Breast carcinoma is the leading cause of death in women, with more than 10 lac cases occurring worldwide annually [1,2]. Early diagnosis and breast conservative surgery lead to good survival rate. Despite of newer imaging techniques, the need for intra-operative consultation of the breast tumour has paved way for the use of IC and FS study. Thereby, the pathologist play a crucial role in the management of this disease [2,3]. In early breast cancer when excision biopsy or lumpectomy is performed without margin evaluation, further, surgery is required if positive margins exist. Repeated operations may cause poor cosmetic appearance, anaesthesia risk, psychological stress, interruption on starting oncological treatments and higher costs. Intra-operative consultation of both IS and FS are critical patient care services provided by histopathologists. Interpretation is an intricate process that requires clinical, laboratory, imaging findings with Histopathologic (HP) knowledge. Key quality components include application, precision, and timeliness [4,5]. IC and FS provide precise results in minutes while the patient is in anaesthesia. IC and FS have a definite role despite the strong popularity of aspiration cytology, when cytological/ core biopsy findings are inconclusive, in the evaluation of lumpectomy margins and intra-operative nodal status [5,6]. Though, FS tissue architecture strongly approximates HP paraffin sections, it is frequently hampered by freezing artifact that, may impair morphologic assessment of the lesion. IC provides better results with crisp cellular details and useful adjunctive technique that complements FS analysis of the lesion at the time of intra operative consultation [5,7]. So both IC and FS are dependable intra operative consultation diagnostic modalities [3,8]. Thus, a study to show features and correlation of results of IC, FS with standard HP diagnosis will be helpful and may allow the procedure to be performed more often.
Materials and Methods
This was a descriptive cross-sectional study conducted in the Department of Pathology, JSS Medical College, JSS University, Mysuru over a period of two years (October 2011- September 2013). A total of 62 cases of surgically resected specimens of breast lesions were studied after obtaining approval from the Institutional Ethical Committee with informed consent of the patients.
Specimens measuring less than 1 cm were excluded. The surgically resected breast specimens were transported immediately to the histopathology laboratory in saline. The specimen was examined grossly for the size of the breast lesion, shape, circumscription, colour, consistency and presence of necrotic, haemorrhagic or cystic areas. The surgical margins and lymph nodes were studied wherever possible. The representative tissue fragment was taken from the lesion and three imprint smears were made by gently rolling the tissue on three glass slides. Two wet fixed smears were immediately fixed in 95% ethyl alcohol and stained with Papanicolaou (PAP), Haematoxylin and Eosin (H&E) and one air dried smear with May Grunwald Giemsa (MGG) stain. The same tissue fragment was subjected to the FS in (LEICA) cryostat at -22°C. The tissue sections were cut at 4 μm thickness and stained with routine H&E stain. Finally, the same tissue was fixed with 10% formalin. Routine HP processing done and sections were stained with H&E stain. The slides prepared by IC, FS and HP were interpreted and analysed by the two pathologists. On IC, lesions were categorized as: i) Inadequate- smears showing mainly RBCs with occasional or no epithelial cells; ii) Negative for malignancy (Benign)- adequacy of smear {Layfield’s cytopathological criteria of adequacy- at least six ductal cell clusters, cumulative total, or the presence of or at least 10 intact bipolar cells per 10 medium power fields (x200)} [9], cellularity with arrangement, bimodal pattern of cells, bare nuclei, cell cohesion, individual cell- N:C ratio, cytoplasm, nuclear features, nucleoli, mitotic figures/10HPF and background stromal fragments. The size of the cell, nuclei and nucleoli were assessed with respect to the size of RBC or small lymphocyte; iii) Suspicious of malignancy- smears showing benign pattern with few atypical cells having high N:C ratio; iv) Positive for malignancy- smears with increased cellularity, large cells, hyperchromatic, pleomorphic nuclei, high N: C ratio and irregular coarse chromatin and necrosis [10]. Subtyping of lesions was done wherever possible.
On FS and HP study, lesions were categorized as benign and malignant. To categorise the lesions as benign and malignant on FS, the following parameters were considered in the sections studied: adequacy, architectural patterns of the lesions and arrangement, N:C ratio, nucleoli, mitosis, bizarre cells, In situ/ invasion, desmoplasia, necrosis, hemorrhage and inflammatory cells, tumour emboli and lymph node metastasis wherever available [3]. If any doubt existed, the diagnosis was deferred to HP paraffin section. Subtyping of the lesions was done on FS in all cases. The results of IC and FS were then correlated with those of final HP report.
Statistical Analysis
All the statistical calculations were done through SPSS for windows (version 16.0). Descriptive statistics such as mean, standard deviation, frequencies, crosstabs (contingency coefficient test) and percentage along with Chi-square test were used to know the association with diagnostic statistics. A p-value of ≤ 0.001 was taken as statistically significant.
