Nasal tip surgery is among the most complex and difficult tasks in modern rhinoplasty [1]. The suture-techniques almost always offer a reliable and dramatic method of tip reshaping without a need to break or interrupt the alar rim strip or even adding tip graft. Moreover, these sutures have proven effective in managing many secondary tip deformities whenever the alar cartilage remnants permit. The accuracy and quality of tip surgery depends on the thoroughness of assessment before modification. One of the major advantages of open rhinophasty is that the alar cartilages can be examined in their normal, resting state to identify intrinsic characteristics of each alar cartilage and the intricate relationship between the two [2].
In 1969 Anderson proposed the “tripod concept” for the tip for the first time. In this technique the right and left lateral crura comprised the two legs of the tripod, and the two conjunct joined medial crura which functioned as the third leg. The medial crura function was supported by the attachments to the superior and inferior septum. The final result was a tip that was positioned in a more superior and anterior location [3]. Later in 1989, Tebbets published and popularized the “systematic non-destructive approach” to nasal tip suturing, in which he described a four-staged approach to tip surgery. Tebbets also introduced the tip rotation suture passing from cephalic portion of the medial crura to the dorsal septum near the septal angle to maintain tip rotation [4]. In 1997 Gruber and in 1998 Guyuron, added some other suture techniques for the tip supporting the existing tip sutures [5]. In all the above mentioned techniques, postoperative change and tip rotation occur sometimes.
This study was aimed at describing a new simple suture that allows securing nasal tip definition through a tripod suture in a manner that will prevent postoperative change. This technique allows the surgeon to maintain optimal control of tip rotation and definition, which can satisfy patient’s expectations with long-lasting durable results.
Materials and Methods
In this prospective study, sixty-two consecutive women with nasal tip drooping and some degree of columellar retraction attending the Department of Plastic and Reconstructive Surgery of 15th Khordad Hospital, were included. All the 62 patients underwent this technique from January 2005 to September 2009. Their age ranged from 17 to 32 years. Most of these patients came to our clinic requesting rhinoplasty in order to improve the aesthetic aspect of their nose especially the tip.
Fifty-one primary and 11 secondary open rhinoplasties were performed using the conventional techniques in patients with minimal columellar show or columellar retraction and tip drooping in need of tip rotation. The new suture technique was used before closing the incisions on each patient. Based on each case, considering patient’s expectations and surgeon’s preferences, the standard technique was performed in order to obtain primary tip definition and rotation.
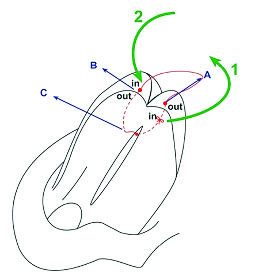
Afterwards, in the final stage of each operation 3 points were marked on the tip and caudal septum with bleu de methylene [Table/Fig-1]. These 3 points included: points A and B on the cephalic edge of the dome on each side with 2 mm distance from the cephalic margin of the medial crura. The third point (i.e., point C) was on the anterior part of the caudal septum [Table/Fig-2]. Here it should be mentioned that before placing sutures, it was necessary to sculpt the anterior septal angle to the desired shape. The suture was bilaterally placed between the medial third portion of the lateral crura (dome area) just posterior to the junction of the intermediate and lateral crura along their cephalic borders and anterior caudal septal angle.
Technique schematic view. A- right new dome of lower cartilage. B- left new dome of lower cartilage. C- nasal cartilaginous septum.
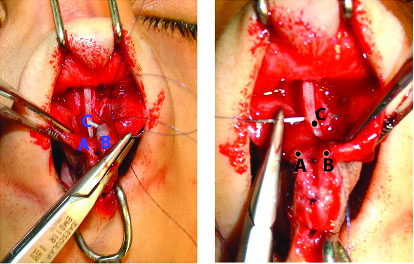
Intraoperative view of this technique. A- right new dome of lower cartilage. B- left new dome of lower cartilage. C- nasal cartilaginous septum.
