Reducing the intensity of labour pain is a way of encouraging women to go for normal vaginal delivery [1]. Labour pain is one of the acute feelings and sufferings experienced by humans. Studies have shown that 77% of mothers suffered severe and intolerable labour pain [2]. Fear of a natural, normal labour pain makes women to opt for the easier, painless caesarean delivery [3]. Labour pain and its intensity is not the same for all women. Several factors including individual expectations of pain relief, anxiety, past experiences and age affects labour pain. These factors may enhance or reduce the mother’s feeling of pain and tolerance [4].
In nulliparous women, the intensity of labour pain is higher than multiparous women [4]. Moreover, prolonged and severe vaginal delivery may be harmful for foetus and mother as well [5]. Severe pain diminishes the mother’s psychological and physical control while increasing her hyperventilation and catecholamine level. It reduces placental perfusion and leads to foetal distress [6].
According to a statement from the Association of American Anaesthesiologists and Gynaecologists, during delivery, women should have access to effective pain relief [7]. Safe procedures for pain relief during labour should not distract natural labour process, physiological functions or the mothers’ consciousness [8]. Several methods have been employed for reducing labour pain such as: entonox, epidural-spinal anaesthesia and Transcutaneous Electrical Nerve Stimulation (TENS) [9–11]. However, TENS is more effective on relieving back pain and dysmenorrhea than labour pain [11–13].
Entonox gas is a combination of 50% nitrous oxide and 50% oxygen providing the inhalational analgesia. entonox is an appropriate anaesthetic method used in delivery. Advantages of this method are fast effective, rapid secretion from the body, user friendly for mother and cost effectiveness. As for the cons, the disadvantages or complications of entonox are dry mouths, vertigo, lethargy, vomiting and uncomfortable feeling, in a word, the uneasiness [9]. Although epidural-spinal anaesthesia is a more efficient way in reducing labour pain than entonox [10] a high rate of approval and satisfaction among mothers and low neonatal complications have been reported after entonox applications [14].
Because self-administrated entonox inhalation was used, the depth of breathing and the amount of gas used could not be evaluated. In addition, woman’s sense of being able to control pain may not only be related to the usage of entonox but also to control herself [15]. Some studies have not shown significant difference between using inhaling oxygen and entonox in reduction of labour pain [13,16]. Application of entonox during labour pain could be a step towards the campaign for natural vaginal delivery because women’s trend and tendency to undergoing CS is high in Iran. The CS rate rose linearly with age of Iranian mothers in urban areas (from 26.0% to 43.4% for ages 15–44 years) [17]. While, according to World Health Organization the rate of CS should decrease to 10-15% of all child births in developing countries [18]. Therefore, pregnant mothers need to use suitable analgesia during labour pain to decrease the rate of CS and should not undergo CS without clinical or medical reasons. This study investigated the effectiveness of entonox on pain relief and the duration of labour in nulliparous women.
Materials and Methods
A clinical controlled trial study was conducted among 120 nulliparous women (60 in intervention and 60 in control group). This study was done in labour units of Atieh Hospital, Hamadan, Iran, in year 2015. The women were selected randomly to receive either entonox (pre-prepared mixture of nitrous oxide and oxygen) or only oxygen. They were selected based on a convenient sampling method and were randomly allocated into intervention and control groups. The allocation sequence was determined by one of the members of the research team, not involved in the sample selection, using a four-block randomized design. The participants were randomly assigned to the intervention and control group with a ratio of 1:1. The codes related to each woman were specified in envelopes in order not to expose the assignment procedure. Thus, the subjects were in A and B group according to the specified sequence [Table/Fig-1]. The data analyzer was not aware of the interventions provided to the groups.
Flow diagram of the participants
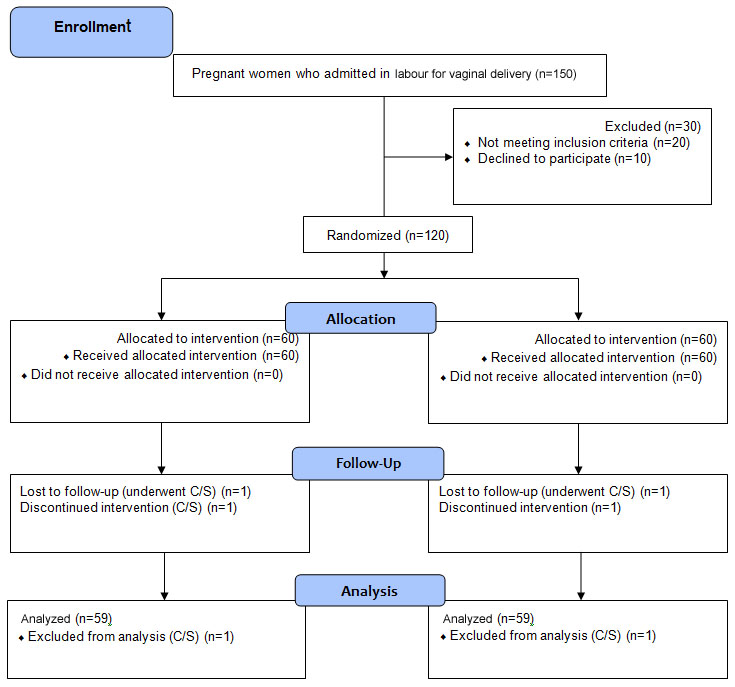
Inclusion criteria were, nulliparous, spontaneous active phase (cervical dilatation 3-4 cm and effacement of 40-50%). The exclusion criteria were: medical problems in foetus or mother, administration of oxytocin, narcotics and sedatives. Informed consent forms were obtained. A basic demonstration was presented to mothers for the use of masks during uterine contractions.
