Knowledge Attitude and Perception of Sex Education among School Going Adolescents in Ambala District, Haryana, India: A Cross-Sectional Study
Randhir Kumar1, Anmol Goyal2, Parmal Singh3, Anu Bhardwaj4, Anshu Mittal5, Sachin Singh Yadav6
1 Assistant Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
2 Assistant Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
3 Assistant Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
4 Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
5 Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
6 Assistant Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Randhir Kumar, Assistant Professor, Department of Community Medicine, MMIMSR, Mullana, Ambala-133207, Haryana, India.
E-mail: randhirchintu@gmail.com
Introduction
Adolescence is a highly dynamic period characterised by rapid growth and development. Adolescents have limited knowledge about sexual and reproduction health, and know little about the natural processes of puberty, sexual health, pregnancy or reproduction. Sex education should be an integral part of the learning process beginning in childhood and continuing into adult life, because it is lifelong process.
Aim
This study was carried out to identify the knowledge and attitude of imparting sex education in school going adolescents in rural and urban area of Ambala district
Materials and Methods
A cross sectional study design was used to study the knowledge of reproductive and sexual health among school going children. A total of 743 adolescents from age group of 13-19 year were studied, using self designed semi-structured questionnaire to assess the knowledge regarding reproductive and sexual health among adolescents
Results
The mean age of study subjects was 15.958±1.61 years, majority of adolescents i.e., 93.5% favour sex education. An 86.3% said sex education can prevent the occurrence of AIDS and 91.5% of adolescents prefer doctors should give them sex education followed by 83.0% school/teacher and least preference was parents 37.3%.
Conclusion
There were substantial lacunae in the knowledge about reproductive and sexual health. Students felt that sex education is necessary and should be introduced in the school curriculum.
Menstruation, Reproductive health, Sexually transmitted diseases
Introduction
The term adolescence comes from Latin word meaning “to grow to maturity” [1]. According to WHO 10-19 years is called adolescents [2]. It is the period when maximum amount of physical, psychological, emotional and behavioural changes take place [3].
Physical health, sexual and behavioural problems of adolescents are interrelated and these factors are related to unhealthy development in adolescents stem from the social environment. It also includes poverty, unemployment, crime, sexual harassment, gender and ethic discrimination and impact of social change on individual, family and communities. So adolescents need to provide preventive interventions for these behaviours are the same and all contribute to positive personal growth and development [4].
Adolescents need to know how to protect themselves from HIV/STDs and premature pregnancies, for this sex education is the best way, it should be a lifelong learning process based on the knowledge and skills and positive attitude, it helps to young people to enjoy sex and relationships that are based on qualities such as positive knowledge, mutual respect, trust, negotiation and enjoyment.
Age appropriate knowledge among youth and adolescents about the changes during puberty, sexuality, modes of transmission and prevention of sexually transmitted infections, HIV, and to maintaining a healthy and safe sexual life is important for the health and welfare and aware them to prevent unwanted pregnancies and of HIV/AIDS [5].
Sex education should be an integral part of the learning process beginning in childhood and continuing into adult life and its lifelong learning process. It should be for all children, young people and adults, including those with physical learning or emotional difficulties. It should encourage exploration of values and morale values, consideration of sexuality and personnel relationships and the development of communication and decision making skills. It should foster self-esteem, self-awareness, a sense of moral responsibility and the skills to avoid and resist sexual experience [6].
Health education plays important roles in human life and it is also a fundamental right. It can help to increase self-esteem, develop effective communication skills and encourage awareness about health and disease related knowledge. The mixture of myths/stigma secrecy, lack of knowledge, social disparity and negative media messages confuses young people and encourages poor self-esteem resulting in uninformed choices being made and it may lead to incorrect knowledge about sex, unprotected sex, unplanned pregnancy; STI’S including HIV/AIDS or deeply unhappy and damaging relationship [7].
