Fissure-in-Ano is a linear ulcer in the squamous epithelium of the anus, distal to the dentate line. It is one of the most common and painful anorectal conditions encountered in surgical practice [1]. CAF is characterized by the presence of indurated edges, visible fibres of internal anal sphincter at the base of the fissure, and sentinel polyp or tag at the distal end of the fissure [Table/Fig-1] [2–4]. There is a dearth of epidemiological studies on anal fissures in India but the incidence of fissure is likely to increase due to factors like change in dietary habits with increased intake of low-fibre high-calorie foods.
There are several effective options for managing acute anal fissures non-operatively. These options vary from a change in dietary habits and fluid intake to local medication options like the cutaneous application of Isosorbide Dinitrate [5] or Diltiazem [6], or intra-sphincteric injection of botulinum toxin [7]. Most of these measures are effective not only for acute fissures but have a role to play in chronic fissures as well. There is however, a relatively higher recurrence rate and fissure persistence when compared to surgical management [5–7]. Surgical management is often offered only when a fair trial of medical management has failed.
Unfortunately, for many poorer patients needing definitive surgical treatment, the cost of treatment becomes manifold when we include the opportunity cost of income lost and expenses incurred during the hospital stay. Total cost incurred to the patient varies largely according to the choice of anaesthesia for the surgery. Patients undergoing surgery under spinal anaesthesia have to undergo a battery of blood tests and imaging as a pre-requisite for acceptance for anaesthesia, while we do not need any expensive investigations to do the same procedure under local anaesthesia. There is a marked difference in the final cost to the patient for the same surgery done under local and spinal anaesthesia.
Moreover, surgeons working in a rural setup are faced with several challenges and limitations, of which availability of anaesthetist is a great limitation and cannot be understated. Hence, it is more important to identify ways and means to do cost effective surgeries in the rural areas without compromising on the outcome, neither of the patient nor the condition being treated. The present study was conducted to compare the outcome of lateral anal sphincterotomy for chronic anal fissure, done under SA and LA.
Materials and Methods
This was a prospective randomized interventional study undertaken in Christian Fellowship Hospital, a secondary level health care setting in the semi-urban town of Oddanchatram in Dindigul district, Tamil Nadu, India. Most of the patients were agricultural labourers on daily wages and belonged to Upper-lower class IV Socio-Economic Class according to Modified Kuppusamy Scale [12].
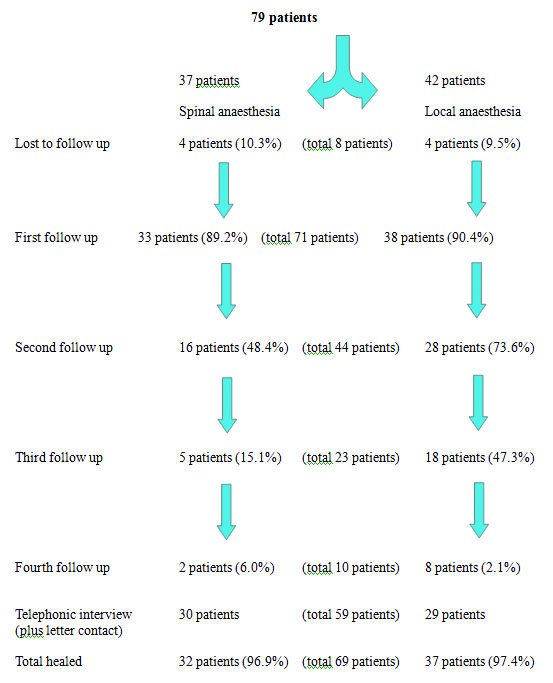
This study was conducted between a 12 month period (October 2009 and September 2010). A total of 79 eligible and willing adult patients with CAF were included in the study and were randomized to either SA group or LA group using a computer generated random numbers table.
For patients in spinal anaesthesia group, detailed blood work-up like haemoglobin, blood sugars, renal function tests and imaging were done before undergoing fitness for anaesthesia. These patients were admitted to the surgical ward prior to surgery and were kept nil orally from midnight on the day of surgery and intravenous fluids started just before shifting them to the operating room. Anaesthesia was administered by the anaesthetist and monitored till the end of the procedure. For patients in LA group, only haemoglobin and random blood sugars were done as they were not required to undergo detailed anaesthetic work-up. They were asked to report in the morning on the day of surgery and were not started on any intravenous fluids. LA was administered by the surgeon himself under aseptic precautions. A combination of 5ml of 2% lignocaine and 5ml of 0.5 % Bupivacaine were taken together, of which 5 ml was injected at the base of the fissure and 5ml injected at the site of sphincterotomy.
