wide local excision is the treatment of choice for such patients. The recurrence rate is reported to be 15-22% [5].
Conclusion
PASH of the breast is a rare, benign proliferative disease, found in pre-menopausal women. It is incidentally found, as seen in our case. It has overlapping clinical, radiologic and cytologic features with fibroadenoma. FNAC and core needle biopsy might not be diagnostic, and excision might be required in such cases to confirm the diagnosis, and exclude malignancy, as was done in this case.
[1]. Jaunoo SS, Thrush S, Dunn P, Pseudoangiomatous stromal hyperplasia (PASH): A brief reviewInt J Surg [Internet] 2011 9(1):20-22. [Google Scholar]
[2]. Abdull Gaffar B, Pseudoangiomatous stromal hyperplasia of the breastArch Pathol Lab Med 2009 133(8):1335-38. [Google Scholar]
[3]. Vo QD, Koch G, Girard JM, Zamora L, Bouquet de Jolinière J, Khomsi F, A Case Report: Pseudoangiomatous Stromal Hyperplasia Tumor Presenting as a Palpable MassFront Surg [Internet] 2016 2:5-8. [Google Scholar]
[4]. Mai C, Rombaut B, Hertveldt K, Claikens B, Van Wettere P, Diffuse pseudoangiomatous stromal hyperplasia of the breast: a case report and a review of the radiological characteristicsJBR-BTR 2014 97(2):81-83. [Google Scholar]
[5]. Almohawes E, Khoumais N, Arafah M, Pseudoangiomatous stromal hyperplasia of the breast: A case report of a 12-year-old girlRadiol Case Reports [Internet] 2015 10(3):1-4. [Google Scholar]
[6]. Masannat Y, Whitehead S, Hawley I, Apthorp L, Shah EF, Pseudoangiomatous stromal hyperplasia: A case reportCase Rep Med [Internet] 2010 2010:549643 [Google Scholar]
[7]. Ding X, Boney-montoya J, Owen BM, Bookout AL, Coate C, Mangelsdorf DJ, NIH Public Access 2013 16(3):387-93. [Google Scholar]