Head and neck cancer consists of a heterogeneous group of lesions that arise in the upper aero digestive tract. It is the sixth leading cancer worldwide with approximately 600,000 cases reported annually [1]. Oral cancer is known to account for 2-4% of all cancers worldwide among which Oral Squamous Cell Carcinomas (OSCC) are responsible for 90% of the cancers. Incidence is much higher in many developing countries [2]. Prevalence of oral cancer in India is around 45% [3,4]. Incidence of cancer in India is known to increase from 1 million in 2012 to greater than 1.7 million in the year 2035 as predicted by the international agency for research on cancer [5]. This depicts that death rate in this period caused due to cancer will also increase from 6.8 lacs to 1 million [5].
Tobacco use and alcohol consumption are independent risk factors for development of oral cancer. However, with combined intake, they have a synergistic effect, in development of Head and Neck Squamous Cell Carcinoma (HNSCC) [6,7]. About 7% of all the deaths in India (>= 30 years of age) are due to tobacco intake as per the World Health Organisation (WHO) Global Report on "Tobacco Attributable Mortality" 2012 [8].
Squamous Cell Carcinomas (SCCs) are histologically graded as well, moderate or poorly differentiated carcinomas. Though histological grading system is essential for the classification of HNSCC, but is not necessary for the treatment protocol. This is due to the fact that clinical outcome or treatment response is not strongly associated with differentiation grade [9].
Tumour Lymph Node and Metastases (TNM) staging system is most useful in predicting prognosis and therefore helps to determine patient’s prognosis based on tumour progression, recurrence, disease free survival and response to therapy. It is based on the clinical, radiological and pathological examination. However, it is noted that patients with tumours of same clinico-pathological stage do not have similar disease progression, response to therapy, rate of disease recurrence and survival [1,10]. This is because molecular heterogeneity of HNSCC is not incorporated in conventional TNM classification. Therefore there is a dire need to understand the prognostic relationship of HNSCC with various molecular markers that have been discovered in the last few years and which have potentially offered new methods for early diagnosis and treatment alternatives. Hence, this study has been undertaken to evaluate expression of cyclin D1 in HNSCC cases and find out its association with various pathological prognostic factors.
Cyclin D1 plays an important role in activation of cell cycle progression and is amplified in 30% to 50% of HNSCC patients hence its overexpression shortens G1 phase of the cell cycle [9]. Cyclin D1 abnormalities result from genomic inversion, translocation or gene amplification [2]. Most commonly reported alteration is gene amplification of CCND1 which correlates significantly with tumour extension, regional lymph node metastases and advanced clinical stage of HNSCC [10]. According to few studies, HNSCC cases have shown resistance to Epidermal Growth Factor Receptor (EGFR) inhibitors which has been attributed to deregulated cyclin D1 overexpression. Hence role of cyclin D1 warrants additional analysis in HNSCC patients, for its utility as a prognostic marker and in determining the response to treatment.
Materials and Methods
The study was conducted in the Department of Pathology in collaboration with ENT Department, Motilal Nehru Medical College, Allahabad during the period of Jun 2014-2015 and included 48 cases diagnosed and operated for HNSCC. HNSCC cases were mainly confined to the oral cavity (lip, buccal mucosa, tongue, gingivobuccal sulcus). Cases in which only a biopsy or limited surgery had been done, cases diagnosed other than SCC and tumours with extensive necrosis with insufficient viable tumour cells for accurate evaluation were all excluded from the study.
Specimens received were fixed in 10% (v/v) formalin. In each case we followed the standard American Joint Committee on Cancer (AJCC) criteria for grossing of the surgical specimens. After conventional processing, paraffin sections of 3-4μm thickness were stained by Haematoxylin and Eosin (H&E) for diagnosing, grading and staging of the tumour. Tumours were graded according to Broder’s criteria into well, moderate and poorly differentiated [11]. Also, 4μm sections from paraffin embedded tumour tissue were taken on the glass slides which were precoated with adhesive (silane) for Immunohistochemistry (IHC).
Immunohistochemistry
IHC was carried out using Rabbit monoclonal anti-Cyclin D1 clone EPR2241 (IHC)-32 (BioGenex, Fremont CA). It forms serine / threonine kinase holoenzyme complex and functions as a regulatory subunit of CDK4 or CDK6, phosphorylates, inactivates Rb protein and promotes progression through the G1/S phase. Tonsillar tissue was taken as control. The tissue samples were considered positive for cyclin D1 when distinct brown nuclear staining was detected in ≥1% of the cells [12]. Cytoplasmic staining was disregarded. Total number of cells showing positivity for cyclin D1 was counted using pinhole method [12].
