Ulcerative colitis is a chronic idiopathic inflammatory disease of the gastrointestinal tract that affects the large bowel and is a major disorder under the broad group of conditions termed Inflammatory Bowel Diseases (IBDs). The disease is characterized by a chronic course with intermittent flares interposed between variable periods of remission [1]. Correct assessment of disease activity and potential exacerbating factors are crucial in deciding the choice of treatment [2,3]. The study aimed to find out various risk factors involved in the exacerbation of ulcerative colitis especially the role of CMV infection and also to evaluate various clinical, endoscopic and histological parameters in assessing disease activity.
Materials and Methods
It was a prospective study of ulcerative colitis patients presenting with acute exacerbation of symptoms (cases) and those who were in remission (controls) attending Department of Gastroenterology, Government Medical College, Kozhikode, Kerala, India, during January 2011 to May 2013 period.
Patients with a diagnosis of ulcerative colitis based on clinical features, endoscopic findings and histopathology followed-up in Department of Gastroenterology who were in remission for at least three months, presenting with an acute exacerbation of symptoms were included in the case group. Control group included similar ulcerative colitis patients in remission with at least three months duration.
Patients not willing for the study and those who had any contraindication for colonoscopy/biopsy were excluded from the study.
A detailed evaluation of the disease history including personal history, treatment compliance and clinical disease severity were noted. Dietary habits, personal stress and smoking history were also recorded. Investigations including blood routine, endoscopic examination with biopsy, histopathological examination and immunohistochemistry for CMV on the biopsy sample were done.
Stress of the patient was assessed using Perceived Stress Scale (PSS) which consisted of a questionnaire about their feelings and thoughts during the last month [4,5].
The clinical disease severity was graded according to True love and Witt’s criteria and Ulcerative Colitis Disease Activity Index [6,7].
True Love and Witt’s Criteria [
6]
This purely clinical classification categorizes disease as mild, moderate, or severe based on a combination of clinical findings and laboratory parameters such as stool frequency, presence of fever, tachycardia, anaemia and ESR levels.
Ulcerative Colitis Disease Activity Index (UCDAI) [
7]
A numerical disease activity instrument that is more useful for patients with limited disease. This index combines clinical and endoscopic assessments such as stool frequency, amount of bleeding per rectum, endoscopic findings and physician’s global assessment of the patient.