Because of lack of clear protocol for sex education, like content, way of approaches, rules and regulation etc., for educational services and how these services should be fulfilled in different socioeconomic and cultural environments is not clear [8]. So, this study was done to identify the knowledge attitude and perception of sex education among school going adolescents.
Materials and Methods
A school based cross-sectional study was conducted among school going adolescents in a rural and urban area of district Ambala, Haryana for a period of six months from January 2015 to July 2015. Adolescent in the age group 13-19 years studying in class 9th to 12th were included and those who had not given consent and who had not completed questionnaires were excluded from study. The sample size was calculated on the basis of prevalence of knowledge regarding reproductive and sexual health with confidence limit 95% and margin of sampling error 10% by using the formula n=4pq/l2, to work out the required sample size the following equation was applied n=4pq/l2. Literature review reveals that the prevalence of knowledge regarding reproductive and sexual health among school going adolescents in India is 35% (WHO/MOHFW [9] and Mittal k et al., [10]). As the data on knowledge regarding reproductive and sexual health for Haryana state is not available, so the sample size was calculated by presuming the prevalence of knowledge regarding reproductive and sexual health in school going children in India to be 35% and thus the sample size for the study came out 743. These samples were divided into 4 strata rural/urban, government/private, class wise and sex wise were taken through stratified random sampling technique and then use simple random sampling technique to reach the total sample size. Ambala district has 224 higher and senior secondary schools only co-educational schools were taken for study. There were 134 government and 69 private co-educational schools in the six community development blocks of district Ambala. As the number government and private schools were in 2:1 ratio, so eight government and four private schools were selected randomly [11], and the number of students included in the study was 446 and 297 from government and private schools respectively. The number of schools in the government sector was more in rural areas and greater numbers of private schools were located in urban areas so the Probability Proportionate To Size (PPS) technique was used to cover the sample size of 743 student. One section of each class from selected school was included in the study, which was taken at random. Only those students were enrolled in the study those fulfilled the inclusion criteria, interview was continued till total sample were covered. Special care was taken to include the students in age group from 13-19 years by ensuring participation of all classes from 9th to 12th. A self designed, semi-structured, self-report pretested questionnaire was used to screen students regarding knowledge and attitude about sex education. The questionnaires were divided in to two groups. Part-1: Socio demographic profile and part-2: sexual health and knowledge, attitude and source of giving sex education. Most of the questions were structured with 3-5 options. Students were to answer one option unless specified otherwise. Open-ended question were given wherever description of answers was required. The questions were framed in English and translated into Hindi. Both Hindi and English questionnaires were used as per choice of the respondents. The study was conducted after obtaining written permission from district education officer, Ambala. Permission was also obtained from the principals of the selected schools. Informed and written consent was also obtained from parents during teacher- parents meeting. Completed questionnaires were compiled and entered into Microsoft Excel and analysed using Stastical Package of Social Sciences (SPSS) version 21, chi-square test and bar diagram.
Results
The present study was a cross-sectional study conducted in rural and urban areas of district Ambala, Haryana. A total of 743 school- going adolescents studying in classes 9th to 12th in the selected government and private schools situated in different parts of urban and rural areas were included in the study. A total of 743 students of 13-19 years age-group those responded well, without hiding any problem were the subjects of the present study. [Table/Fig-1] shows that 294(39.5%) of adolescents belonged to 15-16 year age group. The mean age of studied subjects was 15.958±1.61. Female were 358 (48.2%) and 385 (51.8%) were male. There were more students from government schools 446 (60%). More number of students were studying in class 10th and 11th i.e., 27.2% each, and in urban area 204 (53.5%) belongs to nuclear family and in rural area 198 (54.7%) belongs to joint family. Maximum 211 (28.4%) of adolescents belongs to SES class III and lowest number from class I 84 (11.3%). Whereas in rural area majority of adolescents belongs to SES class V and in urban area majority of adolescents belongs to class II. It was statistically highly significant (p<0.001).