Results
Out of the 62 cases of surgically resected breast specimens, the distribution of lesions in IC, FS and HP are shown in [Table/Fig-1]. In IC, one case of inadequate material (1.61%) and no case of suspicious for malignancy was noted. On final HP study, 33(53.23%) cases were diagnosed as malignant lesion and 29(46.77%) as benign lesion.
Distribution of lesions on imprint cytology, frozen section and histopathology.
| Imprint cytology |
| Imprint cytology | Number of cases | % |
| Inadequate | 1 | 1.61 |
| Negative for malignancy(Benign) | 27 | 43.55 |
| Suspicious for malignancy | 0 | 0 |
| Positive for malignancy(Malignant) | 34 | 54.84 |
| Total | 62 | 100 |
| Frozen section |
| Frozen section | Number of cases | % |
| Benign lesions |
| • Non-neoplastic | 8 | 12.90 |
| • Neoplastic | 20 | 32.26 |
| Malignant lesions | 34 | 54.84 |
| Total | 62 | 100 |
| Histopathology |
| Histopathology | Number of cases | % |
| Benign lesions |
| • Non-neoplastic | 8 | 12.90 |
| • Neoplastic | 21 | 33.87 |
| Malignant lesions | 33 | 53.23 |
| Total | 62 | 100 |
Out of 62 cases, 59 (95.2%) were females and three (4.8%) were males. Male: female ratio being 1:19.7. The youngest age in females was 18 years and the oldest was 70 years. The three cases of males affected were of 18 years and 60 years age.