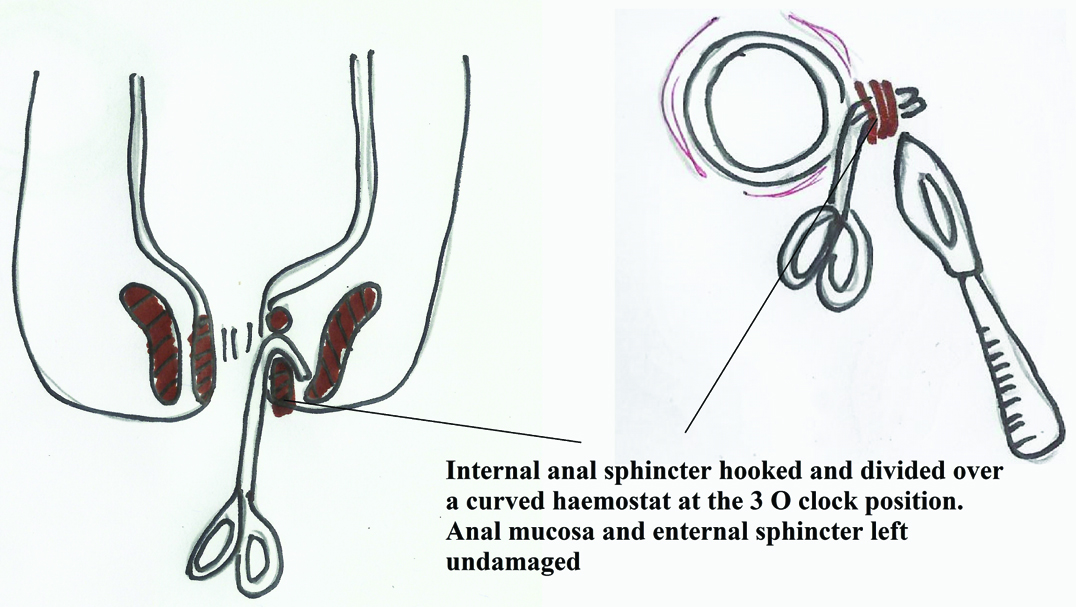
All the patients underwent standard open conservative internal anal sphincterotomy [Table/Fig-2] in lithotomy position irrespective of the group. The sphincter was divided upto the length of the anal fissure, under direct vision using a surgical blade or electrocautery. The adequacy of division was ensured by palpating the inverted ‘V’ shaped defect in the sphincter. The wound was dressed with simple vaseline gauze without suturing.
Schematic representation of the surgical technique in open las; step 1–hooking the internal anal sphincter muscle, and step 2 - division of the internal sphnicter.
Patients were asked to follow-up every week for a period of 4 weeks or till the fissure healed, whichever was earlier. Pain, infection and incontinence (minor and major) were measured during each follow-up visit. Fissure was declared healed when the patient had no pain or bleeding during defecation and clinically by the absence of sphincter spasm.
Pain was assessed using patients’ Verbal Descriptive Scale (VDS) for pain with standard five categories; 0: No pain, 1: Mild pain, 2: Moderate pain, 3: Severe pain, 4: Very severe pain.
Since, the rural populace is known to tolerate pain better and express less, VDS was considered more appropriate for this setting [13]. Persistent pain would mean inadequate sphincterotomy and would directly influence the healing of the chronic anal fissure.
Presence or absence of Infection was recorded during the follow- up visits as infection could increase the chances of incontinence or lead to further complications like abscess formation and bleeding.
Anal Incontinence was recorded using cleveland incontinence scale, severity of incontinence was categorized into minor and major incontinence, though an elaborate scoring scale was not used; Minor incontinence- incontinence to flatus alone, and Major incontinence- incontinence to fecal matter.
The final outcome of the study was the healing rate of Anal fissure. As it can take upto 4-8 weeks for the fissure to heal completely, patients were followed-up weekly for the first 4 weeks. Patients who were symptomatic at the end of 4 weeks were followed-up by phone interviews at the end of 8 weeks. The outcome of the fissure was grouped as healed, or persistent fissure. Patients with persistent pain and bleeding during defecation, or presence of ulcer even after 8 weeks were declared as persistent fissure and evaluated for other causes for the fissure.
