A Giant Cutaneous Horn Projecting from Verrucous Carcinoma of Buccal Mucosa: A Rare Case Report
Priyankar Singh1, Dipesh Nathani2, Shashi Ranjan3, Rashmi Issar4
1 Senior Resident, Department of Dentistry, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
2 Private Practitioner, Dr Nathani’s Dentofacial CareSurat, Gujarat, India.
3 Reader, Department of Oral and Maxillofacial Pathology, Dr B.R.Ambedkar Institute of Dental Sciences and Hospital, Patna, Bihar, India.
4 Reader, Department of Conservative Dentistry and Endodontics, Patna Dental College and Hospital, Patna, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyankar Singh, Senior Resident, Oral and Maxillofacial Surgery, Department of Dentistry, Indira Gandhi Institute of Medical Sciences, Patna-800014, Bihar, India.
E-mail: spriyankar@yahoo.co.in
Cutaneous horn is conical shape of compact keratin that resembles a miniature animal horn. Though morphologically similar to horns in animals they are histologically very different from them. It is a circumscribed, conical, hyperkeratotic dense protrusion with epithelial cornification above the skin surface in response to a wide range of underlying benign and malignant pathological changes. Though benign, a cutaneous horn holds the potential to be premalignant or malignant. In India till now six cases has been reported with cutaneous horn at various unusual sites. We report a unique case of 52-year-old woman with a giant cutaneous horn at left oral commissure with underlying verrucous carcinoma of left buccal mucosa which is a very rare location for such lesion. Considering its malignant potential, adequate therapy requires wide excision with a tumour-free margin of at least 1 cm, particularly in the facial region where the incidence of malignancy is higher.
Habits, Keratin Mass, Premalignant
Case Report
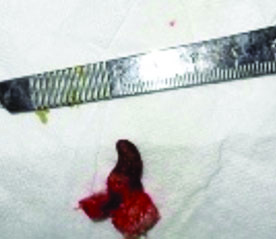
A 52-year-old female reported with complaint of a horn like conical asymptomatic lesion at left corner of mouth. The lesion had been present for last three years and it gradually increased in size despite the patient having cut off its tip many times. Patient also complained of a rough lesion in left cheek mucosa inside mouth which was present from last one year and gradually progressive. A history of betel nut chewing and smoking was noted for the past 10 years. On examination, an isolated, hard and well circumscribed, brownish grey coloured, conical keratinized lesion measuring 3 cm x 1 cm was present over left oral commissure [Table/Fig-1]. Base of the lesion showed crusting and mild purulent discharge. Intraoral examination showed a 4 cm x 2 cm rough velvety proliferative ulcerated growth over the left buccal mucosa extending posteriorly from the left oral commissure [Table/Fig-2]. Neck examination was suggestive of level I and level II cervical lymphadenopathy on left side. Routine blood investigations were within normal limits. The patient initially insisted only for cosmetic removal of the lesion and an incisional biopsy was done involving the cutaneous horn and a deep wedge shaped buccal mucosa at left commissure of lip [Table/Fig-3].
Cutaneous horn at lip commissure.

Lesion in buccal mucosa at base of horn.

Incisional biopsy specimen.
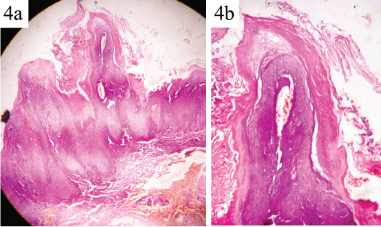
The histopathological reports showed exophytic as well as endophytic proliferation of hyperparakeratinized stratified squamous epithelium with maturing keratinocytes and broad rete pegs with irregular stromal penetration. Surface cleft was plugged with parakeratin. Stroma was fibrovascular and showed chronic inflammatory infiltrates and blood vessels. Pseudo epithelial hyperplasias were seen at places. The findings were consistent with verrucous variant of squamous cell carcinoma. The patient was later convinced and under general anaesthesia a wide local excision of the buccal mucosa growth taking 1 cm margin with supra omohyoid neck dissection of the left cervical nodes was done. Postoperative period was uneventful. Histopathological examination of the surgical specimen showed features consistent with verrucous carcinoma of buccal mucosa [Table/Fig-4a,b]. At follow up patient reported with no fresh complains and wound healing was satisfactory. Patient has been asked to report at every six months for follow up.
Exophytic and endophytic proliferation of para keratinized epithelium with pushing rete pegs covering inflamed storm suggestive of verrucous carcinoma (H&E; 10X).
Discussion
Cutaneous horn is a bulging mass of keratin and is also called as cornu cutaneum [1]. It presents itself as a circumscribed, conical, hyperkeratotic dense protrusion with epithelial cornification above the skin surface simulating the horn of an animal, in response to a wide range of underlying benign and malignant pathological changes [2]. Though, it was first reported in 1588 in an elderly Welsh woman in London, its earliest observations in humans were described by the London surgeon Everard Home in 1791 [3]. It actually results from the extension of another lesion, such as a wart, seborrheic keratosis, actinic keratosis, dermatofibroma, keratoacanthoma, or carcinoma (including basal and squamous cell cancers) [4]. The horn occurs commonly in sun exposed areas or areas prone to actinic radiation, like ears, face, scalp, arms, and dorsal hands but can also occur in areas not exposed to sunlight like penis, lower lip mucosa and nasal vestibule [5]. Cutaneous horn is usually thick, firm, and pedunculated and its shape can vary from straight to curved and twisted. Its size may range from a few millimetres to several centimetres in length and colour from white or yellow to brown or black. Larger lesions can be traumatized, resulting in pain and bleeding. [6,7]. Though benign, a cutaneous horn holds the potential to be premalignant or malignant. An increased risk of malignancy is noted if the lesion is tender at the base, larger in size, occurring in an older individual, or occurring in a patient with other cancerous lesions [8].