The overall breast lesions were more common in the fourth decade of life (35.5%). Benign lesions were more common in the second decade, while malignant lesions in the fourth decade.
The majority of 54 (87.1%) cases presented with lump in the breast, five (8.1%) cases with recurrent lump, three (4.3%) cases with painful swelling and no case in this study showed nipple discharge. Out of 62 specimens, one (1.61%) was simple mastectomy specimen, 27 (43.55%) were excisional lumpectomies and the remaining 34 (54.84%) were modified radical mastectomy specimens.
Grossly, out of 29 benign lesions, 24(82.8%) cases showed well defined, homogenous and grey white area and five (17.2%) showed ill-defined area with cystic change. Out of 33 malignant lesions, 21(63.6%) were infiltrative with grey white - grey brown area with some showing areas of haemorrhage, necrosis and cystic change three (9.1%). A total of five (15.2%) lesions were well defined and four (12.1%) were ill defined.
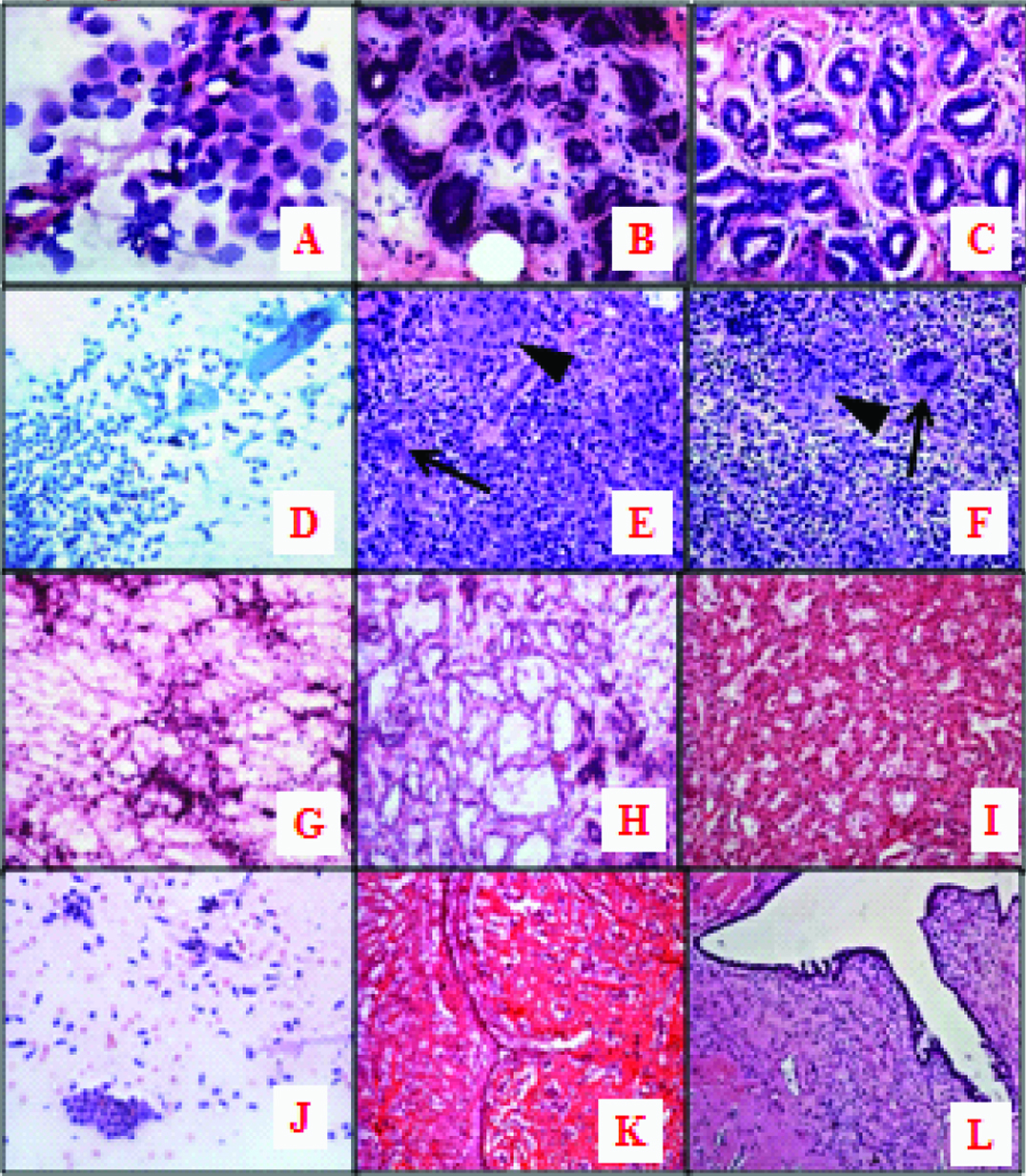
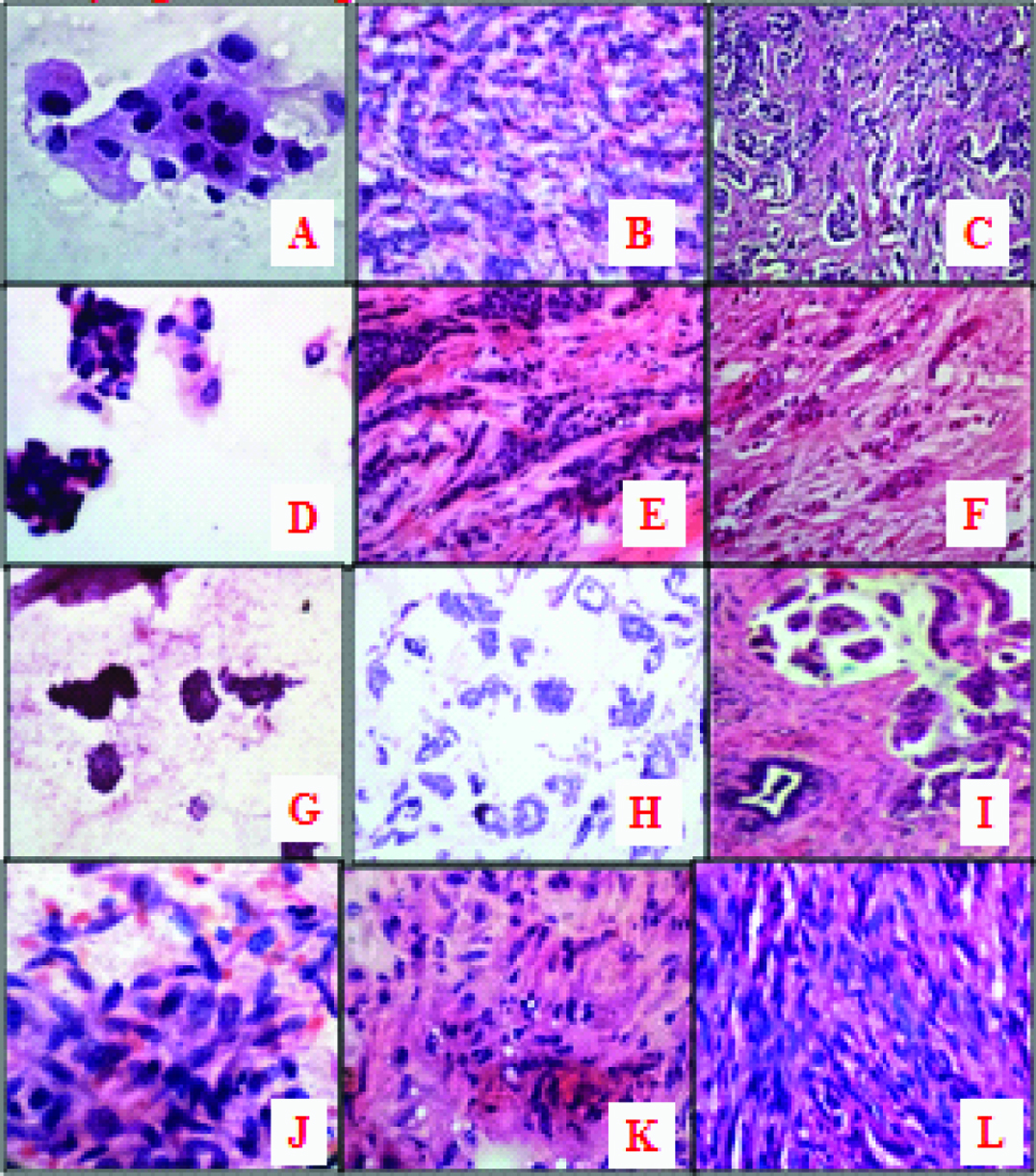
The microscopic features of various benign [Table/Fig-2a-l] and malignant [Table/Fig-3a-l] lesions on IC with FS were noted and later correlated with HP study.