The disease activity index ranges from 0 to 12, with the higher total scores representing more-severe disease. In general, a patient is considered to be in remission if the score is two or less and to have severe disease if the score is greater than ten. An index that has been used extensively in randomized controlled trials is the Mayo score, which incorporates the same four components as the UCDAI [8].
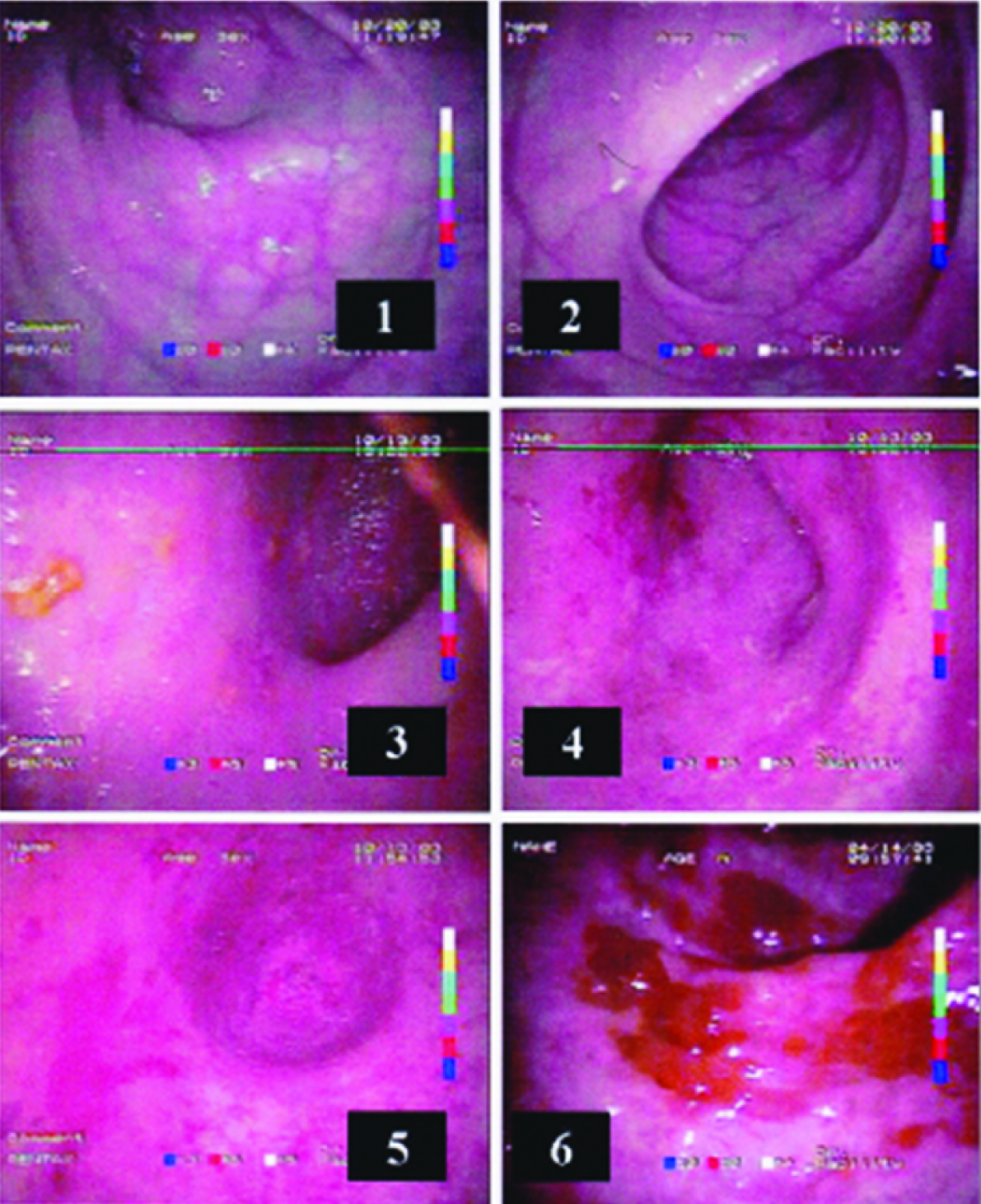
The endoscopic findings were graded from 0 to 4 according to Jewel’s endoscopic criteria [9]. Grade 0 denotes normal mucosa and Grade 4 denotes mucosa with spontaneous bleeding and ulceration. For this study endoscopic grade of 3 or 4 is considered as severe disease [Table/Fig-1].
Endoscopic appearances; 1&2: normal mucosa, 3: Grade 1, 4: Grade 2, 5: Grade 3, 6: Grade 4
Samples of colonic biopsy were fixed in 10% formalin and routinely processed in automatic tissue processor (Leica Biosystems) and their paraffin embedded blocks were prepared. Thin sections were cut from the tissue blocks. One section was stained with Haematoxylin and Eosin (H&E) and on other section performed immunohistochemistry for CMV (Cytomegalovirus Antibodies 2/6 CMVPP65-A).
Immunohistochemistry was performed using Peroxidase-Anti-Peroxidase (PAP) method [10]. A 4 μm thick sections from the paraffin embedded tissue blocks were taken on adhesive-coated slides and manual immunohistochemistry was performed. Slides were incubated with primary antibody for CMV (Novocastra™, Leica Biosystems). The staining was visualized using 3, 3’-Diaminobenzidine-substrate-chromogen (DAB) solution and counterstained using Ehrlich’s haematoxylin.
H&E stained sections were examined and graded according to Geboes histological score [11]. The histological parameters that were considered include degree of architectural change, amount of chronic inflammatory infiltrate, amount of neutrophils and eosinophils in lamina propria, percentage of crypts with neutrophils, amount of crypt destruction and presence of erosion/ulceration. Each parameter was subgraded from 0 to 3. A subgrade of 0 or 1 was considered as mild for that parameter and a subgrade of 3 was considered as severe for that parameter.
A single histological score (acute score) to determine the histological activity was derived by adding the subgrades of neutrophils in lamina propria, neutrophils in epithelium, crypt destruction and erosion or ulceration in each patient. Cytopathic changes of CMV infection were examined both in H&E stained slide and immunohistochemical stained slide. The study was initialized after getting approval from the Institutional Ethics Committee.
