Cervical cancer is one of the major causes of death from cancer among women in developing countries. The treatment and operability depends on the degree of cancer extention outside of the cervix [1,2]. Many of these patients present at an advanced stage, especially in the developing world due to the lack of universal screening. Invasion of the urinary bladder is seen in about 6%-8% [3,4] of all patients with cervical cancer and when present, it signifies advanced disease and renders them unsuitable candidates for a curative resection. Therefore, it is of utmost importance to accurately stage the patients and diagnose bladder invasion with complete accuracy. Diagnostic modalities commonly utilized for this include, Computed Tomography (CT) scan, Magnetic Resonance Imaging (MRI) and cystoscopy. CT and MRI, if available are particularly helpful to assess bladder involvement non invasively. However, the availability of these modalities is limited in the developing countries and a significant proportion of patients are unable to afford them due to a lack of health insurance. TVS appears to be a promising alternative in diagnosing bladder involvement, especially in this situation. Its validity has been shown in various studies recently [5–8].
The present study was designed to evaluate the efficacy of TVS and cystoscopy in diagnosing bladder involvement in early stage cervical cancer patients by confirming it intra operatively and further by histopathologic examination.
Materials and Methods
A single center, partially blinded prospective study was conducted at a tertiary care hospital in New Delhi, between March 2006 and September 2009. The study was conducted according to the principles of the Declaration of Helsinki and was approved by the institutional ethical committee. Study subjects consisted of all patients with a diagnosis of early stage (Stage Ia, Ib and IIa) cervical cancer. The study consisted of an initial evaluation and staging phase followed by the treatment phase. In summary, all the patients with a biopsy proven diagnosis of cervical cancer seen at the outpatient gynaecological cancer clinic of our hospital were evaluated with a baseline clinical evaluation, basic laboratory investigations, cystoscopy, Intravenous Pyelography (IVP) and a chest X-ray. In addition, TVS was performed on each patient by a radiologist blinded to the cystoscopy findings to detect invasion of the urinary bladder. No study subject underwent CT or MRI imaging due to lack of universal availability and patient affordability. After the initial evaluation and staging, therapy was planned for each patient by the attending gynaecologist. This consisted of radical hysterectomy with or without pre operative chemotherapy followed by an adjuvant chemotherapy and/or radiation depending upon the histopathologic findings of the resected specimens. A single operating surgeon performed all the radical hysterectomies. Chemotherapy consisted of cisplatin based regimen and was prescribed by the consulting medical oncologists.
During the TVS procedure, the endocervical probe was placed in the anterior fornix with focus on the cervico-vesical junction and images were obtained in multiple planes to identify structural changes suggestive of bladder invasion viz., reduced mobility of the bladder wall, irregular thickening and heteroechoic appearance of the bladder wall, tenting of the bladder wall and loss of integrity of the bladder-cervix interface. In addition, to characterize the primary growth within the cervix, location and dimensions of tumour were also noted. All sonograms were performed by a single radiologist to eliminate inter observer variation.
Results
Keeping in mind the average number of early stage cervical cancer patients presenting to our institution annually and the sample size chosen in similar studies conducted previously [8,9], a total of 30 study subjects were recruited and followed up during the entire study period (March 2006 to September 2009). The clinico-pathologic features of the study subjects and various therapeutic modalities provided are shown in [Table/Fig-1]. All patients belonged to the stages between Ib1 and IIa cervical cancer and no Stage Ia patient was identified. Mean age of the subjects was 40±4.5years. Various histopathologic types identified were moderately differentiated squamous cell carcinoma (n=21), poorly differentiated squamous cell carcinoma (n=4) and well differentiated adenocarcinoma (n=5). All study subjects were alive at the end of the study period.
Distribution of various characteristics among patients.
| Patient Characteristics | Category/Type | N (%) |
|---|
| Mean age (in years) | 40±4.5 | |
| Mean parity | 4±1.2 | |
| FIGO stage | Ib1 | 12 (40) |
| Ib2 | 8 (26.66) |
| IIa | 10 (33.33) |
| Treatment providedAdjuvant chemoRadiation | Pre operative chemotherapy | 8 (26.6) |
| Hysterectomy | 30 (100) |
| Post operative chemoradiation | 5 (16.6) |
| Post operative radiotherapy | 3 (10) |
| Tumour histology | Moderately differentiated squamous cell carcinoma | 21 (70) |
| Poorly differentiated squamous cell carcinoma | 4 (13.33) |
| Adenocarcinoma | 5 (16.66) |
All study subjects (n=30) underwent radical hysterectomy and subjects with stage Ib2 disease (n=8) received 2-3 cycles of cisplatin based pre operative chemotherapy. TVS was performed before and after the chemotherapy treatment in these eight patients and was found to be normal on both the occasions. Three patients with features suggesting intermediate risk of recurrence (large tumour size, cervical stromal invasion, lympho-vascular space invasion) underwent post operative radiation while five patients with features of high risk of recurrence (parametrial or lymph node involvement and positive margins) received chemo-radiation post operatively.