Benign lesions: a) IC of Fibroadenosis (Negative for malignancy) (H&E, x400); 2b&c: FS and histopathology of Fibroadenosis (Benign lesion). b) FS (H&E, x200), c) HP (H&E, x200); d) IC of Granulomatous mastitis.(PAP, x200); e&f): FS and histopathology of Granulomatous mastitis with epithelioid granuloma (arrowhead), multinucleate giant cell (arrow). e) FS (H&E, x200), f)HP (H&E, x200); g): IC of Galactocele showing benign ductal epithelial cells, foam cells in a background of lipid miscelles.(H&E, x100); h&i) FS and histopathology of Galactocele. h) FS (H&E, x100), i) HP (H&E, x100); j) IC of benign phylloides tumour showing benign ductal epithelial cells and plump spindle cells (H&E, x200); k&l) FS and histopathology of benign phylloides tumour. k) FS (H&E, x40), l) HP (H&E, x100).
Malignant lesions: a) IC of infiltrating duct carcinoma (Positive for malignancy). (H&E x400); b&c) FS and histopathology of infiltrating duct carcinoma (malignant lesion), b) FS (H&E, x100), c) HP (H&E, x100); d) IC of infiltratting lobular carcinoma. (H&E, x400); e&f) FS and histopathology of infiltratting lobular carcinoma with Indian file pattern. e) FS (H&E x200), f) HP (H&E x100); g) IC of mucinous carcinoma showing atypical ductal epithelial cells in a mucinous background. (H&E,x100); h&i) FS and histopathology of mucinous carcinoma. h) FS (H&E, x100), i) HP (H&E, x 100); j) IC of malignant spindle cell tumour showing pleomorphic spindle cells and atypical mitotic figure. (H&E, x400); k&l) FS and histopathology of malignant spindle cell tumour. k) FS (H&E, x400), l) HP (H&E, x400).
IC findings of benign lesions [Table/Fig-2a] had overall low cell yield, except in fibroadenomas.
Imprint smears consisted of aggregates of cohesive, small, uniform cells with small rounded nuclei and bland chromatin with variable number of single, bare, bipolar nuclei scattered in the background, acute and chronic inflammatory cells especially in non neoplastic lesions. One granulomatous lesion was noted [Table/Fig-2d].
IC findings of malignant lesions [Table/Fig-3a] showed variable appearance with higher cell yield, irregular clusters of large discohesive cells with high N:C ratio, hyperchromatic, pleomorphic nuclei having irregular coarse chromatin and prominent nucleoli in the background of necrosis.
Distribution of lesions on FS [Table/Fig-1]: Out of 28(45.16%) cases of benign lesions, eight (12.9%) were non-neoplastic and 20 (32.26%) were benign neoplastic.
FS findings of benign lesions [Table/Fig-2b]: Benign looking epithelial cells arranged in acinar pattern with intervening stroma; inflammatory cells in stroma either neutrophils, lymphocytes, plasma cells or macrophages especially in non neoplastic lesions.
FS findings of malignant lesions [Table/Fig-3b]: Malignant tumour cells arranged in various patterns infiltrating the stroma. The main histologic feature of invasion was total disorganized arrangement of the neoplastic cells in the stroma.
The artifactual changes observed in FS were [Table/Fig-4a-e]: Compression artifacts, ice crystals ("bubbles") in stroma and nuclei. We also noted more condensed hyperchromatic nuclei and chatters even in HP study of the same frozen tissue.
a) FS showing compression artifact. (H&E, x400); b) FS showing ice bubbles in stroma (arrow) (H&E, x100); c) nuclear ice bubbles (arrow) (H&E, x200); d&e) Nuclear chromatin changes in FS and histopatholoy, d) FS (H&E, x400), e) HP (H&E, x400); f) FS of IDC with DCIS (arrow) showing disorganized arrangement of pleomorphic tumour cells in the stroma. (H&E, x40); g) Gross picture of benign adenomyoepithelial tumour (False positive case) showing intracystic solid mass with necrosis in the cyst; h&i) FS and Histopathology of of benign adenomyoepithelial tumour. h) FS (H&E, x400), i) (H&E, x200); j&k) IC and FS of lymph node metastasis. j) IC (PAP, x200). k) FS- (H&E, x40); l) FS of gynecomastia showing proliferating ducts without acini. FS- (H&E, x40).