Socio demographic profile of respondents.
| Variables | Ruraln (%) | Urbann (%) | Totaln (%) | χ2 (p-value) |
|---|
| Age group (years) |
| 13-14 | 52 (14.4%) | 106 (27.8%) | 158 (21.3) | 23.9(p<0.001) |
| 15-16 | 161 (44.4%) | 133 (34.9%) | 294 (39.5) |
| 17-18 | 136 (37.6%) | 121 (31.7%) | 257(34.6) |
| >19 | 13 (3.6%) | 21 (5.5%) | 34 (4.6%) |
| Mean age | 16.11±1.357 | 15.82±1.809 | 15.958±1.61 |
| Sex |
| Boys | 190 (49.4%) | 195 (50.6%) | 385 (51.8%) | 0.127(p=0.722) |
| Girls | 172 (48.0%) | 186 (52.0%) | 358 (48.2%) |
| Type of school |
| Government | 287 (64.3%) | 159 (35.7%) | 446 (60.0%) | 109(p<0.001) |
| Private | 75 (25.3%) | 222 (74.7%) | 297 (40.0%) |
| Class |
| 9 | 60 (16.6%) | 83 (21.8%) | 143 (19.2%) | 7.22(p=0.065) |
| 10 | 94 (26.0%) | 108 (28.3%) | 202 (27.2%) |
| 11 | 113 (31.2%) | 89 (23.4%) | 202 (27.2%) |
| 12 | 95 (26.2%) | 101 (26.5%) | 196 (26.4%) |
| Type of family |
| Joint | 198 (54.7%) | 177 (46.5%) | 375 (50.5%) | 5.041(p=0.025) |
| Nuclear | 164 (45.3%) | 204 (53.5%) | 368 (49.5%) |
| Socio-economic status (SES) |
| I | 4 (1.1%) | 80 (21.0%) | 84 (11.3%) | 290.55(p<0.001) |
| II | 33 (9.1%) | 123 (32.3%) | 156 (21.0%) |
| III | 100 (27.6%) | 111 (29.1%) | 211 (28.4%) |
| IV | 44 (12.2%) | 62 (16.3%) | 106 (14.3%) |
| V | 181 (50.0%) | 5 (1,3%) | 186 (25.0%) |
Present study [Table/Fig-2] reveals the association between different socio-demographic profile and perception of need of sex education among adolescents; it shows that majority of adolescents 695 (93.5%) favour sex education. However, boys 374 (97.1%) were more likely to favour sex education as compared to girls 321 (89.7%). It was found that adolescents with higher age group, belongs to urban area and private school with higher SES favours sex education in school. It was considered statistically significant.
Perception of sex education according to their socio-demographic profile of adolescents.
| Variables | Yes | No | Total | χ2 (p-value) |
|---|
| Age group (years) |
| 13-14 | 138 (87.3%) | 20 (12.7 %) | 158 (100%) | 18.206 (p≤0.001) |
| 15-16 | 273 (92.9%) | 21 (7.1 %) | 294 (100%) |
| 17-18 | 251 (97.7 %) | 6 (2.3%) | 257 (100%) |
| >19 | 33 (97.1%) | 1 (2.9%) | 34 (100%) |
| Sex |
| Boys | 374 (97.1%) | 11 (2.9%) | 385 (100%) | 18.1(p≤0.001) |
| Girls | 321 (89.7%) | 37 (10.3%) | 358 (100%) |
| Type of school |
| Government | 406 (91.0%) | 40 (9.0%) | 446 (100%) | 11.617(p=0.001) |
| Private | 289 (97.3%) | 8 (2.7%) | 297 (100%) |
| Place of school |
| Rural | 332 (91.7%) | 30 (8.3 %) | 362 (100%) | 3.899 (p=0.048) |
| Urban | 363 (95.3%) | 18 (4.7%) | 381(100%) |
| Class |
| 9 | 121 (84.6%) | 22 (15.4%) | 143 (100%) | 33.899(p<0.001) |
| 10 | 184 (91.1%) | 18 (8.9%) | 202 (100%) |
| 11 | 198 (98.0%) | 4 (2.0 %) | 202 (100%) |
| 12 | 192 (97.9%) | 4(2.1%) | 196 (100%) |
| Type of family |
| Joint | 344 (91.7%) | 31 (8.3%) | 375 (100%) | 4.088(p=0.043) |