A non-absorbable suture (Prolene or Nylene5-0) was inserted through point A from the cephalic side of one dome to point B on the cephalic side of another dome and finally through point C on the anterior part of caudal septum. In other words, Prolene or Nylene 5-0 was used in a loop manner suture from the cephalic side of each dome to the anterior part of caudal septum [Table/Fig-1]. Intraoperatively, the exact effect of this suture can be determined by observing the domes movement as the suture is tightened. The knot is placed in buried interrupted fashion. The suture is tightened incrementally, which enables the surgeon to set the inter-domal and dome septal angle distance or reduce it if necessary.
Since this suture is placed in the cephalic part of the dome and anterior of caudal septum retraction of the columella is not observed and its effect on the inter-domal distance is less. In order to prevent the widening and flattening of the lower lateral cartilage, only the interdomal suture and columellar strut were used in all patients in the usual manner. In the patient with mild or border-lined projection, the suture was used with caution in order to save the tip-to-septal distance.
This suture completed Daniel’s suture and in it, all the required techniques for reforming cartilages and tip were used. Care was taken to pass the suture along equal points on each dome to enable proper alignment with the transverse and vertical tip plane. Caution is necessary so the suture is not secured too tight, which would result in excess crura flare and overly supra tip depression. Consequently, this suture was used in the final part of operation for better establishment of the domes and for providing a favorite tip definition. The above-mentioned suture was used in patient tip rotation with increased columellar retraction for achieving ideal tip definition and it corrects tip projection by tip rotation.
Results
The patients were followed-up from 22 to 72 months (mean = 52.3). The projection and rotation was satisfactory in most patients and the final results persisted with only minimal changes over time. One patient encountered depression in the supra tip after 3 weeks, hence suture was removed and the patients breathing was revived. Three patients encountered widening in the tip area, which was corrected during revision by replacing the inter-dome. In four other patients revision was done for other reasons such as osteotomy asymmetry, dorsum depression, and hump remain. In some patients the outcomes were adverse and repeat surgery was required [Table/Fig-3,4].
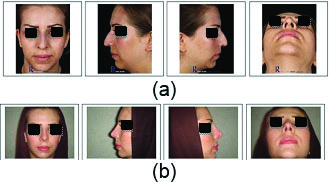
A patient’s before (A) and after (B) nasal tip projection and supra tip break formation by using this technique.
The postoperative frontal view shows a narrower nasal tip and shorter nose with more upper lip visible.
The postoperative left and right lateral view shows a shorter nose, removal of her dorsal hump and increased nasal tip rotation and longer upper lip.
The postoperative base view shows a narrower nasal tip that is more triangular in shape.
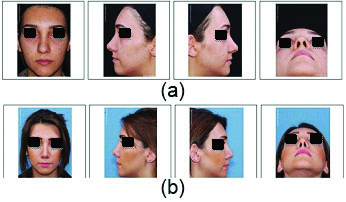
Frontal, left lateral, right lateral and base view of a patient’s before (A) and after (B) nasal tip projection and supra tip break formation by using this technique.
The postoperative frontal view shows a narrower nasal tip and shorter nose with more upper lip visible.
The postoperative left and right lateral view shows a shorter nose and increased nasal tip rotation and longer upper lip.
The postoperative base view shows a narrower nasal tip that is more triangular in shape.
Nevertheless, this new suture maintains the favorite tip definition with slight dorsal tip inclination. Indeed, it causes a two-point definition as the columellar lobular angle and supra tip break definition. In addition, long-term follow up shows that this new suture (i.e., cephalic dome septal rotation suture) is able to maintain optimal position of supra tip break and definition. All patients were followed up six months post-surgery. However, in the one-year follow-up 17 out of 62 patients did not refer to our center for evaluation, although they stated they were satisfied with the results on phone conversations [Table/Fig-5].
