Most commonly used diagnostic aids of the Temporomandibular Joint (TMJ) in Orthodontic practices are panoramic radiographs, transcranial projections, and tomography because of their avail-ability, ease of use, relatively low radiation requirement, and low cost. Katsavrias and Halazonetis advocated that the mandibular fossa and condyle varied in shape in patients with different types of malocclusion [1]. The interpretation of the condyle-fossa relationship on the radiographs is challenging, as there will be differing references and patient positioning. Although many investigators used panoramic radiographs to assess changes in the condyles from functional appliances [2] and other orthodontic treatments [3,4], the inherent anatomic diversity of the TMJ articulation, compounded by factors that influence 2D image presentation (e.g., anatomic superimposition, beam projection angle, and patient positional changes), throw into doubt the validity of those studies. Computed Tomography (CT) provides optimal imaging of the osseous components of the TMJ with 87.5% to 96% [2] accuracy in detecting degenerative arthritis.
The morphology of TMJ is influenced by the functional loads. The loads, to which TMJs are submitted, vary according to the subject’s dentofacial morphologies, suggesting the morphological difference of condyle and the mandibular fossa in subjects with various malocclusion patterns [5,6].
The relationship between occlusal factors and joint morphology is contradictory, some studies showed a significant relationship [5–7] whereas others failed to demonstrate a correlation [8–15].
Materials and Methods
The study was a cross-sectional study. The purposive sampling of 60 patients was done, with age group of 18 -30 years. The subjects were randomly selected from the patients attending Mamata Dental College and Medical College, Khammam, Telangana, India, during the year 2011 to 2013. The CT scan for the patients with the normal occlusion was obtained after explaining the procedures involved in the study. Most of these patients attended medical college for treatments in the maxillofacial region other than the TMJ. The CT scan of the patients with malocclusion was obtained from the patients who attended to orthodontic department for correction of malocclusion. Informed consent was obtained from all the patients. Institutional Ethical committee clearance was obtained for conducting the study (MDC126226041wide Lr. No. 521/A7/MDS/Diss/2009-12, dated 19-11-2009.) The sample was categorized into 3 groups, based on overbite and growth pattern. The criteria for overbite included subjects having overbite range of 4-6mm and without crowding. Using a sharp, nontoxic marking pencil the overbite was measured. While the subject’s TMJ was comfortably closed, a horizontal line was marked on the lower incisor at the level of the upper incisors. Then the subject was asked to open the mouth half way, so as to record the vertical measurement between the superior aspect of the lower incisors and the line that was marked. The groups included 20 subjects with normal occlusion, 20 patients with horizontal growth pattern and deep bite, 20 patients with vertical growth pattern and deep bite. The patients were selected according to following criteria: No history of previous orthodontic treatment, without any functional mandibular deviations, without missing teeth except third molars. The patients having restricted mouth opening, mandibular deviations, missing teeth other than third molars and the patients having parafunctional habits were excluded from the study.
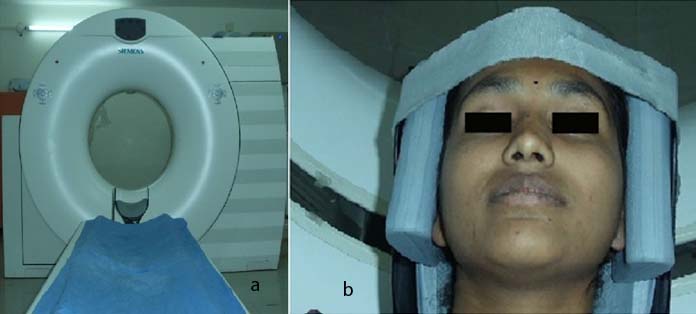
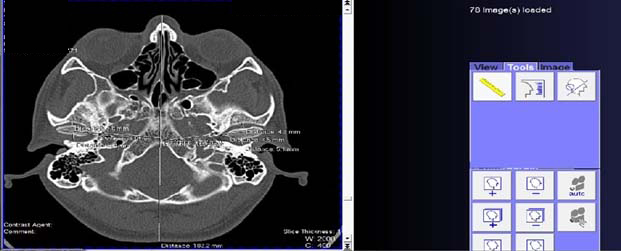
Spiral CT was performed with SIEMENS, (Somatom Emotion machine, Germany). The CT images were obtained with the patients in maximum dental intercuspation, and their heads were positioned so that the Frankfort and midsagittal planes were perpendicular to the floor as shown in [Table/Fig-1]. The scans were performed using 60 Kvp, 30mA, thickness 1mm spaced at 2.5mm intervals as shown in [Table/Fig-2]. The linear and angular measurements were made directly off the scan monitor upon digitizing the appropriate landmarks as shown in [Table/Fig-3] by using syngo fast View software.