Statistical Analysis
Data was entered according to the variables onto spreadsheets of Microsoft Office Excel 97 - 03 and the variables were analyzed using standard analytical techniques with SPSS version 16.0 for Windows. Quantitative variables were expressed as mean±standard deviation while the qualitative variables were expressed as percentage. The associations between study variables were analyzed using Chi-square test and p-values <0.05 were considered significant.
Results
A total of 58 patients with ulcerative colitis were studied. The sample was constituted by 37 cases and 21 control patients. The age of the patients ranged from 13-71 years. There were 36 males and 22 females [Table/Fig-2].
Age and sex distribution of the sample
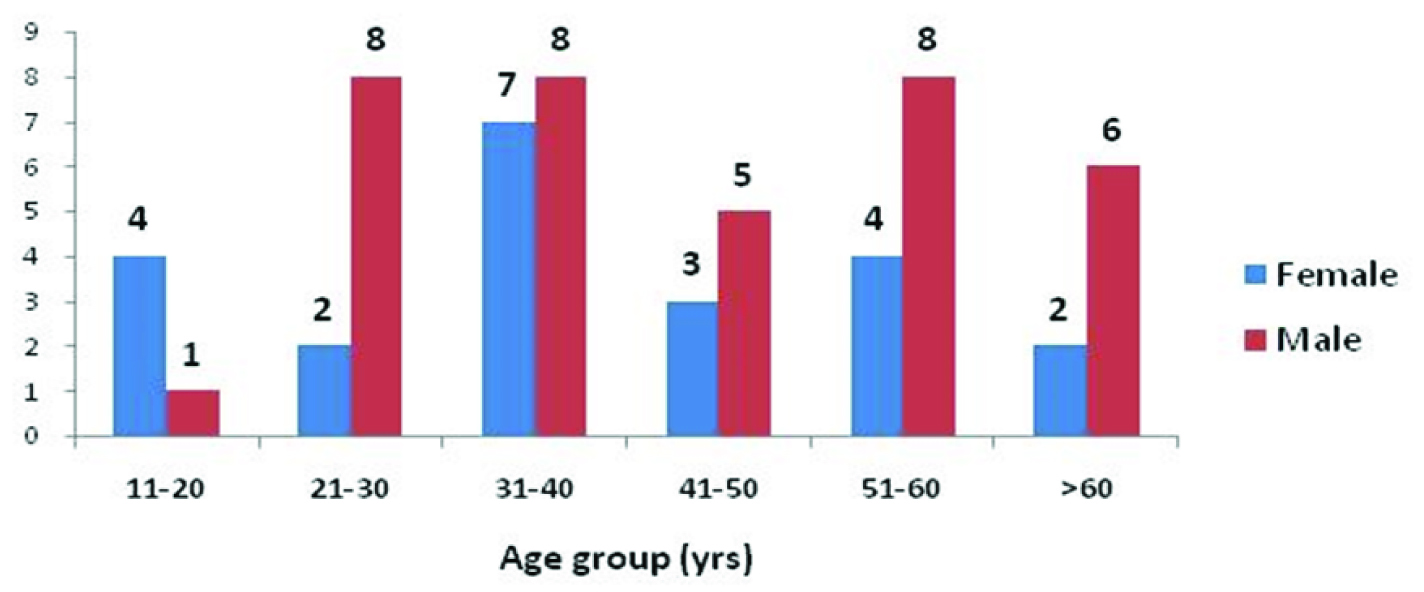
Males constituted 67.6% of cases and 52.4% of control. Age at diagnosis of ulcerative colitis ranged from 12-67 years among cases and 15-65 years among control group. Duration of illness ranged from 0.5-20 years among cases and 1-12 years among control group. Extent of the disease ranged from proctitis to pancolitis in both case and control group with 10 cases and three controls having pancolitis. Percentage of patients with more than one exacerbation was calculated. Eight cases and three controls had more than one exacerbation after their initial diagnosis of ulcerative colitis. Regarding the dietary habit, 35 cases and 18 controls were non-vegetarians. A total of 31 cases and 18 controls were non-smokers at the time of study. Control group showed good treatment compliance than the case group. Mean PSS score was higher among cases than among controls [Table/Fig-3].