Patients’ follow-up data after Conventional rhinoplasty with this new suture technique.
| Primary/Secondary correctivenasal surgery | follow-up(mean = 52.3 months) |
|---|
| Conventional rhinoplasty with this new suture | conventional Primary rhinoplasty with this new suture (n=51 patients) | supra tip depression (n=1) |
| widening in the tip area (n=3) |
| conventional Secondary rhinoplasty with this new suture (n=11 patients) | revision required for other reasons (osteotomy asymmetry, dorsum depression, and hump remain) (n=4) |
| patients lost to follow-up (n=17) |
This new suture is presented as a new complementary technique in rhinoplasty for nasal tip rotation and defining supra-tip and infra-tip. The results are shown to be long lasting and optimal. In brief, the advantages of this new suture technique are as follow:
The negative effects can be controlled and are reversible intraoperatively;
There is no harmful effect on the wound healing;
It does not disrupt the structural integrity of the tip elements;
It improves the surgeon’s control on the amount of tip definition and rotation;
It provides good results on supra tip break point (bird beak appearance);
It increases columellar lobular angle;
It does not decrease columellar show.
Discussion
The goal in each rhinoplasty is a good tip projection and definition, an adequate rotation as well as a good configuration of the tip. The dome is considered the highest arching segment within the nasal vestibule, which is why we have focused on dome.
Projection of the tip refers to the posterior-anterior distance, in which the tip extends from the alar-facial groove. Several methods of calculating tip projection have been developed. The simplest method, as described by Simons [6], defines projection as the distance from the sub-nasal to the tip defining point as seen on the profile view. If the base view demonstrates a columellar-to-lobule ratio of approximately 2:1, the intent of these reports is the planned and unintended dynamic changes that occur when the sutures are used to reshape the tip [7,8].
Ideally the difference in the height of the dome vs. the anterior septal angle is about 6 to 7 mm. Here we emphasize that the goal of this new suture is a better tip rotation for tip definition. Moreover, in cases with drooping tip, this rotation leads to a better tip projection and can stabilize tip rotation. In order to get a better tip projection and definition, the domes need to be fixed in the anterior part of the caudal septum. Surgeons can apply our technique to change the tension of suture for a better tip definition, as she/he desires.
Several techniques are available for the rhinoplastic surgeon to modify the tip. These techniques include suture, scoring or crushing, resection, and grafts to the tip [9]. Since most of the supporting structures of the tip are interrupted during rhinoplasty, increasing tip definition during surgery is necessary [10].
The effects of sutures depend largely on the magnitude of suture tightening, the intrinsic factor of the cartilage thickness, and the degree of soft tissue undermining. The tip complex is perhaps the most intricate of the nasal structures, exhibiting subtle but evident responses to manipulations of the lower lateral cartilages. Cephalic dome-septal rotation suture can cause supra-tip break. This dynamic effect was obtained by altering the relationship between projection of the defining tip points and the dorsum and by lowering the dorsal septum and augmenting tip projection with a columellar strut. Domes were equalized above the anterior caudal septum with creating supra tip and tip support.
It is important to note that this new suture is different from the ‘tip rotation suture’, which was described by Anderson and Tebbets [3,4]. Nasal tip rotation suture was passed through the medial crura and then tied up to the anterio-caudal septum. The overprojected nasal tip also widened and retracted. Tip rotation suture consists of a loop that passes caudal to or through the medial genu, in effect harnessing the lower lateral cartilages. Then it anchors to the anterio-caudal septum. If a medial suture is not used before the placement of this suture, it may result in columellar flattening [11].
Conclusion
It is important to say that this new suture is different from ‘tip rotation suture’ that was described by Tebbets. Our suture maintains the favorite tip definition with slight dorsal tip inclination. Indeed, it causes a two-point definition as the columellar lobular angle and the supra tip break definition. In addition, long-term follow-up has shown that this new suture (i.e., cephalic dome-septal rotation suture) is able to maintain optimal position of the nasal tip projection and definition. Actually, in this technique we could form the supra tip break in more controlled manner during operation which is slightly different from previous techniques as mentioned in this study and the tip defining points is created better accompanying with more attractive supra tip break. Also, the durability of the final shape of nose obviously increased by our method.
Conflict of Interest: The authors declare that there has been no conflict of interest upon this article whatsoever.