(a) Computed Tomography machine used in the study; (b) Position of the patient in computed tomographic machine.
(a) Sagittal section of TMJ; (b) Coronal section of TMJ.
Measurements being done on monitor by using syngofastview software.
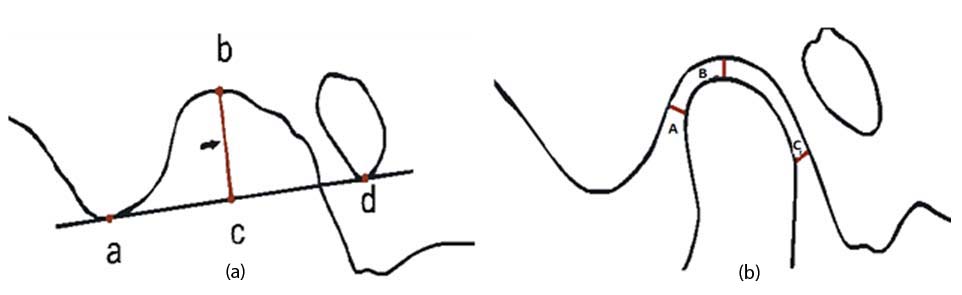
The following measurements were assessed on the sagittal plane. Depth of the mandibular fossa (VD) i.e., the superior point of the fossa to the plane formed by the most inferior point of the articular tubercle to the most inferior point of the auditory meatus, Anterior Joint Space (AJS) i.e., the shortest distance between the most anterior point of the condyle and the posterior wall of the articular tubercle, Posterior Joint Space (PJS) i.e., the shortest distance between the most posterior point of the condyle and the posterior wall of the mandibular fossa, Superior Joint Space (SJS) i.e., the shortest distance between the most superior point of the condyle and the most superior point of the mandibular fossa [Table/Fig-4].
(a) Depth of the mandibular fossa; a-Most inferior point of the articular tubercle; b- Most superior point of the fossa; c- Point of intersection from a perpendicular dropped on line a-d from point b; d- Most inferior point of auditory meatus. The vertical distance b-c is the depth of the mandibular fossa; (b) Concentric position of the Condyle; A- Anterior joint space; B- Superior joint space; C- Posterior joint space.
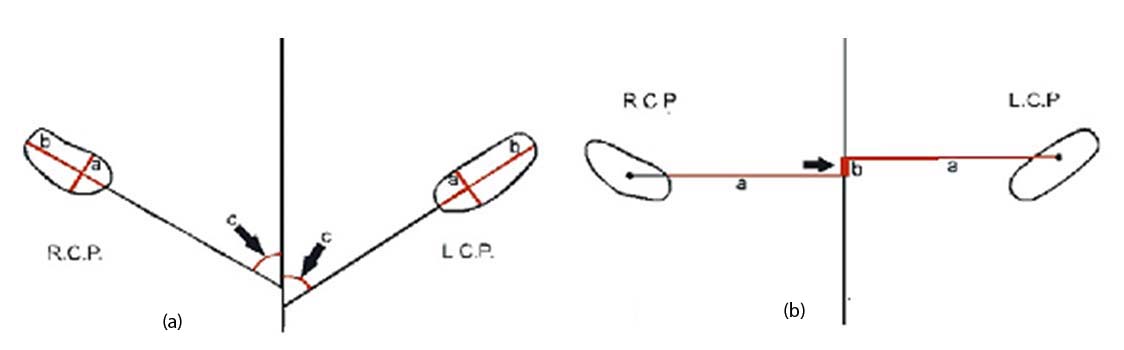
The following measurements were assessed on the axial plane. The greatest Antero-Posterior Diameter (APC) of the mandibular condylar processes, the greatest Medio-lateral Diameter (MLC) of the mandibular condylar processes, the angle between the long axis of the mandibular condylar process and the mid-sagittal plane (AG), the distance between the geometric centers of the condylar processes and the mid sagittal plane (CDMS), measured with a line that passed through the geometric centers of the condylar processes and perpendicular to the mid sagittal plane and the antero-posterior difference (AP) between the geometric center of the right and left condylar processes as reflected on the mid sagittal plane [Table/Fig-5].