Telephonic interviews were conducted for those who failed to attend the follow-up clinic, at 4 weeks and 8 weeks. On the telephone interviews, patients were enquired regarding their symptoms of pain, bleeding, infection and incontinence. Patients who reported to be completely asymptomatic on the telephonic interviews were declared fissure healed and included in the final outcome as such. Patients with any persistent symptoms were requested to review in the follow-up clinic for further evaluation of the fissure. For those with no phone numbers, postcards were sent requesting them to review in the follow-up clinic for evaluation of fissure healing.
Statistical Analysis
The data was analysed using statistical softwares SPSS 15.0, Stata 10.1 and MedCalc 9.0.1. A total of 79 patients participated in the study with 55 (69.6%) women and 24 (30.4%) men. A total of 42 patients (53%) underwent LAS under local anaesthesia and 37 patients (47%) underwent LAS under spinal anaesthesia.
Results
During the intra-operative period, 4 patients (9.5%) in the local anaesthesia group complained of severe pain during the procedure. The pain was mostly while injecting the local anaesthetic which reduced as the local anaesthetic took effect, following which they tolerated the procedure well. They were further managed with local anaesthetic upto the maximum allowable dose. No pain or anaesthesia related complications were reported in the spinal group. However, this increased incidence of intra-operative severe pain in the local group was not statistically significant (p=0.054) when compared to the spinal group.
In the immediate post-operative period, 3 patients (7.1%) in the local group complained of severe pain while none in the spinal group had any complaints. Also the difference was not statistically significant between the two groups (p=0.097). Though pain eventually subsided with oral analgesics, one of the three patients had to be admitted for pain relief.
Of the 79 patients, only 71 (89.9%) reported for the first follow-up visit, one week after surgery. Remaining 8 patients (10.1%) failed to follow-up even once and was not contactable by phone or letters. These patients were considered lost to follow-up and were excluded from the analysis.
Two patients, one from each group, presented with severe pain and sphincter spasm in the first week. They were reviewed by senior consultants and found to be due to inadequate surgical procedure. As they occurred within the first week, they were considered as surgery failures and included as such in the final analysis. Repeat surgery was done for these two patients immediately and both recovered well.
During the second follow-up visit (two weeks after surgery), only 44 patients (61.9%) reviewed, 28 (66.7%) belonged to local group and 16 (43.2%) belonged to spinal group. There was further decrease in patient numbers during subsequent follow-up visits. All ten patients who reported at the end of 4 weeks were pain-free and their fissures healed completely. Summary of patient numbers during follow-up visits is presented in [Table/Fig-3].
Summary of patients in both groups and during follow-up visits.
All the 71 patients were followed-up till 8 weeks. While 10 (2 and 8) patients came for follow-up, rest 59 patients were contacted by phone (51) and letters (8) at the end of 4 weeks and 8 weeks. Of those contacted by telephone at 4 weeks, forty five patients (63.4%) were completely asymptomatic without any complications, and were declared fissure healed. Remaining six patients (8.5%) complained of some pain and occasional bleeding during defecation at the end of 4 weeks. These six patients were contacted by phone again at the end of 8 weeks and were found to be asymptomatic, eligible to be considered fissure healed. All eight patients who were contacted by letters reviewed within a week. All of them were pain free and their fissures healed completely.
Pain: Two patients, one from each group, were declared as surgery failure and repeat surgery was done immediately. Both the patients were included back in the study after the repeat surgery and followed-up like other patients till the fissure healed. Hence, both these patients were included in the final analysis. Of the 71 patients reviewed in the first visit, one patient in spinal group presented with severe pain while others presented with mild or moderate pain. The association between pain and anaesthesia was analyzed using Fisher-exact test, and there was no statistically significant difference in pain between the two groups (p=0.482). Findings of the same are summarized in [Table/Fig-4].
Pain during first follow-up visit (N=71).
| Pain | Local anaesthesia | Spinal anaesthesia | Total |
|---|
| No Pain | 19(51.3%) | 21(65.6%) | 42(59.2%) |
| Mild Pain | 16(43.2%) | 9(28.1%) | 25(35.2%) |
| Moderate Pain | 2(5.4%) | 1(3.1%) | 3(4.2%) |
| Severe Pain | 0(0%) | 1(3.1%) | 1(1.4%) |
| Very Severe Pain | 0(0%) | 0(0%) | 0(0%) |
| Total | 37(100%) | 32(100%) | 69(100%) |
p=0.482, Not significant, Fisher-Exact test. [Two patients (one from each group) were excluded in the first follow up as they were considered as surgical failure]
Similarly, there was no statistically significant difference (p=0.834) in pain during the second follow-up visit as shown in [Table/Fig-5].