In active phase of labour, pain intensity was analyzed in both groups using the VAS values. Women were asked to rate their pain intensity on scale of 0 to 10 during their labour pain. Martensson L and Bergh I have confirmed the effect of VAS changes score in labour pain [19].
In two groups gas-inhalations were introduced from the active phase of the first stage of labour (cervical dilatation 3-4 cm and effacement of 40-50%) up to the delivery of newborn (end of second stage of labour). ENTONOX® cylinders made by BOC health care factory were used. They were supplied to the following specification: oxygen 50.0%±2.0%; nitrous oxide 50.0%±2.0%. The medical oxygen specification and the nitrous oxide specification compile with the current European Pharmacopeia Monograph [20].
In the intervention group, entonox gas inhalation was released at the onset of pain and with each contraction in labour room. The self-usage of entonox gas was done via a face-mask. The entonox administration continued uptil the end of contraction pain and after this period the woman breathed room air as normal [21]. The monitoring of contraction frequency and intensity, foetal heart rate, and mother’s physical signs (blood pressure, pulse, and temperature and breath rate) were done as routine for both groups by midwifery personnel’s. For the control group in labour room, only oxygen gas inhalation was initiated at the onset of pain with each contraction. Women were unaware of the nature of the gas inhaled however, the researcher was not blinded for the type of gas inhalation used. Thus, the single-blind study was carried out. Women’s Blood Pressure (BP), pain severity, pain duration (hours) and duration of labour was compared in two groups.
Statistical Analysis
Using SPSS version 20.0 data analysis was done. The descriptive statistics, chi-square test, independent t-test were used. The significant level was set at p<0.05.
Results
The mean age of women was 25.69 (SD=4.83). About 91% were housewives and remaining 9% were employed. Sixty percent had completed high school education level and 21% had college education. No significant differences were observed between the two groups in relation to mother’s age, gestational age, Body Mass Index (BMI) and neonatal weight [Table/Fig-2].
Comparisons of characteristics between two groups.
| Characteristics | EntonoxMean±SD | ControlMean±SD | t | p-value |
|---|
| Age | 26.10±5.24 | 25.27±4.40 | 0.95 | 0.347 |
| Gestational age | 39.54±2.93 | 40.37±5.44 | 1.04 | 0.301 |
| BMI | 25.46±2.43 | 25.15±2.66 | 0.68 | 0.501 |
| Neonatal weight | 3183.61±427.66 | 3115.83±403.85 | 0.90 | 0.372 |
[Table/Fig-3] reveals significant differences between two groups on labour pain using VAS values at the first, second, third and fourth hours after intervention (p<0.05). Mean and standard deviation of duration of labour in the intervention group (64.80±25.60 minutes) was significantly shorter than that of the control group (98.33±26.88 minutes) (p<0.001).
Comparison of pain and duration of labour stage in two groups.
| Characteristics | EntonoxMean±SD | ControlMean±SD | t | p-value |
|---|
| Pain in first hour | 5.95±1.32 | 8.45±1.02 | -11.65 | <0.001 |
| Pain in second hour | 5.44±1.94 | 8.12±2.16 | -7.17 | <0.001 |
| Pain in third hour | 1.26±2.48 | 6.27±4.20 | -7.99 | <0.001 |
| Pain in fourth hour | 0.28±1.25 | 1.88±3.80 | -3.13 | 0.002 |
| Duration of first stage | 64.80±25.60 | 98.33±26.88 | -6.44 | <0.001 |
| Duration of second stage | 44.26±21.09 | 64.25±30.14 | -4.23 | <0.001 |
In this study, the pain relief therapy did not have any effect on decreasing the rate of CS. In the entonox group one mother and in the oxygen group another mother underwent the CS; the rest of the mothers had done normal vaginal delivery. There were no significant differences between two groups on women’s blood pressure and neonatal Apgar score (p>0.05). Nausea was reported more in the intervention group than that of the control group (p<0.05) [Table/Fig-4].