Percentage of cells stained was scored as Expression Score (ES) [Table/Fig-1]. The staining intensity was compared with IHC stained sections of tonsillar tissue taken as positive control and recorded as Intensity Score (IS) [Table/Fig-2]. Finally, Total Score (TS) was calculated by multiplying ES with IS to produce a semi quantitative immunohistochemical score, which was graded [Table/Fig-3].
Expression score of cyclin D1 staining according to percentage of cells stained.
| Expression Score | % of cells stained |
|---|
| 1 | 1 - 25% |
| 2 | 26-50% |
| 3 | 51-75% |
| 4 | >75% |
Intensity score of cyclin D1 expression according to the intensity of staining.
| Intensity Score | Intensity of staining |
|---|
| 1 | mild |
| 2 | moderate |
| 3 | strong |
Grading of total score of Cyclin D1 expression (TS=ES x IS).
| Total Score | Grading |
|---|
| 1–4 points | + weak |
| 5–8 points | ++ moderate |
| 9–12 points | +++strong |
Scoring criteria for cyclin D1 immunoreactivity were based on previous scoring methods used by Saawarn et al., [12]. The study had been conducted after ethical clearance by Institutional ethical committee.
Statistical Analysis
Data obtained were analysed and finally transported to the excel sheet. Chi-square test with and without Yate’s correction was used to compare various parameters. The p-value ≤ 0.05 was taken as critical level of significance.
Results
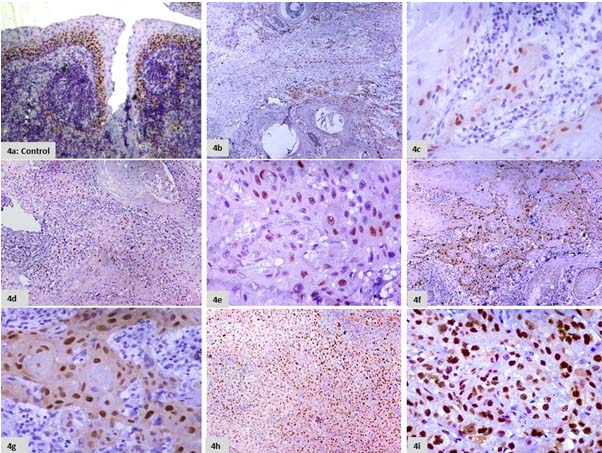
Tonsillar tissue taken as control showed brown nuclear staining which was confined to the proliferating basal and parabasal layers of the epithelium [Table/Fig-4a]. Cyclin D1 staining in the tumour sections was scored as per the percent of cells stained and was assigned as ES [Table/Fig-4b-i]. The intensity of nuclear staining was scored as IS [Table/Fig-5a-c]. Total Score of Cyclin D1 expression was evaluated for each SCC case by (ES x IS) and the case distribution based on total scoring was done [12] [Table/Fig-6].
a) Section of tonsillar tissue taken as control showing cyclin D1 expression confined to the basal layers of the epithelium.(IHC, 10X). b) Section showing cyclin D1 positivity in <25% of the tumour cells. (ES 1; IHC, 10X). c) Section showing cyclin D1 positivity in <25% of the tumour cells. (ES 1; IHC, 40X). d) Section showing cyclin D1 positivity in 25-50% of the tumour cells. (ES 2; IHC, 10X). e) Section showing cyclin D1 positivity in 25-50% of the tumour cells. (ES 2; IHC, 40X). f) Section showing cyclin D1 positivity in 50-75% of the tumour cells. (ES 3; IHC, 10X). g) Section showing cyclin D1 positivity in 50-75% of the tumour cells. (ES 3; IHC, 40X). h) Section showing cyclin D1 positivity in >75% of the tumour cells. (ES 4; IHC, 10X). i) Section showing cyclin D1 positivity in >75% of the tumour cells. (ES 4; IHC, 40X).
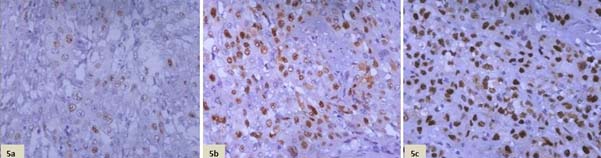
a) Section showing mild intensity of cyclin D1 staining. (IS 1; IHC, 40X). b) Section showing moderate intensity of cyclin D1 staining. (IS 2; IHC, 40X). c) Section showing strong intensity of cyclin D1 staining. (IS 3; IHC, 40X).