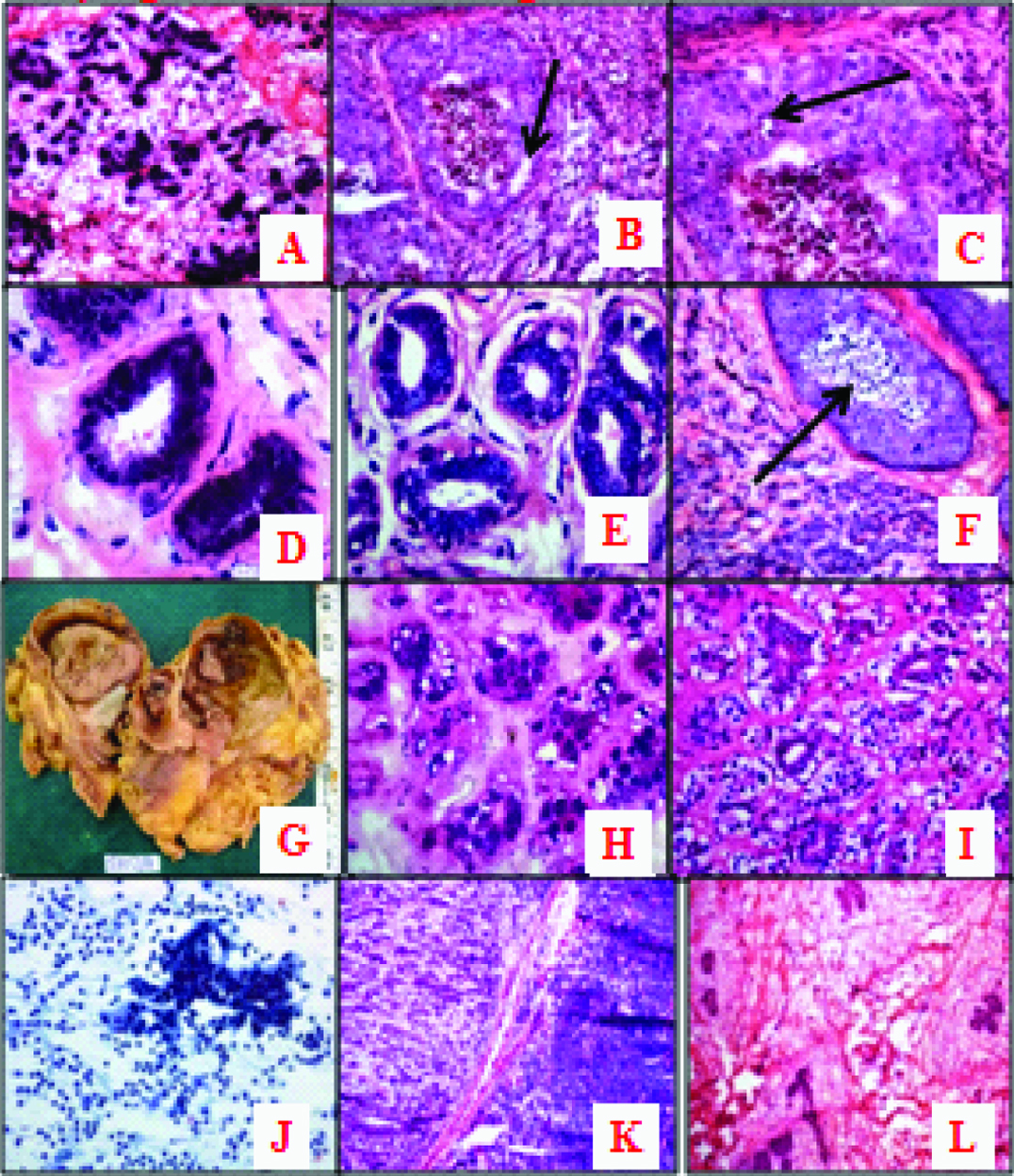
Associated Ductal Carcinomas In Situ (DCIS) were better appreciated in FS especially comedo pattern [Table/Fig-4f]. One case of false positivity on IC and FS was noted due to error in interpretation of gross, IC and FS features [Table/Fig-4g-i]. On HP study it was confirmed as benign adenomyoepithelioma.
Out of 33 malignant cases, 25 cases were evaluated by IC with FS for surgical resected margin involvement by malignancy and lymph node metastasis. One case showed a positive resected margin for malignancy, while remaining (24 cases) were negative. Among them, 20 cases were positive for lymph node metastasis [Table/Fig-4j-k] and rest (05) was negative, which were confirmed by HP study with an accuracy rate of 100%.