Clinical and demographic characteristics of cases and controls.
| Parameter | Case | Control | p |
|---|
| Mean age (years) | 43.6 | 40.0 | 0.3894 |
| Males (%) | 67.6 | 52.4 | 0.2519 |
| Age at diagnosis (mean) | 38.9 | 36.1 | 0.4848 |
| Duration of illness (years) | 4.7 | 3.8 | 0.4528 |
| Presence of pancolitis (%) | 27.0 | 14.3 | 0.2634 |
| >1 exacerbation after diagnosis (%) | 21.6 | 14.3 | 0.4934 |
| Non-vegetarian diet (%) | 94.6 | 85.7 | 0.2468 |
| Smoking at present (%) | 16.2 | 14.3 | 0.8452 |
| Good treatment compliance (%) | 59.5 | 100 | 0.0003 |
| Perceived stress scale score (mean) | 19.6 | 15.0 | 0.0001 |
chi square-test is used
Mean haemoglobin was higher among controls than among cases. Mean TLC and mean ESR were higher for cases than for controls [Table/Fig-4].
Laboratory test results in cases and controls.
| Parameter | Case | Control | p |
|---|
| Haemoglobin (mean g/dl) | 11.4 | 13.6 | 0.001 |
| TLC (mean cells /mm3) | 9991 | 7423 | 0.0067 |
| ESR (mean mm/1st hour) | 48.5 | 17.9 | 0.001 |
chi square-test is used
All 37 cases were having severe disease and all 21 controls were having mild disease according to True love and Witt’s criteria [Table/Fig-5].
Clinical and endoscopy severity scores in cases and controls
| Parameter | Case | Control | p |
|---|
| Truelove score – Severe disease (%) | 100 | 0 | - |
| Mayo score in remission (%) | 0 | 90.5 | 0.001 |
| Mayo score – severe disease (%) | 16.2 | 0 | 0.0513 |
| Jewell endoscopic disease severity grade (severe disease %) [Grade 3, 4] | 97.3 | 4.8 | 0.001 |
chi square-test is used
Severe structural abnormality was seen in nine cases and three controls, severe chronic inflammatory infiltrate in 17 cases and one control, severe increase in lamina propria eosinophils in seven cases and one control, severe increase in lamina propria neutrophils in six cases and two controls, severe increase of neutrophils in epithelium in 18 cases and three controls, severe crypt destruction in 12 cases and no controls and severe erosion in 9 cases and no controls [Table/Fig-6]. The severity assessed by various clinical and endoscopic scores showed significant correlation with the histopathological score [Table/Fig-7].
Histological features in cases and controls (Geboes scoring system).
| Parameter | Case | Control | p |
|---|
| Mild (%)[subgrade 0 & 1] | Severe (%)[subgrade 3] | Mild (%)[subgrade0 & 1] | Severe (%)[subgrade 3] |
|---|
| Structure | 16.7 | 25.0 | 33.3 | 14.3 | 0.2979 |
| Chronic inflammatory infiltrate | 2.8 | 47.2 | 23.8 | 4.8 | 0.0008 |
| Lamina propria eosinophils | 36.1 | 19.4 | 80.9 | 4.8 | 0.002 |
| Lamina propria neutrophils | 8.3 | 16.7 | 76.1 | 9.5 | 0.001 |
| Neutrophils in epithelium | 8.3 | 50.0 | 76.2 | 14.3 | 0.001 |
| Crypt destruction | 22.3 | 33.3 | 85.7 | 0 | 0.001 |
| Erosion or ulceration | 13.5 | 24.3 | 76.2 | 0 | 0.001 |
chi square-test is used
Correlation between acute score versus various clinical and endoscopic severity scores.