Case distribution based on total score.
| Total Score | Grade | N (%) |
|---|
| 1-4 | Weak | 21(43.75) |
| 5-8 | Intermediate | 18(37.5) |
| 9-12 | Strong | 9(18.75) |
N = No. cases out of 48 that lied in each grading category
Correlation of total score of Cyclin D1 expression with various pathological prognostic factors including Grade, Stage and Lymph node metastasis:
Association between T.S. of cyclin D1 and tumour grades was analysed and we found that maximum number of cases 16/34(47%) of grade I, showed weak cyclin D1 expression [Table/Fig-7,8].
Distribution of cases based on T.S. of cyclin D1 with tumour grade.
| CYCLIND1(T.S.) | 1-4(Weak)n (%) | 5- 8(Intermediate)n(%) | 9-12(Strong)n(%) | Total |
|---|
| Grade | n(%) |
|---|
| WDSCC | 16(33.33) | 12(25) | 6(12.5) | 34(70.8) |
| MDSCC | 5(10.42) | 5(10.42) | 3(6.3) | 13(27.1) |
| PDSCC | 0(0) | 1(2.1) | 0(0) | 1(2.1) |
| Total | 21(43.8) | 18(37.5) | 9(19) | 48(100) |
WD- Well Differentiated, MD- Moderately Differentiated, PD- Poorly Differentiated
Distribution of cases based on T.S. of cyclin D1 with tumour grade.
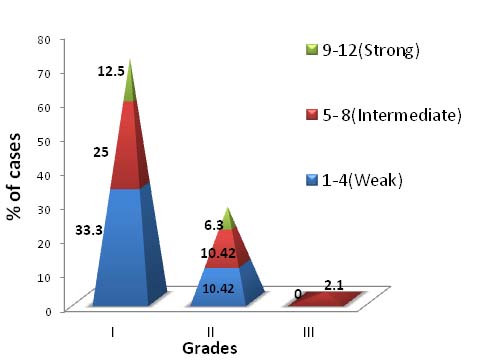
The association between T.S. of cyclin D1 expression and tumour grades was not statistically significant (p=0.73).
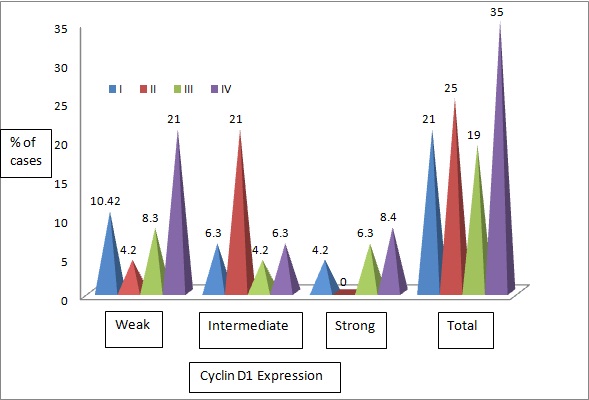
Association between T.S. of cyclin D1 and tumour stages was evaluated and we saw that out of 17 cases in stage IV, maximum 10/17(58.8%) expressed weak cyclin D1 expression. Out of 9 cases that showed strong expression maximum 4/9(44.4%) cases were from stage IV [Table/Fig-9,10]. The association between T.S of cyclin D1 expression and tumour stage was statistically significant. (p=0.02).
Distribution based on T.S. of cyclin D1 with tumour stage.
| CYCLIND1(T.S.) | 1-4(Weak)n(%) | 5- 8 (Intermediate)n(%) | 9-12 (Strong) n(%) | Total |
|---|
| Stage | n(%) |
|---|
| I | 5(10.42) | 3(6.3) | 2(4.2) | 10(21) |
| II | 2(4.2) | 10(21) | 0(0) | 12(25) |
| III | 4(8.4) | 2(4.2) | 3(6.3) | 9(19) |
| IV | 10(21) | 3(6.3) | 4(8.4) | 17(35) |
| Total | 21(43) | 18(38) | 9(19) | 48(100) |
Distribution based on T.S. of cyclin D1 with tumour stage.
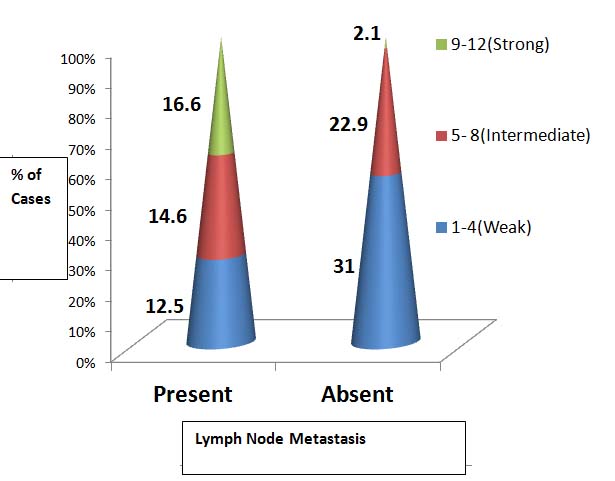
On evaluating association between T.S of cyclin D1 and Lymph Node metastasis we found that out of 21 cases with lymph node metastasis, about 8/21(38.1%) showed strong cyclin D1 expression. Similarly out of 27 cases without lymph node metastasis, maximum 15/27 (55.5%) showed weak expression [Table/Fig-11,12]. A statistically significant association was seen between cyclin D1 expression with lymph node metastasis (p=0.008).