(a) Axial section of CT image; Measurement of diameters of mandibular condylar processes: a- greatest anteroposterior diameter; b-greatest mediolateral diameter and; c- The angle (AG) between the long axis of the mandibular condylar process and the mid sagittal plane; (b) Axial section of CT image; Measurement of perpendicular distance between the geometric centers of the condylar processes and the mid sagittal plane (CDMS); a- the distance between the geometric center of the condylar processes to the midsagittal plane and; b- anteroposterior difference of the condylar processes. MSP-midsagittal plane; LCP- left condylar process; RCP- right condylar process.
Data analysis was performed in SPSS version 14. A p-value of <0.05 was set to be statistically significant. ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
Results
The descriptive statistics of each measurement for average growers, horizontal growers with deep bite, and vertical growers with deep bite are shown in [Table/Fig-6,7 and 8], respectively. The descriptive statistics of concentric position of condyles of the three groups are shown in [Table/Fig-9]. In average growers and horizontal growers there was no significant difference in the mean AJS for right side and left side (1.91±0.69 and 2.01±0.7) (2.05±0.70 and 2.17±0.75) (p<0.001), PJS for right and left side (1.95±0.76 and 2.04±0.66) (2.02±0.55 and 2.06±0.53) (p<0.001), SJS for right and left side (2.70±0.73 and 2.70±0.76) (2.82±0.95 and 2.75±1.20) (p<0.001), VD for right and left side (8.32±1.14 and 8.3±1.24) (8.36±1.08 and 8.61±1.43) (p<0.001), APC for right and left side (8.02±1.45 and 8.01±1.50) (7.30±1.17 and 7.71±0.83) (p<0.001), MLC for right and left side (19.46±2.03 and 19.02±1.83) (18.47±1.94 and 18.10±2.20) (p<0.001), Angle for right and left side (60.12±7.09 and 59.18±7.01) (62.29±7.49 and 61.90±6.81) (p<0.001). The mean CDMS score was significantly higher for right side than left side (p<0.001) in average growers, it is not significantly high in horizontal growers as shown in [Table/Fig-6,7].
The descriptive statistics of each measurement for average growth pattern.
| Group | | Right | Left | p-value | R | p*-value |
|---|
| Mean | SD | Mean | SD |
|---|
| AverageGrowthPattern | AJS | 1.91 | 0.69 | 2.01 | 0.70 | 0.21 | 0.87 | <0.001 |
| PJS | 1.95 | 0.76 | 2.04 | 0.66 | 0.28 | 0.86 | <0.001 |
| SJS | 2.70 | 0.73 | 2.70 | 0.76 | 0.96 | 0.80 | <0.001 |
| VD | 8.32 | 1.14 | 8.33 | 1.24 | 0.98 | 0.67 | <0.001 |
| APC | 8.02 | 1.45 | 8.01 | 1.50 | 0.98 | 0.76 | <0.001 |
| MLC | 19.46 | 2.03 | 19.02 | 1.83 | 0.11 | 0.81 | <0.001 |
| Angle AG | 60.12 | 7.09 | 59.18 | 7.01 | 0.58 | 0.42 | 0.07 |
| AP | 0.00 | 0.00 | 1.54 | 2.33 | 0.01 | . | . |
| CDMS | 51.15 | 4.04 | 46.78 | 2.90 | 0.00 | 0.10 | 0.68 |
A p-value of <0.05 is set to be statistically significant.
(AJS-Anterior Joint Space; PJS- Posterior Joint Space; SJS- Superior Joint Space; VD-Depth of the mandibular fossa; APC: The greatest anteroposterior diameter of the mandibular condylar processes; MLC- The greatest mediolateral diameter of the mandibular condylar processes; AP- The anteroposterior difference between the geometric center of the right and left condylar processes; Angle AG- The angle between the long axis of the mandibular condylar process and the mid sagittal plane; CDMS- The distance between the geometric centers of the condylar processes and the mid sagittal plane)
Descriptive statistics of each measurement for horizontal growth pattern with deep bite. ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
| Group | | Right | Left | p-value | R | p*-value |
|---|
| Mean | SD | Mean | SD |
|---|
| HorizontalGrowthPattern | AJS | 2.05 | 0.70 | 2.17 | 0.75 | 0.30 | 0.76 | <0.001 |
| PJS | 2.02 | 0.55 | 2.06 | 0.53 | 0.71 | 0.62 | <0.001 |
| SJS | 2.82 | 0.95 | 2.75 | 1.20 | 0.64 | 0.81 | <0.001 |
| VD | 8.36 | 1.08 | 8.61 | 1.43 | 0.26 | 0.72 | <0.001 |
| APC | 7.30 | 1.17 | 7.71 | 0.83 | 0.20 | 0.06 | 0.79 |
| MLC | 18.47 | 1.94 | 18.10 | 2.20 | 0.43 | 0.52 | 0.02 |
| Angle AG | 62.29 | 7.49 | 61.90 | 6.81 | 0.79 | 0.62 | <0.001 |
| AP | 0.00 | 0.00 | 1.30 | 3.20 | 0.09 | . | . |
| CDMS | 49.04 | 5.07 | 47.63 | 4.57 | 0.34 | 0.10 | 0.68 |
ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
A p-value of <0.05 is set to be statistically significant.