| Nuclear | 351 (95.4%) | 17 (4.6 %) | 368 (100%) |
| Socio-economic status |
| I | 83 (98.8%) | 1 (1.2%) | 84 (100%) | 30.022 (p<0.001) |
| II | 153 (98.0%) | 3 (2.0 %) | 156 (100%) |
| III | 198 (93.8%) | 13 (6.2%) | 211 (100%) |
| IV | 96 (90.6%) | 10 (9.4%) | 106 (100%) |
| V | 165 (88.7%) | 21 (11.3%) | 186 (100%) |
[Table/Fig-3] reveals the reason for sex education among adolescents, out of 695 adolescents who are in favour of sex education, 600 (86.3%) said sex education can prevent the occurrence of AIDS, whereas 396 (57.0%) removes myth, 373 (53.7%) believe knowledge of sex makes future life easy, 275 (39.5%) thought that protects from other diseases and 102 (13.7%) don’t give any reason for sex education.
Perception of the reasons of sex education among adolescents (n=695).
| Reason for sex education | Boys | Girls | Total* |
|---|
| Prevent the occurrence of AIDS | 344(49.5%) | 256(36.8%) | 600(86.3%) |
| Protect from other disease | 158(22.7%) | 117(16.8%) | 275(39.5%) |
| Knowledge of sex makes future life easy | 209(30.1%) | 164(23.6%) | 373(53.7%) |
| Remove myth | 236(34.0%) | 160(23.0%) | 396(57.0%) |
| Need of their age | 156(22.4%) | 119(17.1%) | 275(39.5%) |
| Not stated | 20(2.7%) | 82(11.0%) | 102(13.7%) |
(*Multiple responses)
[Table/Fig-4] reveals that majority of adolescents thought 615 (86.9%) sex education and STDs, 581 (82.2%) menstruation and its hygiene, 512 (72.3%) changes occurring during puberty and 503 (71.0%) drug abuse was the most common topic that should be discussed in class. However, 349 (49.4%) urban adolescents thought menstrual and its hygiene topic and about 280 (39.5%) rural adolescents sex education and STDs related topic should discuss in class.
Perception of students about content of sex education.
| Topic should discuss in class | No. of responses |
|---|
| Rural | Urban | Total * |
|---|
| Changes occurring during puberty | 178(25.1%) | 334(47.2%) | 512(72.3%) |
| Menstruation and its hygiene | 232(32.8%) | 349(49.4%) | 581(82.2%) |
| Birth spacing and contraception | 217(30.7%) | 249(35.2%) | 466(65.9%) |
| Maternal and child health | 261(37.0%) | 201(28.5%) | 462(65.4%) |
| Sex education and STDs | 280(39.5%) | 335(47.3%) | 615(86.9%) |
| Drug abuse | 259(36.6%) | 244(34.5%) | 503(71.0%) |
(*Multiple responses)
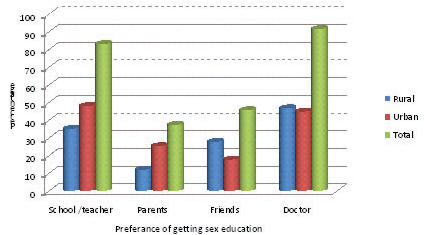
[Table/Fig-5] shows the area wise distribution of respondents according to their preference for getting sex education. It was found that majority 680 (91.5%) of adolescents prefers doctors should give them sex education followed by 617 (83.0%) school/teacher and least preference was parents 277 (37.3%). However, in urban adolescents most common preference for sex education was school/teacher i.e., 357(48.0%) and in rural area 347 (46.7%) doctor was the most common preference for getting sex education.