| Correlation parameter | Correlation coefficient | F | p |
|---|
| Acute score and Mayo score | 0.45 | 46.5 | 0.001 |
| Acute score and Truelove score | 0.48 | 52 | 0.001 |
| Acute score and Jewell’s endoscopic score | 0.33 | 27.2 | 0.001 |
chi square-test is used
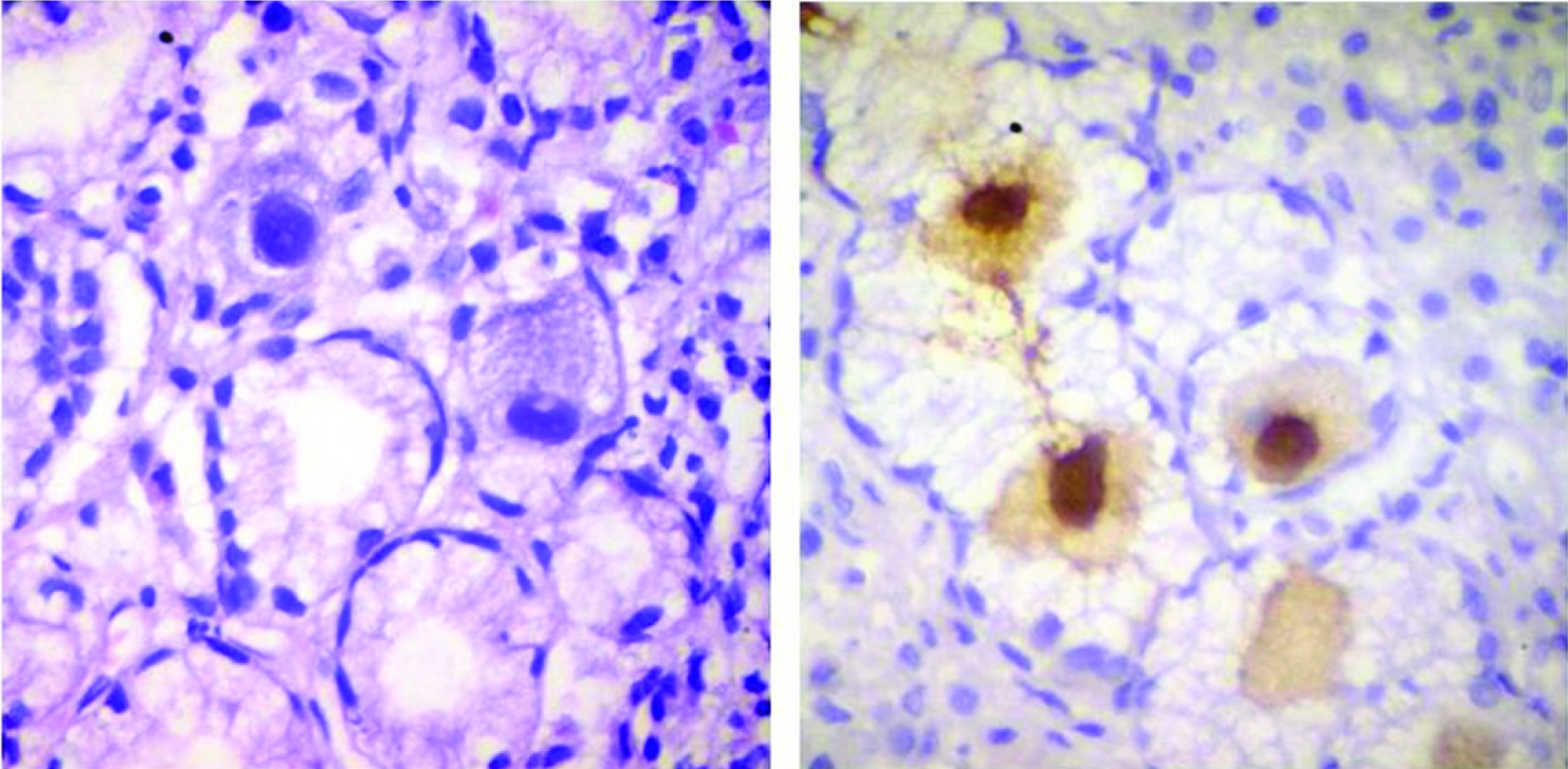
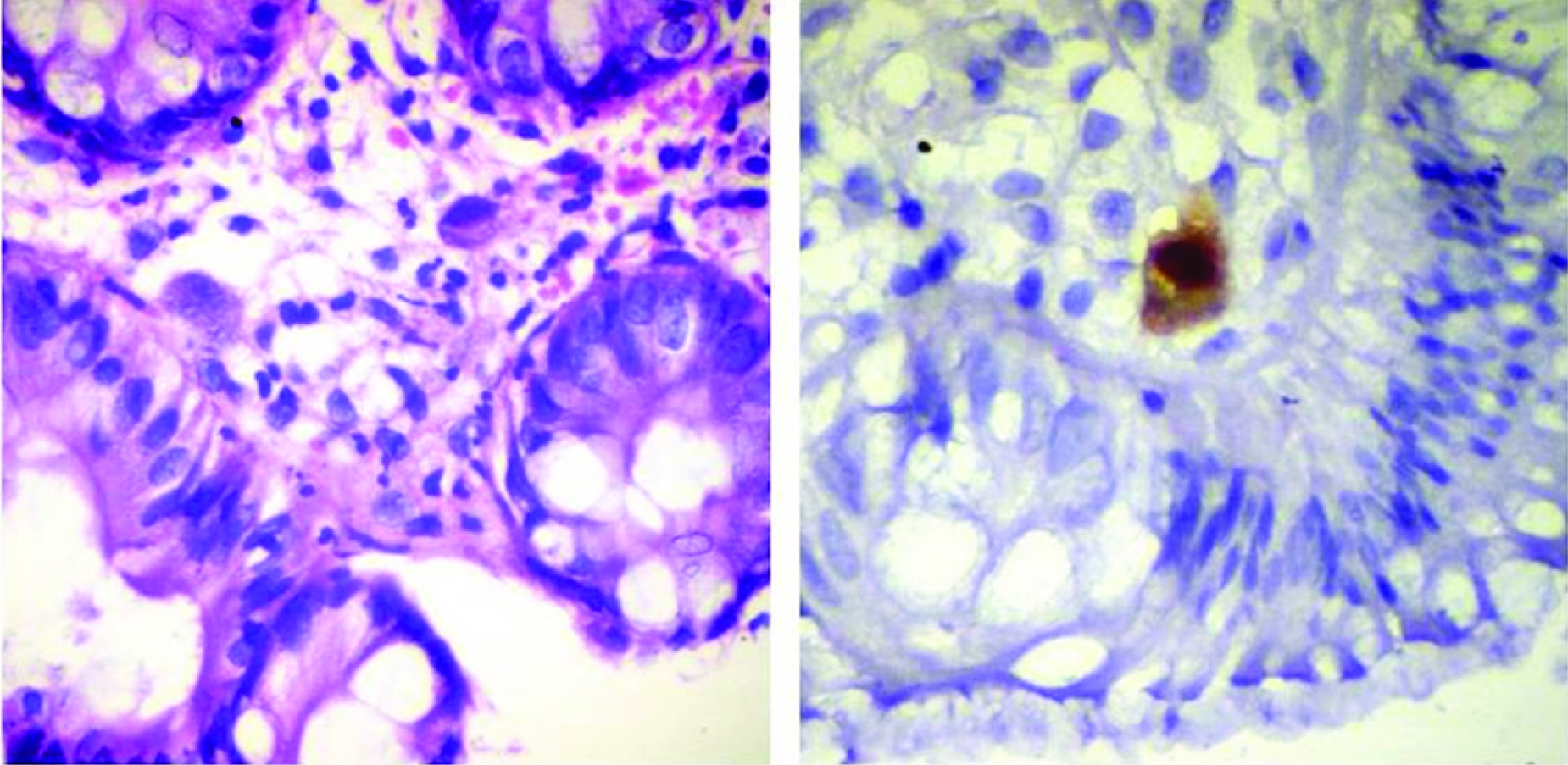
Histopathological examination of two cases (5.4%) showed few large cells, some lining the vessels and some within the lamina propria. These cells had abundant cytoplasm with round nucleus and large prominent intra-nuclear inclusion. Immunohistochemistry (IHC) for CMV was positive in these two cases [Table/Fig-8,9]. IHC for CMV was negative in controls and all other cases.
The photomicrographs of CMV positive case 1. (a:H&E,x400; b:IHC for CMV, x400).
The photomicrographs of CMV positive case 2. (a:H&E,x400; b:IHC for CMV, x400).
Of the two cases in which CMV was detected, the first was a 35-year-old male, diagnosed as having ulcerative colitis at the age of 34 years. He had proctosigmoiditis at the time of diagnosis with bad treatment compliance. He is a non-smoker and takes non-vegetarian diet with PSS score of 18, True love: severe disease, Mayo score: 9, Endoscopy: Grade 4 and histology acute score: 9. The second case was a 54-year-old male, with pancolitis at the time of diagnosis and with good treatment compliance. He is a non-smoker and takes non-vegetarian diet, with PSS score of 14, Truelove: severe, Mayo score: 11, Endoscopy: Grade 4 and histology acute score: 7.