Case Distribution based on Total Score (T.S.) of Cyclin D1 with Lymph Node Metastasis.
| CYCLIN D1(T.S.) | 1-4(Weak)n (%) | 5- 8(Intermediate)n(%) | 9-12(Strong)n(%) | Total |
|---|
| Lymph Node Metastasis | n(%) |
|---|
| Present | 6(12.5) | 7(14.6) | 8(16.6) | 21(43.7) |
| Absent | 15(31) | 11(22.9) | 1(2.1) | 27(56.3) |
| Total | 21(43.7) | 18(25) | 9(31.3) | 48(100) |
Case distribution based on T.S. of cyclin D1 with lymph node metastasis.
Discussion
Oropharyngeal cancers are a heterogeneous group of malignancies in terms of aetiology, biological behaviour and prognosis. Over the years TNM staging has been the most useful indicator to predict the prognosis in patients with oropharyngeal carcinoma. In the recent years several attempts have been made by researchers, across the globe, to find immunohistochemical markers that can be used either independently or in conjunction with TNM staging, to predict the outcome of these cancers.
Out of total 48 cases in our study, majority 21(43.75%) showed weak cyclin D1 expression followed by 18(37.5%) cases which showed intermediate and 9(18.8%) showed strong expression. Das S et al., conducted a study on 45 cases and found that 66.6% cases showed cyclin D1 positivity [13]. Among them 20/45 cases (44.4%) showed high cyclin D1 expression, 10(22.2%) showed moderate and 15 (33.3%) cases showed either low or no expression. In our study the combined intermediate and strong expression was (27/48)56.25%. Thus our study was in concordance with their study.
A study conducted by Saawarn et al., on 40 biopsy specimens of OSCC cases showed cyclin D1 expression in 45% of the cases [12]. Cyclin D1 expression was weak in majority of the cases, followed by strong and intermediate which was similar to our study.
We evaluated the significance of association between Total Scores of cyclin D1 expression and grade of the tumour [Table/Fig-7,8]. The result did not show a statistical significant association between them (p=0.73). Our study was in accordance to study by Feng Z et al., which also showed no significant association with tumour grade [14]. Whereas, our study was discordant to studies by (p<0.001), Saawarn et al., Das et al., Zhao et al., and Bova et al., in which there was a significant correlation with tumour grade [12,13,15,16].
We did comparative analysis of cyclin D1 expression with tumour stage [Table/Fig-9,10]. We found that there was a significant association of cyclin D1 expression with tumour stage (p=0.02). These finding were in accordance to studies conducted by Das et al., (p<0.02) Zhao et al., and Angela et al, (p=0.004) as they also observed a significant association of cyclin D1 expression with tumour stage [13,15,17]. Whereas, findings of Saawarn et al., and Feng Z et al., showed no significant correlation with tumour stage [12,14].
We also interpreted the association of cyclin D1 expression with lymph node metastasis [Table/Fig-11,12] and found that there was a significant association. (p=0.008). Studies by Das et al., Zhao et al., were consistent with our study which showed that cyclin D1 expression was associated with lymph node metastasis (p=0.001) [13,15].
Conclusion
Staging and grading are, till date, the most important parameters that helps to understand the possible outcome of patients diagnosed with malignancy. In this study, we have tried to find out the association of cyclin D1 expression, marker that is now routinely used, with different tumour stages and grades, in OSCC patients. Our study has focussed primarily on the role of cyclin D1 in HNSCC. In most of the studies, CCND1 aberration has been proved as a prognostic marker for disease-free survival and overall survival in HNSCC patients. Deregulated cyclin D1 overexpression is associated with resistance of HNSCC to EGFR inhibitors. Therefore, findings of this study will be an important adjunct, along with staging and grading, to determine the prognosis and also to design the treatment options that would lead to lesser morbidity and increased survival of patients with OSCC.
N = No. cases out of 48 that lied in each grading category
WD- Well Differentiated, MD- Moderately Differentiated, PD- Poorly Differentiated