In male patients all three cases had gynaecomastia [Table/Fig-4l].
Distribution of various benign and malignant lesions on histopathology is given in [Table/Fig-5]: Fibroadenoma (42.86%) and infiltrating duct carcinoma (75.76%) were the commonest lesions in benign and malignant groups respectively.
Types of benign and malignant lesions on histopathology.
| Benign lesions on histopathology | No | % |
|---|
| Non-neoplastic lesions | Chronic abscess with foreign body granuloma | 1 | 12.5 |
| Lymphocytic mastitis | 1 | 12.5 |
| Granulomatous mastitis | 1 | 12.5 |
| Antibioma | 1 | 12.5 |
| Galactocele | 1 | 12.5 |
| Gynaecomastia | 3 | 37.5 |
| Total | 8 | 100 |
| NeoplasticBenign lesions | Fibroadenoma | 9 | 42.86 |
| Fibroadenomatoid hyperplasia | 5 | 23.81 |
| Fibrocystic disease | 3 | 14.21 |
| Adenomyoepithelial tumour | 1 | 4.76 |
| Proliferative breast disease without atypia | 1 | 4.76 |
| Fibroadenosis | 1 | 4.76 |
| Benign phylloides | 1 | 4.76 |
| Total | 21 | 100 |
| Total benign lesions on histopathology | 28 | 100 |
| Malignant lesions on histopathology | No | % |
| Infiltrating duct ca | 25 | 75.76 |
| Malignant phylloides | 2 | 6.06 |
| Medullary ca | 2 | 6.06 |
| Metaplastic ca/ angiosarcoma | 1 | 3.03 |
| Infiltrating lobular | 1 | 3.03 |
| Poorly differentiated ca | 1 | 3.03 |
| Mucinous/colloid ca | 1 | 3.03 |
| Total malignant lesions on histopathology | 33 | 100 |
Out of 62 cases studied, one (1.61%) inadequate case was excluded; hence, correlation was done for 61 cases of IC with the final HP study [Table/Fig-6]. In IC and FS one (2.94%) case was false positive which was due to error in interpretation and no false negative cases in this study [Table/Fig-7]. IC correlated 100% with final HP study in all malignant lesions and for benign lesions it showed 93.1% correlation. Sensitivity and specificity of IC was 100% and 96.43% respectively. The overall accuracy was 98.36% [Table/Fig-7]. On comparing the FS diagnosis of 62 cases with the final HP study, FS showed correlation of 100% for all malignant lesions and 96.6% for benign lesions. Sensitivity and specificity of FS was 100% and 96.55% respectively. The overall accuracy was 98.39% [Table/Fig-7]. p-value for IC and FS were <0.001 indicating significant correlation with HP study [Table/Fig-7].
Correlation of Imprint Cytology (IC) and Frozen Section (FS) with histopathology.
| Imprint cytology | Histopathology | Total |
|---|
| Benign | Malignant |
|---|
| Benign | 27(93.1%) | 0 | 27(43.5%) |
| Malignant | 1(3.4%) | 33(100%) | 34(54.8%) |
| Inadequate | 1(3.4%) | 0 | 1(1.6%) |
| Total | 29(100%) | 33(100%) | 62(100%) |
| Frozen section | Histopathology | Total |
| Benign | Malignant |
| Benign | 28(96.6%) | 0 | 28(45.2%) |
| Malignant | 1(3.4%) | 33(100%) | 34(54.8%) |
| Total | 29(100%) | 33(100%) | 62(100%) |
Statistical correlation of imprint cytology, frozen section with histopathology.
| Parameter | Imprint cytology | Frozen section |
|---|
| Number of inadequate material | 1 | 0 |
| Number of benign lesions | 27 | 28 |
| Number of malignant lesions | 34 | 34 |
| Total Number of evaluated cases | 61 (98.39%) | 62 (100%) |
| Total benign lesions on histopathology - 29 |
| Total malignant lesions on histopathology -33 |
| True positive‡ | 33(97.06%) | 33 (97.06%) |
| False positive ‡ | 1 (2.94%) | 1 (2.94%) |
| True negative ‡ | 27 (100%) | 28 (100%) |
| False negative‡ | 0 | 0 |
| Sensitivity § | 100% | 100% |
| Specificity § | 96.43% | 96.55% |
| Positive predictive value § | 97.06% | 97.06% |
| Negative predictive value § | 100% | 100% |
| Diagnostic accuracy § | 98.36% | 98.39% |
| p-value | <0.001 | <0.001 |
Tests of significance: Criteria
‡A true-positive result for malignancy indicated that IC, FS and histopathological analysis of the specimen was diagnostic of a malignant lesion.
‡A false-positive result for malignancy indicated that a diagnosis of malignancy was given on IC and FS, but the HP turned out to be benign.