Discussion
At present, the precise aetiology of ulcerative colitis is unknown, but it is thought to be multi-factorial involving genetic, immunologic, and environmental factors. There are several potential risk factors which may precipitate exacerbation in patients with ulcerative colitis in remission. Various risk factors described include enteric infections, use of various drugs including Non-steroidal Anti-Inflammatory Drugs (NSAIDs), stressful events, dietary factors, quitting smoking, change in climate and non-compliance with treatment. Identification of these risk factors are essential for proper management and providing these patients with longer relapse free interval, thereby, improving the quality of life.
Mean age of ulcerative colitis patients at the time of diagnosis was 37 years in our study. Studies done by Gismera CS et al., also had similar findings [12]. Out of the various clinical and demographic parameters; good treatment compliance and PSS score showed a significant difference between cases and controls in our study. Kane S et al., had shown that, medication non-adherence increases the risk of clinical relapse in ulcerative colitis [13]. The study by Levenstein S et al., showed that, long-term perceived stress increases the risk of exacerbation in ulcerative colitis [4].
Basic laboratory parameters like haemoglobin level, TLC and ESR showed a significant difference between cases and controls in our study. Mean haemoglobin level among cases in our study was subnormal. Anaemia may be due to chronic blood loss or due to secondary marrow suppression resulting from chronic inflammation or medication induced. TLC and ESR level among cases were higher than the control group in our study. These findings also indicate active inflammation. Vermeire S et al., mentioned that, markers of inflammation such as ESR and C-Reactive Protein (CRP) give reliable information on disease activity [14]. Some studies have suggested the estimation of fecal lactoferrin and calprotectin levels for the detection of intestinal inflammation in IBD patients. It can be used to differentiate irritable bowel syndrome from IBD and also to determine whether the symptoms in IBD patients are due to disease flare or due to non-inflammatory complications [15–17].
Clinical disease severity indices like True love and Witt’s criteria, Mayo score and Jewell’s endoscopic disease severity grade were significantly different among cases and controls in our study except for Mayo score in severe disease which does not show statistical significance. Assessment of disease activity is important for prognostication and therapeutic decision making. Patient symptoms alone cannot be relied when making treatment decisions because clinical symptoms often either underestimate or overestimate disease activity. So, objective measures such as CRP, fecal calprotectin, or endoscopy should be used to complement assessment of the patient’s clinical symptoms. Composite indices, such as the Mayo clinic index, which combines clinical symptoms with endoscopy can better predict disease activity than individual indices [3].
Geboes histological scoring system also showed significant differences between cases and controls for the various parameters assessed in our study except for the structural changes which was not statistically significant. Endoscopic and histologic findings were complementary. Researchers have found 89% agreement between endoscopy and histopathology for identifying patients in remission. One specific advantage of histology is that the lack of microscopic inflammation on mucosal biopsy effectively excludes active ulcerative colitis, and a biopsy sample can be assessed independently from endoscopy. Incorporation of histology for evaluation has the disadvantage of time delay and more cost [3]. Correlation of various clinical and endoscopic severity scores against histological score showed a positive correlation in our study. Walsh A et al., also had similar results [3]. They also mentioned that, by using a combination of indicators clinicians are more likely to get an accurate picture of the severity of the patient’s disease. Clinicians can then adjust therapy accordingly to achieve the best outcome for the patient. An international agreement as to which index or combinations of indices should be used to evaluate patients should be formed, and this consensus should include definitions of remission, mild disease, moderate disease, and severe disease. More validated studies are required to compare the advantages and disadvantages of various indices and their relationship to the outcome.