(AJS-Anterior Joint Space; PJS- Posterior Joint Space; SJS- Superior Joint Space; VD-Depth of the mandibular fossa; APC: The greatest anteroposterior diameter of the mandibular condylar processes; MLC- The greatest mediolateral diameter of the mandibular condylar processes; AP- The anteroposterior difference between the geometric center of the right and left condylar processes; Angle AG- The angle between the long axis of the mandibular condylar process and the mid sagittal plane; CDMS- The distance between the geometric centers of the condylar processes and the mid sagittal plane).
Descriptive statistics of each measurement for vertical growth pattern with deep bite.
| Group | | Right | Left | p-value | R | p*-value |
|---|
| Mean | SD | Mean | SD |
|---|
| VerticalGrowthPattern | AJS | 2.48 | 0.69 | 2.32 | 0.67 | 0.05 | 0.88 | <0.001 |
| PJS | 1.68 | 0.50 | 1.78 | 0.50 | 0.31 | 0.63 | <0.001 |
| SJS | 2.63 | 1.01 | 2.68 | 0.98 | 0.60 | 0.91 | <0.001 |
| VD | 8.27 | 1.11 | 8.45 | 1.07 | 0.40 | 0.65 | <0.001 |
| APC | 7.31 | 1.10 | 7.64 | 1.04 | 0.02 | 0.86 | <0.001 |
| MLC | 18.13 | 2.29 | 17.91 | 2.00 | 0.41 | 0.85 | <0.001 |
| Angle AG | 62.34 | 8.28 | 61.59 | 7.48 | 0.65 | 0.58 | 0.01 |
| AP | 0.00 | 0.00 | 0.53 | 2.18 | 0.30 | . | . |
| CDMS | 51.07 | 3.01 | 47.46 | 3.74 | 0.00 | 0.25 | 0.28 |
ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
A p-value of <0.05 is set to be statistically significant.
(AJS-Anterior Joint Space; PJS- Posterior Joint Space; SJS- Superior Joint Space; VD- depth of the mandibular fossa;APC: The greatest anteroposterior diameter of the mandibular condylar processes; MLC- The greatest mediolateral diameter of the mandibular condylar processes; AP- The anteroposterior difference between the geometric center of the right and left condylar processes; Angle AG- The angle between the long axis of the mandibular condylar process and the mid sagittal plane; CDMS- The distance between the geometric centers of the condylar processes and the mid sagittal plane)
Descriptive statistics of concentric position of condyles in average, horizontal and vertical groups.
| Group | | AJS | PJS | AJS-PJS | p- value | R | p*-value |
|---|
| Mean | SD | Mean | SD | Mean | SD |
|---|
| Average | Right | 1.91 | 0.69 | 1.95 | 0.76 | -0.04 | 0.79 | 0.823 | 0.407 | 0.075 |
| Left | 2.01 | 0.70 | 2.04 | 0.66 | -0.03 | 0.89 | 0.862 | 0.158 | 0.507 |
| Horizontal | Right | 2.05 | 0.70 | 2.02 | 0.55 | 0.03 | 1.05 | 0.9 | -0.416 | 0.068 |
| Left | 2.17 | 0.75 | 2.06 | 0.53 | 0.11 | 1.02 | 0.635 | -0.23 | 0.329 |
| Vertical | Right | 2.48 | 0.69 | 1.68 | 0.50 | 0.80 | 0.78 | <0.001 | 0.156 | 0.510 |
| Left | 2.32 | 0.67 | 1.78 | 0.50 | 0.54 | 0.89 | 0.014 | -0.153 | 0.519 |
ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
A p-value of <0.05 is set to be statistically significant.