Summary of pain during second follow-up visit.
| Pain | Local anaesthesia | Spinal anaesthesia | Total |
|---|
| No Pain | 19(67.9%) | 10(62.5%) | 29(65.9%) |
| Mild Pain | 8(28.6%) | 6(37.5%) | 14(31.8%) |
| Moderate Pain | 1(3.6%) | 0(0%) | 1(2.3%) |
| Severe Pain | 0(0%) | 0(0%) | 0(0%) |
| Very Severe Pain | 0(0%) | 0(0%) | 0(0%) |
| Total | 28(100%) | 16(100%) | 44(100%) |
p=0.834, Not significant, Fisher-Exact test
Infection: Two patients had wound infection in the spinal group during the first follow- up visit, while two patients in the local group and one patient in the spinal group presented with infection during the second visit. However, there was no statistically significant difference (Fisher-Exact test) between the two groups during both the visits (p=0.171 and p=1.000 respectively) as shown in [Table/Fig-6]. All settled without any need for surgical intervention.
Summary of infection during first and second follow- up visits.
| Infection | Local anaesthesia | Spinal anaesthesia |
|---|
| First Visit | Second Visit | First Visit | Second Visit |
|---|
| Present | 0(0%) | 2(7.1%) | 2(6.3%) | 1(6.3%) |
| No infection | 39(100%) | 26(92.9%) | 30(93.8%) | 15(93.8%) |
| Total | 39(100%) | 28(100%) | 32(100%) | 16(100%) |
| p-value | 0.171 | 1.000 |
Incontinence: Incontinence was measured based on patient symptoms, in the form or minor and major anal incontinence. Only three patients (4.2%) in the study reported incontinence during the first follow-up visit and all three had minor incontinence i.e. incontinence to flatus only. None of the patients reported incontinence during subsequent visits. Using Fisher-exact test, there was no statistically significant difference between the groups (with a p-value of 1.00) as presented in [Table/Fig-7].
Incontinence between local anaesthesia (LA) and spinal anaesthesia (SA) in follow-up visit I. (N=71).
| Incontinence first follow up visit | Local anaesthesia | Spinal anaesthesia | Total |
|---|
| Present | 2(5.1%) | 1(3.1%) | 3(4.2%) |
| Absent | 37(94.9%) | 31(96.9%) | 68(95.8%) |
| Total | 39(100%) | 32(100%) | 71(100%) |
p=1.000, Not significant, Fisher-Exact test
Fissure Healing: Of the total 71 patients included in the analysis, fissure healed in 69 patients (97.2%) within the planned study period of 4 to 8 weeks. Fissure healed completely in 63 patients (88.7%) within 4 weeks. It healed by 8 weeks in another 6 patients (8.5%). Comparing the fissure healing rates between the local and spinal anaesthesia groups, there was no statistically significant difference in fissure healing rates (p=1.000, Not significant, Fisher-Exact test).
Discussion
Even with the advent of several non-operative therapies for chronic anal fissure, Lateral anal sphincterotomy is still considered the standard surgical treatment that provides the best healing rates and least recurrence. From preference to general anaesthesia in the earlier years, trends have gradually shifted towards LA [11,14,15]. A few distinct advantages were noted in the study while doing LAS under LA. First, adequate analgesia for the procedure was satisfactorily achieved in most of the patients. By injecting some lignocaine at the base of the fissure, there was good relief of pain over the fissure. This also allowed painless per rectal examination of the internal sphincter. This was followed by injecting lignocaine at the surgery site which provided good analgesia for sphincterotomy. However, 4 patients in the local group reported severe pain during the procedure though it was not statistically significant. As the surgeries were done by several consultants and registrars, this may be attributed to minor differences in surgical technique.