Comparisons of side effects in two groups.
| Side-effects | EntonoxN (%) | ControlN (%) | Chi-square | p-value |
|---|
| Nausea | 36 (59.0%) | 2 (3.3%) | 43.50 | <0.001 |
| Vomiting | 15 (24.6%) | 7 (11.7%) | 3.40 | 0.650 |
| Lethargy | 3 (4.9%) | 4 (6.7%) | 0.17 | 0.680 |
| Dry of mouth | 13 (21.3%) | 10 (16.7%) | 0.40 | 0.520 |
Discussion
This study indicated the pain relief effect of entonox during active phase of labour. Similarly, Jafarzadeh L et al., studied the effect of entonox in pain relief in 60 Iranian women (30 women in each case and control group). They found that the mean of pain scores in case group was 3.98±2.7 and 5.60±3.8 for control group (p=0.03) [22]. Masoudi M et al., compared the effect of entonox and warm water for pain relief during labour. They found that the pain scores in entonox group was significantly lower than warm water group {4.32±1.65 vs. 6.43±2.06 (p<0.05), respectively} [23]. In another study among 60 women, researchers found that the mean for labour pain intensity decreased significantly after the usage of entonox compared to the control group (p<0.001) [24].
Bergeret S et al., investigated the effect of five non-epidural methods on labour pain among 177 pregnant women. The pain relief methods were: Nitrous oxide/oxygen inhalation (N2O), Nalbuphine (NAL), Sufentanil (SUF), Pethidine (PET), and Spinal Analgesia (SA). The choice of the method was in agreement with the choice of midwives/anaesthetists and as per the cervical dilation. The SA group demonstrated more relief as compared to the other groups during the treatment. No significant differences in pain relief were reported between the four groups (SUF, NAL, PET, N2O). Maternal satisfaction was higher in the SA, SUF and N2O groups than those of the PET and NAL groups. The most observed maternal side effects were maternal sedation in the NAL group and pruritus in the SA group. The infant’s side effects such as respiratory problems were unrelated with the analgesic method [25].
In this study, the first and second stage of labour was shorter in entonox users compared with those of the oxygen group. Similarly, in Jafarzadeh L et al., study duration of first stage of labour in entonox users was shorter than control group (3.9±2.7 vs. 5.6±3.8 (p<0.001) [22]. In study of Masoudi M et al., the cervical dilatation in entonox group was higher than warm water group (7.52±2.32 vs. 5.86±2.04 (p<0.05), respectively) [23].
In the current research, no essential or significant variance was obtained in any of the two groups including for the rate of the caesarean, maternal blood pressure, maternal heart rate, foetal heart rate and Apgar scores. Other studies also found no significant changes on mother/foetus vital signs in entonox users [21–26]. Yazdi Moghaddam H et al., investigated and probed the effect of entonox gas on the Apgar of neonates in 270 pregnant women hospitalised at the labour ward in Sabzevar, Iran. They found no significant differences between the two groups in age, gestational age of pregnancy, labour induction methods. Moreover, Apgar scores of entonox group at first, fifth and 20th minutes postpartum were significantly higher than control group [26].
Outcome of this study showed that 97% women in both groups had normal vaginal delivery. Therefore, the present study did not show difference between two groups on the CS rate. Previous study also showed that fewer patients in the entonox group required CS compared with the control group but the difference was not significant (p=0.52) [24].
In current study, 85% of mothers showed their content in using entonox inhalation as a pain reliever. In other researches respectively 60% to 78.2% of mothers were also satisfied with inhaling entonox for the reduction of the labour pain [9,16]. Also, McNeill JA et al., revealed that mothers who used entonox had also successfully passed the vaginal delivery pain [27].
Side effects of entonox may include light-headedness, dry mouth and tingling feeling around the fingers (due to hyperventilation) [21]. Since in current study, each midwife supervising the use of entonox was skilled, informed and mature enough to instruct its administration, the unpleasant side effects were avoided by rhythmic, steady breathing and adequate hydration after use. In the present study, only nausea in entonox group was more compared to the control group. Similarly, in a previous study nausea was reported in the intervention group more than the control group [22].
Previous studies suggested training and exercising to be a necessity for pregnant mothers to choose normal delivery rather than the CS [3,24]. To encourage mothers for normal delivery, they should become aware of the advantages of vaginal delivery inducing hormones’ secretion which are useful for both the mother and the child while at the same time reducing the post-term complications such as breast feeding disorders [25,28,29]. The main reason for opting for caesarean was fear of labour pain and the most doubtful reason to use analgesia during labour was the fear of complications albeit the uninformative grounds [3,30].
Physicians and midwives may provide training classes and educational brochures to increase awareness of pregnant women towards the benefits of the normal birth delivery. Also, providing the appropriate protocols for usage of appropriate analgesia during labour in public and private delivery care centers could be important for promoting mother and neonatal welfare and health.
Limitation
The study results may be limited by convenience sampling, the number of participants, self-reporting of pain score, self-reporting of side effects and medical conditions which have not been diagnosed changing the effectiveness of the entonox. This study was conducted in one hospital and hence, as such inapplicable in all cases and not observed as a founded source implementable in other hospitals. As we introduced entonox during labour pain (less than 10 hours), the blood cell counts were not performed, if treatment exceeds four days, twice weekly blood cell counts should be performed looking for evidence of megaloblastic changes in red cells or hypersegmentation of neutrophils.
Conclusion
Entonox consumption showed pain relief in women during first and second stages of labour and a decrease in the length of their labour. No significant reported complication of entonox was an advantage of this analgesic method. Therefore, to decrease labour pain, entonox inhalation analgesia is useful.