AJS- anterior joint space; PJS- Posterior Joint Space; AJS-PJS- difference between AJS and PJS.
Vertical growers with deep bite showed a significant difference in the mean AJS for right side and left side (2.48±0.69 and 2.32±0.67 respectively) (p<0.001), APC for right and left side (7.31±1.10 and 7.64±1.04 respectively) (p<0.001), the mean CDMS score was significantly higher for right side than left side (p<0.001). There was no significant correlation between right and left side CDMS (p=0.28) as shown in [Table/Fig-8].
In the evaluation of the concentric position of the condyles vertical growers with deep bite showed significantly higher mean AJS than PJS in both right (2.48±0.69 and 1.68±0.5) and left sides (2.32±0.67 and 1.78±0.5) (p<0.001 and 0.014 respectively), although there was no significant correlation between AJS and PJS scores in both right and left sides (p=0.51 and 0.519 respectively) as shown in [Table/Fig-9].
Discussion
TMJ is considered to be an important factor in orthodontic treatment, perfect positioning of the condyle in the glenoid fossa is very important to maintain functional balance, the change in position of the condyle leads to displacement of disc either anteriorly or posteriorly causing disc derangements. CT imaging has been shown to be one of the ideal tools for TMJ assessment. Three-dimensional information evaluated from a series of thin slices of the internal structure eliminates superimposition, offers higher sensitivity during differentiation of tissues when compared with conventional radiography and it also allows manipulating and adjusting the image after scanning [19].
In this study, CT was chosen to evaluate the condyle fossa relationship of the TMJ because it is the best examination tool for visualization of articular skeletal anatomy. According to Vitral RW et al., [20], CT of the TMJ shows the details of bony structures.
The axial slice is the most appropriate method to assess the position of the condyles in both anteroposterior and mediolateral aspects as it shows both condyles in the same image.
Cohlmia et al., [17] conducted a study to evaluate the morphologic relationship of condyle and fossa in patients with different maloc-clusions and skeletal pattern. They concluded that the left condyle was found to be more anteriorly positioned than the right. There were no significant differences in condylar position between class I and class II groups but skeletal and dental class III patients had significantly more anteriorly positioned condyles. So in the present study, skeletal base was not taken into consideration.
Wood et al., [21], studied on different incisal biting forces and condylar seating, they concluded that biting force significantly affected the condylar movement. Deep overbite and Class II malocclusion are commonly represented in TMJ patient populations with deep bite as a cause of posterior condylar displacement, disk laxity, TMJ clicking, and pain [12], so considering these factors, in the present study deep bite is taken into consideration to evaluate the relation between deep bite and condyle fossa relationship.
Considerable difference in skeletal form between the hyper and hypodivergent facial patterns is that the anatomical constraints of the hyperdivergent pattern would dictate condylar function further out of the fossa. Rationally it advocates that the unfavorable anterior or posterior facial height ratio ensures greater condylar distraction (especially in the vertical dimension) so as to bring anterior teeth to functional contact [22].
The purpose of this study was to compare the condylar symmetry and condylar-fossa relationship in horizontal and vertical growers with deep bite. The results of our study did not show any statistical significance in the symmetry of right and left condylar processes in all the groups. This is in accordance with Vitral et al., [16], Gianelly et al., [23], Rodrigues et al., [24]. Vitral and Telles [18] found similar results in a Class II Division 1 subdivision sample with deep bite whereas, Anthony A. Gianelly et al., [23], found a similar result in class II deep bite non overjet malocclusions and Rodrigues et al., [24], found same results in Class I malocclusion patients. These results seem to confirm the statement of Masi et al., [25] that the occlusal features might be associated with TMJ structure remodeling to create symmetrical relationships.
The present study results showed a significant reduction in the angulation of left condyle to the midsaggital plane compared to the right in two groups (i.e., average, horizontal deep bite (p=0.01, p=0.09) which indicate that left condyle is more anteriorly placed whereas, in vertical deep bite sample there is no much difference observed (p=0.01, p=0.09, p=0.30), this is in accordance with Cohlmia et al., [17], study who found that the left condyle was more anteriorly placed than the right and this asymmetry may be related to normally occurring cranial base asymmetries and side preferences during mastication.
The present study results showed that there is no significant change in condylar position in horizontal deep bite patients. This is in accordance with Gianelly et al., [23], who studied the positions of the condyles in glenoid fossa in Class II malocclusions characterized by a bite depth and an inter-incisal angle and they concluded that there is no significant correlation was noted in condylar position (concentric position of condyle in fossa) related to bite depth.