‡A true negative result was considered when the diagnosis on IC, FS and HP was benign.
‡A false-negative result was considered when IC and FS showed no malignancy but the final diagnosis turned out to be malignant on HP.
§Sensitivity: probability that a test result will be positive when the disease is present (true positive rate, expressed as a percentage); §Specificity: probability that a test result will be negative when the disease is not present (true negative rate, expressed as a percentage); § Positive predictive value: probability that the disease is present when the test is positive (expressed as a percentage); §Negative predictive value: probability that the disease is not present when the test is negative (expressed as a percentage); § Diagnostic Accuracy is the sum of true positive and True negative divided by number of cases (expressed as a percentage).
Discussion
In the era of breast conservative therapy, breast tissue is most commonly sent for intra operative consultation [11]. The assessment of breast lesions has changed significantly with the advent of less radical surgical options and increased involvement of the patient in decision making, most breast biopsies are performed without an intent to proceed to immediate mastectomy if carcinoma is found [12]. Both FS and IC serve this purpose well and provide an accurate result in minutes while the patient is under anaesthesia. The interpretation of IC and FS allows a definite one stage surgical procedure possible leading to proper surgical plan and reduction in medical costs with inter departmental consultation [3]. Adhering to certain procedures for IC gives better results such as, tissue surface to be imprinted should be flat with no fat protruding from the edges and by blotting the cut surface by an absorbent material. Benign lesions requires more pressure during imprinting due to cohesiveness of epithelial cells and hence, cells in clusters. Malignant tissue imprints were more cellular than those of benign. Exceptions being carcinoma with dense fibrous stroma which yields less cells and fibroadenoma inspite of being benign is highly cellular [9,13]. Similar observations were noted in our study also.
One case of lymphocytic mastitis on IC showed inadequate smear with only few lymphocytes and no opinion was possible. This case was excluded for correlation of IC with HP study. On FS, extensive sclerosis and periductal inflammation consisiting of lymphocytes was noted and the diagnosis was given as strongly suggestive of lymphocytic mastitis which was confirmed on HP study. This was the only inadequate smear in this study which was due to non representative tissue taken or extensive sclerosis associated with the lesion. The diagnostic pitfalls in breast IC yielding to false positive diagnosis are pregnancy and lactation, papillary lesions, radial scar/complex sclerosing lesion, cellular fibroadenoma, epithelial hyperplasia with nuclear atypia, regenerative epithelial atypia and atypia of ductal epithelium in cysts [2,14,15].
The risk of making a false negative diagnosis on IC are tumours with central necrosis or sclerosis, complex proliferative lesions, low grade ductal carcinoma, lobular carcinoma, small cell carcinoma, high grade DCIS, mucinous lesions and small sclerotic fibroadenoma [2,8,14,15].
Technical skill and diagnostic expertise are essential for frozen diagnosis. Artifacts are unavoidable but they should be overcome. Pathologists should recognize these artifacts while analysing the FS as they obscure the definitive pathology. On FS artifactual changes observed are Ice Crystals ("bubbles") in fibrous stroma which is due to freezing of ice crystals giving appearance of bubbles and compression artifacts. But when the same tissue was processed for HP study, these "bubbles" of water disappeared due to redistribution into the stroma. At times very edematous tissues were difficult to cut without shattering due to the icy consistency. Nuclear ice crystals were due to damage by cautery or ischemia. The FS and HP paraffin block of the same tissue shows more condenced hyperchromatic nuclei, increased distortion by folds, tears, and chatter due to hardening of the tissue by freezing [3,16]. Similar findings were noted in our study also.
False positive diagnosis of breast lesions in FS: Benign lesions which were frequently over diagnosed as malignancy are microglandular adenosis, epithelial proliferations, sclerosing adenosis, radial scar, intra cystic papilloma, fat necrosis and juvenile papillomatosis. False positive conditions might also be attributed to false invasion [3,7,17–19]. Also seen in physiologic hyperplasia, reactive changes from chronic inflammation around a cyst or in the area of fat necrosis, treatment induced changes by radiotherapy and chemotherapy [20]. The total disordered arrangement of the malignant cells in association with a desmoplastic stromal reaction is the main histologic feature of invasion on FS [3].
False negative diagnosis of breast lesions in FS- The malignant lesions which are commonly under diagnosed as benign are tubular carcinoma, infiltrating lobular carcinoma, DCIS and lesions due to morphological changes after chemotherapy [3,7,8].
The incidence of false negativity on frozen tissues increases with diminishing size of the lesion due to artifactual distortion on freezing. Hence, the Association of Directors of Anatomic Surgical Pathology recommends that lesions less than 1 cm should not be frozen [7,21]. We also adopted the same criteria in our study. When faced with an unusual or rare form of invasive breast cancer, a standard diagnosis of invasive carcinoma can be used at the time of FS with the final diagnosis pending for HP paraffin section report [3].