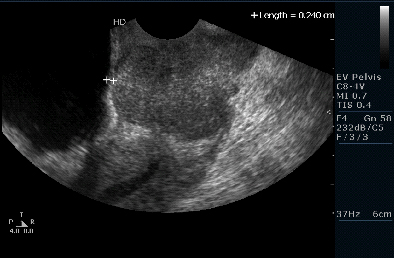
Pre operative cystoscopy showed no evidence of bladder invasion in all 30 patients. On the other hand, TVS was positive for bladder involvement in three of these patients. In these cases, a tumour protuberance was noted at the cervico-corporeal junction, resulting in an elevation of the bladder wall and causing a tent like appearance of the bladder wall on TVS. In addition, the inner bladder wall was found to be heteroechoic with abnormal surface and echotexture. The ability of the bladder to slide over the cervix was also found to be restricted in these cases. Other features indicating bladder involvement included irregular thickening of the bladder wall and an absence of a well-defined plane between bladder and cervix [Table/Fig-2,3].
TVS image of a patient with no bladder involvement showing smooth bladder cervix interface.

TVS image of a patient with bladder involvement showing tenting of the bladder wall.
In these three patients, the bladder wall was found to be stuck to the cervix and was invaded by the tumour intra operatively (superficial detrusor muscle invasion). Sharp dissection had to be performed to release it from cervix. The part of bladder wall, which appeared invaded by the tumour was resected and sent for histopathologic examination which confirmed bladder wall invasion.
The remaining 27 patients had no evidence of bladder involvement intra operatively.
Discussion
Cervical cancer is one of the most common causes of mortality from cancer among women in the developing world [10]. Appropriate pre operative staging of the disease is imperative in order to plan therapy. In addition to cystoscopy, imaging modalities like CT and MRI, although not mandatory for staging, have become standard tools to diagnose lymphatic or parametrial spread and involvement of the adjacent organ especially in the developed countries owing to their easy availability.
Bladder invasion, if present portends a less than 16% five year survival [11–13]. Potentially, bladder invasion may be missed during a cystoscopic examination if the tumour only involves the outer bladder wall without any invasion of the mucosa. In addition, CT and MRI are not universally available in developing countries. Thus, any non invasive modality that detects bladder invasion accurately will be of extreme use in this special setting.
TVS is a promising tool to diagnose bladder invasion owing to its easy availability, and comparatively lower cost. Both the inner and outer wall of the bladder can be clearly distinguished and seen on TVS. Bladder invasion may easily be diagnosed on TVS by identifying disruption, irregularity or tenting of the outer bladder wall. Although TVS has not been widely studied in the pre surgical staging of cervical cancer, we found it to be 100% sensitive in diagnosing bladder invasion. This was confirmed both intra operatively and by histopathologic examination of the excised specimens. Similar results were reported by Iwamoto K et al., [8]. In their study, the diagnosis of bladder invasion was made by restricted mobility of the bladder wall over the cervix upon moving the probe in anterior fornix. They also reported a relatively lower accuracy of CT and MRI in detecting bladder invasion. The study conducted by Deo SV et al., revealed that the accuracy of trans-abdominal pelvic sonography was comparable to that of CT scan in detecting bladder involvement in cervical cancer patients [14]. In a separate study, Huang WC et al., also reported a 100% sensitivity of the TVS in diagnosing bladder infiltration [9]. The variables they measured on TVS to define bladder infiltration included bladder wall thickness, less clear-cut bladder wall outline and morphological changes in the inner bladder.
Limitation
The sample size, in the present study, was relatively small and the findings need to be confirmed by trials with larger sample size.
Conclusion
Our study showed that TVS is more sensitive than cystoscopy in the pre-operative diagnosis of bladder invasion in early stage cervical cancer and could be the preferred modality of choice, especially if imaging modalities like CT and MRI are not widely available. More studies with larger sample size are the needed to confirm our findings.