The major risk factor for malignancy is the underlying condition which may be benign or malignant rather than the horn itself [9]. A histopathological study estimated the frequency to be 0.3-1.3%. In the two largest published series, which 38.9% and 74.6% of cases respectively were derived from malignant and benign lesions [10]. Souza LN reported another large study which included 230 cutaneous horns reported 58% of either premalignant or malignant changes at their base [11,12]. Spira J and Rabinovitz H concluded that cutaneous horns in association with a malignant or premalignant base are more common in patients with a history of other malignant or premalignant lesions [13].
Though morphologically similar to horns in animals human horns are histologically very different as they are not composed of superficial hyperkeratotic epidermis, dermis, and centrally positioned bone as seen in animal horns [14]. In past, nine cases of cutaneous horn over the lip have been reported and three of these had an associated squamous cell carcinoma at its base [8,9,15]. In India till now six cases have been reported with cutaneous horn at various unusual sites [1,16–19]. Due to frequent association of malignant or premalignant changes at the base, cryosurgery is not suggested for the treatment of cutaneous horns as it doesn’t ensure full thickness excision of the tumour and also is not appropriate for the treatment of squamous cell carcinomas. Therefore, adequate therapy requires wide excision with a tumour-free margin of at least 1 cm, particularly in the facial region where the incidence of malignancy is higher [20].
Conclusion
To conclude we would say that these lesions need to be managed carefully due to the high incidence of malignant histopathological changes.
Author Contributions
First and second author operated the case and formed the base of manuscript; third author did the histological analysis and helped in reviewing the manuscript; fourth author is an endodontist and the case reported at her clinic. She also assisted us in regular follow up of the patient and preparing and editing of the manuscript.
[1]. Kumar S, Bijalwan P, Saini SK, Carcinoma buccal mucosa underlying a giant cutaneous horn: a case report and review of the literatureCase Rep Oncol Med 2014 2014:518372 [Google Scholar]
[2]. Gould JW, Brodell RT, Giant cutaneous horn associated with verruca vulgarisCutis 1999 64(2):111-12. [Google Scholar]
[3]. Bondeson J, Everard Home, John Hunter. Cutaneous horns: A historical reviewAm J Dermatopathol 2001 23(4):362-69. [Google Scholar]
[4]. Leelavathy B, Kemparaj T, Sathish S, Khadri SIS, Squamous cell carcinoma arising from a giant cutaneous horn: a rare presentationIndian J Dermatol 2015 60(1):107 [Google Scholar]
[5]. Mutaf M, A rare perioral lesion: Cutaneous horn of the lower lipEur J Plast Surg 2007 29:339-41. [Google Scholar]
[6]. Nthumba PM, Giant cutaneous horn in an African woman: a case reportJournal of Medical Case Reports 2007 1:170 [Google Scholar]
[7]. Copcu E, Sivrioglu N, Culhaci N, Cutaneous horns: are these lesions as innocent as they seem to be?World J Surg Oncol 2004 2:18 [Google Scholar]
[8]. Skoulakis C, Theos E, Chlopsidis P, Manios AG, Feritsean A, Papadakis CE, Giant cutaneous horn on squamous cell carcinoma of the lower lipEur J Plast Surg 2009 32:257-59. [Google Scholar]
[9]. Popadi M, Squamous cell carcinoma presenting as a giant cutaneous horn of the lower lipIndian J Dermatol Venereol Leprol 2014 80:74-76. [Google Scholar]
[10]. Yu RC, Pryce DW, Macfarlane AW, Stewart TW, A histopathological study of 643 cutaneous hornsBr J Dermatol 1991 124:449-52. [Google Scholar]
[11]. Souza LN, Martins CR, de Paula AM, Cutaneous horn occurring on the lip of a childInt J Paediatr Dent 2003 13:365-67. [Google Scholar]
[12]. Thappa M, Laxmisha C, Cutaneous horn of eyelidIndian Pediatr 2004 41:195 [Google Scholar]
[13]. Spira J, Rabinovitz H, Cutaneous horn present for two monthsDermatol Online J 2000 6:11 [Google Scholar]
[14]. Michal M, Bisceglia M, Di Mattia A, Requena L, Fanburg-Smith JC, Mukensnabl P, Gigantic cutaneous horns of the scalp: lesions with a gross similarity to the horns of animals: a report of four casesAm J Surg Pathol 2002 26(6):789-94. [Google Scholar]
[15]. Pinto-Almeida T, Oliveira A, da Cunha Velho G, Alves R, Caetano M, Selores M, Giant cutaneous horn on the lower lipDermatology Online Journal 2011 17(12):10 [Google Scholar]
[16]. Chakraborty AN, A case of cutaneous hornBr J Dermatol 1951 63:323 [Google Scholar]
[17]. Rekha A, Ravi A, Cornu cutaneum-cutaneous horn on the penisIndian J Surg 2004 66:296-97. [Google Scholar]
[18]. Tauro LF, Martis JJF, John SK, Kumar KP, Cornu cutaneum at an unusual siteIndian J Plast Surg 2006 39:76-78. [Google Scholar]
[19]. Chowdhury J, Kumar P, Gharami RC, Multiple cutaneous horns due to discoid lupus erythematosusIndian J Dermatol Venereol Leprol 2014 80:461-62. [Google Scholar]
[20]. Schosser R, Hodge S, Gaba C, Owen L, Cutaneous horns: a histopathologic studySouth Med J 1979 72:1129-31. [Google Scholar]