Distribution of respondents according to their preference for getting sex education.
Discussion
This study has tried to assess the knowledge, attitude and practices regarding reproductive health and sexual problems, to assess the perception regarding reproductive and sexual health among adolescents and to identify the need of imparting sex education in school going adolescents (13-19 year) from urban and rural area of district Ambala Haryana.
Regarding the need of sex education among adolescents, it shows that majority of adolescents (93.5%) favour the sex education. However, boys (97.1%) were more likely to favour sex education as compared to girls (89.7%). A similar study was conducted by Jaideep K et al., in Chandigarh found that 95% of students were in favours of mainstreaming of sex education [12]. Another study done by Benzaken T et al., shows 90% favours sex education and study by Thakur HG et al., shows that 90% and 97% favours sex education, among boys 82.9% and among girls 75.6% respectively [13,14]. A study done by Dorle AS et al., from Karnataka found only 48% of student favours sex education in higher and senior secondary school and it was lower than our study it might be because of regional and cultural difference and also study was conducted five year back [15].
To find out the reason of sex education, 86.3% participants said that sex education can prevent the occurrence of AIDS, whereas 57.0% remove myth, 53.7% knowledge of sex makes future life easy, 39.5% protect from other disease and 102 (13.7%) don’t give any reason for sex education. A study done by Mueller TE et al., reported that majority of adolescents said sex education reduce the risks of potentially negative outcome from sexual behaviour such as fear and stigma of menstruation, unwanted and unplanned pregnancies and infection with STIs including HIV [16]. To know the preference for getting sex education, present study found that majority 680 (91.5%) of adolescents prefers doctors followed by 617 (83.0%) school/teacher and least preference was parents 277 (37.3%) respectively. A similar study was conducted by Jaideep K et al., in Chandigarh found that 76.74% students choose the teacher as the best source to provide sex education [12]. Similar observation was found by Wong WC et al., in Hongkong and Zhang L et al., in China [17,18]. All these variation might be because of regional and cultural difference. A study done by Dorle AS et al., from Karnataka found girls favours parents and boys favours friend as a source of information about sex [15]. A view point given by Datta SS et al., favours school and college should give sex education to adolescents [19].
Limitation
This study suffers from the usual limitation of a cross-sectional study. We only include the co-education school so it cannot be generalizes to all school adolescent. As sex education is a sensitive topic, we cannot guarantee about the honest answers as it covered the sensitive issue i.e., recall bias. Participants may agree with statements as presented to them, especially when in doubt i.e., acquiescence bias and also social desirability bias.
Recommendation
Sex Education must be introduced in the school which should start from the primary school and brings about the age appropriate topics as they go through the high school. It should contain a package of information about life skills, reproductive health, safe sex, pregnancy and STI’s including HIV/AIDS. A socio cultural research is needed to find the right kind of sexual health education services for boys and girls separately from the teacher of same gender. It is the responsibility of parents, teachers, social workers, politicians, administrators, medical and paramedical profession so that adolescent girl or boy got legitimate due to education and empowerment and change over to adult men or women is smooth and streamlined with nil or least medical, social or psychological problems.
Conclusion
In this present study knowledge and perception of sex education was good, majority believe that sex education should implemented in school curriculum and majority of them gave good reason for sex education implementation in school. The most common preference for getting sex education was from doctor and teacher/school followed by friend respectively. Sex education and sexuality is unaccepted in many communities and also among some parents, adolescents feel shy and scared to talk about sex education, some adolescents hesitate to reply about sex education especially girls.