The role of CMV in exacerbations of IBD remains a topic of ongoing debate. Various diagnostic tools that are used for CMV detection include serology, anti-genemia, serum Polymerase Chain Reaction (PCR), histology, histology with IHC, tissue PCR, stool PCR, viral culture etc. All these tests have varying sensitivity and specificity [18]. In a study conducted by Domènech E et al., they found that, CMV disease in ulcerative colitis affects only seropositive, steroid-refractory patients and not among healthy controls, inactive ulcerative colitis patients, or steroid-responding ulcerative colitis patients [19]. Kim YS et al., found evidence of CMV infection in three (4.5%) patients with new onset ulcerative colitis [20]. They concluded that, CMV infection is rare in new onset ulcerative colitis. Both these studies suggested that, the use of immunosuppressive medications is an important risk factor for CMV infection in ulcerative colitis. Diepersloot RJ et al., described a case of ulcerative colitis that developed as a result of primary infection with CMV [21]. Kandiel A et al., found a prevalence of CMV infection in acute severe ulcerative colitis of 21–34%, and in the steroid refractory subgroup of these patients 33–36% [22]. Nguyen M et al., suggested that disease severity itself can cause CMV reactivation in patients with little or no steroids/immunosuppressant use [23]. Criscuoli V et al., found evidence of CMV infection in seven (16.6%) patients with acute severe ulcerative colitis, out of which three patients responded to conventional treatment without need for anti-viral therapy [24]. They concluded that, CMV is frequently associated with colitis but is not always pathogenic. Studies on the genotyping of the virus might explain the diversity of its biological behaviour. Carmo AMd et al., suggested that, CMV replication was not accompanied by greater intestinal inflammatory activity and CMV is just a spectator of the inflammatory process in IBD [25]. Dose reduction of corticosteroids and institution of anti viral therapy for U C patients with CMV antigen was found to be effective in long term prognosis study by Inokuchi E et al. He also noted significant avoidance of colectomy in ganciclovir administered patients [26]. Maconi G et al., concluded that, CMV infection is frequently found in surgical specimens of patients with steroid-refractory ulcerative colitis but is frequently unrecognized in pre-operative biopsy specimens, thus, raising concerns about the accuracy of the available diagnostic tools [27].
From the above discussion, it is clear that, CMV infection can initiate ulcerative colitis, can cause acute exacerbation of ulcerative colitis, can be non-pathogenic and can even be undiagnosed in pre-operative biopsy. CMV reactivation in ulcerative colitis patients usually occurs when they are immunosuppressed (steroid dependent) or when they have severe active colitis. Most of the reports of ulcerative colitis associated with CMV are steroid refractory cases. European Crohn’s and Colitis Organisation (ECCO) guidelines and American College of Gastroenterology recommend antiviral treatment when CMV is detected in colonic tissue [28].
Identification of CMV infection in patients with ulcerative colitis is clinically significant even when the prevalence is low because these patients may not respond to the conventional treatment for ulcerative colitis and may require treatment with anti viral drugs to avoid complications. Clinicians should be aware of the possibility of concurrent CMV infection while treating patients with acute exacerbation of ulcerative colitis not responding to the conventional management.
The prevalence of CMV colitis in cases of acute exacerbation was 5.4% (two cases) compared to 0% in controls. This however, was not stastistically significant, given the relatively small sample size. The reduced prevalence of CMV in our study may be due to the small sample size, reduced number of steroid dependent cases or the reduced severity of our cases.
Conclusion
Clinical and endoscopic disease severity indicators can be used as predictors of histological activity in ulcerative colitis. Poor treatment compliance and stress are important risk factors for acute exacerbation of ulcerative colitis. Clinicians should be aware of the possibility of concurrent CMV infection while treating patients with acute exacerbation of ulcerative colitis not responding to the conventional management. Reduced prevalence of CMV colitis in cases of acute exacerbation of ulcerative colitis in our study may be due to the small sample size, reduced number of steroid dependent cases or reduced severity of our cases.
Limitation Future Implications
Mucosal biopsies were only examined for this study, so there is chance of probable sampling error. Due to financial constraints PCR on biopsy samples could not be performed. A negative mucosal biopsy for CMV only rules out CMV gastrointestinal disease, it does not rule out CMV systemic disease.
An international agreement should be formed as to which index or combinations of indices to be used for assessing disease activity. Advances in molecular medicine with regard to genetic and etiologic factors in IBD may result in identification of better markers for the disease. A consensus on gold standard diagnostic tool for detection of CMV infection in Ulcerative colitis has to be designed. These will help the clinician to provide appropriate treatment to their patients.
chi square-test is used
chi square-test is used
chi square-test is used
chi square-test is used
chi square-test is used