In the present study, the three groups showed non-concentric positioning of the condyle bilaterally, but vertical growers showed significant non concentrism. In this study there is no significant difference between right and left concentric positioning of the condyles in 3 groups. The present study results are in accordance with Rodrigues et al., [24]. They conducted a study to investigate the positioning of the condyles in glenoid fossa, and compared the variation in positioning between right and left condyles in subjects with Class I malocclusion and they concluded that there is nonconcentric positioning of the condyles on either side.
The present study results showed a statistically significant change in position of condyle in vertical grower, this is in accordance with Girardot [22]. He compared the condylar position in hyperdivergent and hypodivergent facial skeletal types and concluded that there was a statistically significant greater distraction of the condyles in the hyperdivergent group in both the horizontal and vertical planes.
In the present study, only the vertical growers with deep bite showed significant change in position of the condyle. This is in accordance with Pullinger et al. [13], study who investigated the influence of occlusion on condylar position as seen on TMJ tomograms in a group of 44 young adults with no history of orthodontic or occlusal therapy and no objective signs of masticatory dysfunction and concluded that there is no correlation between the degree of overbite or overjet and the measured condylar position.
The present study confirms nonconcentric positioning of condyles in all the three groups and significant non concentrism of the condyle in vertical group compared to other groups. There is no significant change in the vertical depth of the condyle in all the three groups. Left condyle is more anteriorly placed than right condyle in vertical growers.
Limitation
The statistical evaluation for the sample size determination was not done hence purposive sampling was done. Magnetic Resonance Imaging (MRI) aids in clear vizualisation of disc, so in this aspect MRI can be used to assess disc derangements. Open bite patients were not considered in the study.
Conclusion
No significant change was seen in the position of the condyles in average growers with normal overbite and horizontal growers with deep bite. There is a significant change in the position of the condyle (decreased posterior joint space indicating posterior positioning of the condyle in fossa) in vertical growers compared to average and horizontal growers. Left condyle is more anteriorly placed than the right condyle in all the three groups. There is no significant change in the vertical depth of the mandibular fossa in all the three groups. There is no significant change in symmetry of the condyles when compared to right and left side.
The findings suggest that there is a condylar positional change only in vertical growers with deep bite, when compared to average growers with normal bite and horizontal growers with deep bite. This suggests that the effect of anterior deep bite does not affect the condylar position but the growth pattern has an influence on condylar position.
A p-value of <0.05 is set to be statistically significant.
(AJS-Anterior Joint Space; PJS- Posterior Joint Space; SJS- Superior Joint Space; VD-Depth of the mandibular fossa; APC: The greatest anteroposterior diameter of the mandibular condylar processes; MLC- The greatest mediolateral diameter of the mandibular condylar processes; AP- The anteroposterior difference between the geometric center of the right and left condylar processes; Angle AG- The angle between the long axis of the mandibular condylar process and the mid sagittal plane; CDMS- The distance between the geometric centers of the condylar processes and the mid sagittal plane)
ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
A p-value of <0.05 is set to be statistically significant.
(AJS-Anterior Joint Space; PJS- Posterior Joint Space; SJS- Superior Joint Space; VD-Depth of the mandibular fossa; APC: The greatest anteroposterior diameter of the mandibular condylar processes; MLC- The greatest mediolateral diameter of the mandibular condylar processes; AP- The anteroposterior difference between the geometric center of the right and left condylar processes; Angle AG- The angle between the long axis of the mandibular condylar process and the mid sagittal plane; CDMS- The distance between the geometric centers of the condylar processes and the mid sagittal plane).
ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
A p-value of <0.05 is set to be statistically significant.
(AJS-Anterior Joint Space; PJS- Posterior Joint Space; SJS- Superior Joint Space; VD- depth of the mandibular fossa;APC: The greatest anteroposterior diameter of the mandibular condylar processes; MLC- The greatest mediolateral diameter of the mandibular condylar processes; AP- The anteroposterior difference between the geometric center of the right and left condylar processes; Angle AG- The angle between the long axis of the mandibular condylar process and the mid sagittal plane; CDMS- The distance between the geometric centers of the condylar processes and the mid sagittal plane)
ANOVA was performed to assess the significance. If it was found significant, post-hoc Tukey’s test was performed to see which two groups were statistically significant.
A p-value of <0.05 is set to be statistically significant.
AJS- anterior joint space; PJS- Posterior Joint Space; AJS-PJS- difference between AJS and PJS.