(*Multiple responses)
(*Multiple responses)
[1]. Bansal RD, Mehra M, Adolescent girls an emerging priorityIndian J Public Health 1998 42(1):1-2. [Google Scholar]
[2]. WHO. Adolescents, The critical phase, the challenges and the potential published by WHO [Internet]. Regional office for South-East Asia, New Delhi 1997. [Cited 2014 April 25] Available from: URL:http://www.searo.who.int/entity/child_adolescent/documents/adolescent_critical_phase/en [Google Scholar]
[3]. Leland NL, Petersen DJ, Braddock M, Alexander GR, Variations in pregnancy outcomes by race among 10-14-year-old mothers in the United StatesPublic Health Rep 1995 110(1):53-58. [Google Scholar]
[4]. Menon S. Adolescent health issues, public Health update 2002; pp. 1.3 [Google Scholar]
[5]. Parimala S. Sex education in Indian schools [Internet]. WHO World health forum 1995;16(3):277-78. [Cited 2014 April 10] Available from: URL: http://www.who.int/iris/handle/10665/47114 [Google Scholar]
[6]. Info series No. 6, Sex education for Adolescents. Indra Gandhi institute of child health, Bangalore 2006:3-4 [Google Scholar]
[7]. Grunseit, Kippex. Effects of sex education on young people’s sexual behaviour [Internet]. WHO/GPA, Geneva.1993:18-20. [Cited 2014 March 02] Available from: URL: http://data.unaids.org/publications/IRC-pub01/jc010impactyoungpeople_en.pdf [Google Scholar]
[8]. Friedman HL, Edstrum KG, Adolescent reproductive health. An approach to planning health service research, IntroductionWHO Offset Publ 1983 (77):1-53. [Google Scholar]
[9]. WHO/ MOHFW. Reproductive and Sexual Health of Young People in India. Secondary analysis of data from National Family Health Surveys of India - 1, 2, 3 (1992-2006) for the age group 15-24 years. New Delhi: GOI, MOHFW; 2009. [Cited 2012 August 25] Available from: URL: http://mohfw.nic.in /NRHM/Documents/RSH_of_YP_in_India.pdf [Google Scholar]
[10]. Mittal K, Goel MK, Knowledge Regarding Reproductive Health among Urban Adolescent Girls of HaryanaIndian J Community Med 2010 35(4):529-30. [Google Scholar]
[11]. Qadri SS, Goel R, Singh J, Ahluwalia SK, Pathak R, Bashir H, Prevalence and pattern of substance abuse among school children in northern India: A rapid assessment studyInt J Med Sci Public Health 2013 2(2):273-82. [Google Scholar]
[12]. Jaideep K, Need Assessment for Sex Education amongst the University Students –A Pilot StudyGJMEDPH 2012 1(2):23-29. [Google Scholar]
[13]. Benzaken T, Palep AH, Gill PS, Exposure to and opinions towards sex education among adolescent students in Mumbai: A cross-sectional surveyBMC Public Health 2011 11:805 [Google Scholar]
[14]. Thakor HG, Need Assessment for sex education amongst the school childrenIndian J Community Med 1998 23(2):62-68. [Google Scholar]
[15]. Dorle AS, Hiramath LD, Mannapur BS, Ghattargi CH, Puberty changes in secondary school children of Bagalkot, KarnatakaJournal of Clinical and Diagnostic Research 2010 (4):3016-19. [Google Scholar]
[16]. Mueller TE, Gavin LE, Kulkarni A, The association between sex education and youth’s engagement in sexual intercourse, age at first intercourse, and birth control use at first sexJ Adolescents Health 2008 42:89-96. [Google Scholar]
[17]. Wong WC, Lee A, Tsang KK, Lynn H, The impact of AIDS/Sex education by schools or family doctors on Hong-Kong Chinese adolescentsPsychol Health Med 2006 11(1):108-16. [Google Scholar]
[18]. Zhang L, Xiaoming Li, Shah IH, Where do Chinese adolescents obtain knowledge of sex? Implications for sex education in ChinaHealth Education 2007 107(4):351-63. [Google Scholar]
[19]. Datta SS, Majumder N, Sex education in schoolJournal of Clinical and Diagnostic Research 2012 6(7):1362-64. [Google Scholar]