The lesions that deferred the diagnosis to HP study are all epithelial proliferative lesions which includes usual ductal hyperplasia, atypical ductal and lobular hyperplasia, and ductal and lobular carcinoma in situ [3,7,17,19]. Others are intra ductal papillomas, lymphoproliferative lesions of the breast [3,7,19], soft tissue tumours and stromal or vascular lesion [22,23].
The conflicting situation between gross and microscopic examinations was radial scar, florid adenosis and those between microscopic and clinical findings were granulomatous mastitis, mammary duct ectasia and fat necrosis [18]. We noted one case of granulomatous mastitis on IC and FS [Table/Fig-2d-f] with well formed granulomas and giant cells and latter confirmed with final HP study. Acid Fast Bacilli (AFB) was negative in this case.
Diagnostic delay is directly related to excess fat or sclerotic tissue in samples and post chemotherapetic morphologic changes [18]. The definitive diagnosis should be deferred to HP study whenever the FS features are not specific. Under diagnosis of malignancy is apparently preferable to over diagnosis, which could prevent mutilating surgery [22].
The four main causes for committing errors in intra operative diagnosis of breast lesions are: inexperience (57%), microscopic sampling errors (24%), gross sampling errors (9.5%) and lack of inter departmental communication (9.5%) [3]. This should be overcome by knowing merits and demerits of these diagnostic methods.
One false positive case in this study was benign adenomyoepithelial tumour. It was wrongly diagnosed as malignant lesion on IC and FS. HP study showed tumour cells arranged in tubules lined by inner epithelial and outer myoepithelial cells with mild nuclear atypia. No mitosis was noted and finally diagnosed as benign adenomyoepithelial tumour. This false positive case was due to gross appearance of the tumour which showed intra cystic solid mass and necrosis [Table/Fig-4g-i]. On IC, this case was falsely misinterpreted for malignancy due to increased cellularity and mild atypia of cells. Cytological diagnosis of this entity is often difficult and which leads to risk of false positive reports [24]. On FS, artifactual changes due to freezing was misinterpreted as nuclear atypia and myoepithelial cells with clear cytoplasm for ice crystal bubbles. This case being rare and all the rare entities should be well known and considered in the differential diagnosis before giving the final report.
Finally, IC and FS correlated with final HP diagnosis in all malignant lesions giving 100% correlation and in benign lesions 93.1% correlation for IC while 96.6% correlation for FS. The accuracy rate was 98.36% for IC and 98.39% for FS. IC findings in our study were comparable with Tarek MN et al., and Francis IM et al., [18,24] while FS with Tarek M N et al., and Sultana N et al., [18,22]. Analysis of predictive values of both IC and FS revealed that Negative Predictive Value (NPV) is higher than Positive Predictive Value (PPV) denoting that these intra operative diagnostic methods are more reliable when negative than when it is positive for malignancy.
Limitation
A few cases with inadequate material were left out from the study which could have further enhanced the sample size.
Conclusion
IC is a simple, accurate, rapid and cost effective diagnostic tool, intra operatively wherein facilities for FS are not available. It preserves crisp cellular and nuclear detail. FS tissue architecture closely approximates permanent HP sections, but is frequently hampered by freezing artefact. But FS is able to differentiate carcinoma in situ and infiltrative lesions from benign breast lesions. When done together, IC and FS offer a more reliable diagnosis rather than when done individually. Hence, intra operatively, it is always useful to prepare both the slides. Knowledge of pitfall in IC and FS with documentation of clinical features, gross appearance, selection of appropriate tissue fragment helps in a more accurate intra operative diagnosis. HP study still remains the gold standard in final diagnosis of any breast lesion. The correlation of intra operative IC and FS diagnosis with the final HP diagnosis on permanent sections should form an integral part of quality assurance activities in the surgical pathology laboratory.
Tests of significance: Criteria
‡A true-positive result for malignancy indicated that IC, FS and histopathological analysis of the specimen was diagnostic of a malignant lesion.
‡A false-positive result for malignancy indicated that a diagnosis of malignancy was given on IC and FS, but the HP turned out to be benign.
‡A true negative result was considered when the diagnosis on IC, FS and HP was benign.
‡A false-negative result was considered when IC and FS showed no malignancy but the final diagnosis turned out to be malignant on HP.
§Sensitivity: probability that a test result will be positive when the disease is present (true positive rate, expressed as a percentage); §Specificity: probability that a test result will be negative when the disease is not present (true negative rate, expressed as a percentage); § Positive predictive value: probability that the disease is present when the test is positive (expressed as a percentage); §Negative predictive value: probability that the disease is not present when the test is negative (expressed as a percentage); § Diagnostic Accuracy is the sum of true positive and True negative divided by number of cases (expressed as a percentage).