Second, internal sphincter is not relaxed under LA. As the sphincter is in spasm, the length of the sphincter could be appreciated easily and the adequacy of the length of division verified distinctly. This benefit is lacking under spinal or general anaesthesia where the sphincter is fully relaxed, presenting difficulties in defining its length. Since, we performed conservative or limited sphincterotomy in the study, defining the length of the sphincter carried major importance. Longer division of sphincter would lead to a higher rate of incontinence while shorter division may not relieve the spasm or heal the fissure [16]. The low rates of incontinence reported in the study (4.2%) supports other studies’ findings [17,18] of low rates of incontinence with limited sphincterotomy. Third is the difference in the cost of Surgery done under LA and SA. Considering the cost of pre-operative evaluation, surgery cost and opportunity cost, spinal group patients spent atleast three times more money than the local group patients for the same surgery. This carries greater significance in this setting where most of the patients come from poor economic backgrounds. In view of these benefits with LA, Hiltunen and Matikainen called it ambulatory treatment for CAF where patients were allowed to leave the clinic immediately after the surgery [19].
With shortage of trained anaesthetists in surgical centres in rural hospitals, in spite of awareness of the potential complications of SA, often surgeons themselves have to give the SA, while trained nurses monitor the vitals throughout the procedure. In such contexts, LA administered by the surgeon himself is definitely safer in avoiding the risks of SA. Obese patients or those with unfavourable buttocks or those needing exploration can be reserved for SA or general anaesthesia to achieve good relaxation and exposure. In our study however, we were able to perform sphincterotomy inspite of all patients randomized to this group. We did not have to resort to regional or general anaesthesia due to an obese body habitus.
Following surgery all patients in the study got back to their routine work within the first week. Symptoms subsided completely in most of the patients by the end of one week. Due to irregularity in follow up, telephonic interviews were resorted to at 4 and 8 weeks. Many patients in the study, coming from low socio-economic background, failed to report regularly for follow-up visits as this meant a loss of one day’s wages apart from the expenses incurred in travelling and food. Mousavi et al., in a similar study have used telephonic interviews to enquire about the fissure status in addition to the frequent visits on pre-determined basis [20]. On the other hand, Fallaize reports higher patient satisfaction with telephonic follow-up for patients following anorectal surgery [21].
Though weekly follow-up helped in assessing the progress of fissure healing, it did not influence the final outcome. As persistence of fissure is almost always associated with symptoms of pain and bleeding during defecation, phone interviews at 4 weeks provided a fairly reasonable assessment whether the fissure is healed or persistent. As some fissures take up to 8 weeks to heal completely, a repeat phone interview at the end of this period provided adequate information regarding the status of the fissure. Almost all patients could be contacted by phone, and those who did not have phone numbers responded to post cards requests to review.
Most of the studies have showed greater than 95% fissure healing rates following LAS [6,22]. The two surgery failures in the study are probably due to improper surgical technique. As a surgical training institute there is a small chance of technical inadequacy in surgeries being done by registrars under supervision. Following repeat surgery these two patients were followed-up till fissure healed, though they were removed from analysis. The fissure healing rates would only be higher if these patients were included.
Fecal incontinence is the most feared complication following LAS, as mentioned in several studies. In this study, we had a total incontinence rate of 4.2%, which is much lower as compared to other studies [17,18,22]. Even with the widely varying incontinence rates reported in other studies, this study rate is significantly lower. Limited or conservative sphincterotomy used in the study could partly explain this low rate as studied by several others [16,23].
Limitation
Being a training institution, procedure was performed by the surgery residents as well as consultants. This could explain the reason for failed surgeries. Telephonic interviews used in the study cannot replace regular patient follow-up. However, it can be used as surrogate indicator in such situations where patients may feel uncomfortable to review especially when they are asymptomatic.
Conclusion
Lateral anal sphincterotomy provides very good healing of CAF. Choice of anaesthesia for the procedure is at the discretion of the surgeon and depends on the availability of anaesthetist.
LA provides adequate pain relief for the procedure apart from the advantage of easy palpability of the sphincter. It can be done as an Outpatient procedure without the need for an anaesthetist, and carries a significant cost benefit to the patient especially in lower socio-economic settings.
There is no significant difference in the complications or the healing of the fissure when compared with SA.
All the incontinences reported were minor which did not require any treatment. Overall fissure healing rate was very high and there was no recurrence of fissure in the period of study.
p=0.482, Not significant, Fisher-Exact test. [Two patients (one from each group) were excluded in the first follow up as they were considered as surgical failure]
p=0.834, Not significant, Fisher-Exact test
p=1.000, Not significant, Fisher-Exact test