Ameloblastoma is one of the most recognized odontogenic tumour in many countries from all over the world. It is a relatively rare neoplasm derived from odontogenic epithelium and represents about 1% of all oral tumours [1]. Ameloblastoma may arise from developing enamel organ, epithelial cell rest of dental lamina, epithelial lining of odontogenic cysts and basal cells of oral epithelium [2]. It is a benign tumour but has aggressive characteristics such as persistent growth and locally invasive to surrounding structures [3]. Ameloblastomas usually present as a painless swelling, slow growing mass, expansion of jaw bones, perforation of mandible or maxilla cortical plates and infiltration to surrounding soft tissue or sinonasal structure [4]. According to the 2005 classification of tumours of the World Health Organization, there are four different categories of ameloblastoma: the conventional solid/multicystic ameloblastoma, the peripheral ameloblastoma, the desmoplastic ameloblastoma, and the unicystic ameloblastoma [5]. Extraosseous ameloblastoma known as peripheral ameloblastomas are very rare and constitute 1-5% of all ameloblastomas [6]. Radiographically, ameloblastomas may present as unilocular or multilocular radiolucent lesions [7,8], located primarily in the posterior mandibular region [1,9–12].
Several histopathological subtypes of ameloblastoma are follicular, plexiform, acanthomatous, desmoplastic, granular cell, and basal cell pattern. All of these histopathological subtypes can be found as individual or as a combination of two or more types or can be found as a hybrid lesion with any other odontogenic tumours. Surgical removal is still the best option for patient with ameloblastoma and range from conservative surgical therapy to radical surgery [13]. The recurrence rate is found related to the type of surgery and extents from 15-25% after radical surgery to 75-90% after conservative surgery [14]. Prevalence of ameloblastoma is high in Asian [15,16] and African [17,18] populations, but it is a minority in North America [19,20] and European countries [21].
Even though the prevalence of ameloblastomas has been established worldwide, demographic profile and histopathological data of ameloblastoma in different populations is not adequate [2]. In Southeast Asian alone, collective data of ameloblastoma has not been well analyzed or compared separately from other odontogenic tumours. The study of the tumour in these regions especially in Myanmar and Northern Thailand are still limited. Thus, the aim of this study was to analyze and compare the prevalence and demographic data of clinical features of ameloblastoma and its histopathological variants in Southeast Myanmar and lower Northern Thailand populations diagnosed over a period of more than 13 years.
Materials and Methods
A retrospective study on ameloblastoma was performed based on the availability of oral biopsy specimens retrieved from Surgical Oral Pathology Laboratory Archive, Division of Oral Pathology, Department of Oral Diagnosis, Faculty of Dentistry, Naresuan University, Phitsanulok, Thailand, between January 2002 and August 2015. Total 616 cases were obtained from the entire archive, and 30 cases were diagnosed as ameloblastoma. All ameloblastoma specimens were sent in by clinicians in lower Northern Thailand and the hospital located along the border of Southeast Myanmar and Thailand region.
The age, gender, nationality, anatomical location and clinical appearances of all cases were compiled from the clinical data sent with the biopsy records. Histopathology slides stained with hematoxylin and eosin were reviewed and classified by an experienced oral pathologist based on World Health Organization classification [5]. Clinical records of one case that was sent with the biopsy material were with inadequate information and was excluded. Data with regard to age, gender, nationality, clinical manifestation, radiographic appearances, anatomical distribution and histological subtypes were analyzed. Site distribution in both jaws was divided into anterior (from midline to distal surface of canine) and posterior (from mesial surface of first premolar to ramus in the mandible and to tuberosity in the maxilla) parts. Lesions that involved entire left or right side of mandible and maxilla or entire mandible or maxilla as well as coronoid or condylar process were classified in separate category of anatomical distribution. The collected data were subjected to descriptive statistical analyses with the SPSS version 17.0 statistical software package (SPSS Inc., Chicago, USA). Pearson’s χ2 test and t-test were employed. The critical level of significance was set at p<0.05. This work was approved by the ethics committee of Naresuan University (535/59).
Results
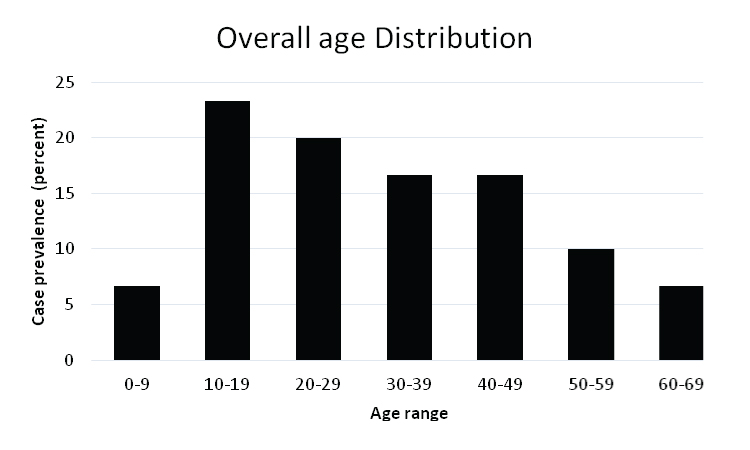
Total of 616 reported cases from over 13 years archive were reviewed, 30 cases (5%) were diagnosed as ameloblastoma. One case with inadequate clinical information was excluded. The remaining patient group comprised 14 females and 16 males, for a M:F ratio of 1.14:1. The mean age (±standard deviation) of the patients was 31.3±15.6 (range, 9 to 63) years. The mean age for each gender was 34.3±16.4 years for males and 27.9±14.4 years for females. Ameloblastoma was found most commonly in the age range of 10-49 year. The peak prevalence was in the 10 to 19-year age group (23.3%) and it gradually fell off with increasing age [Table/Fig-1]. Total 22 patients were Thai and eight were Burmese. Peak prevalence for Thais was in 10 to 19-year age group (27.3%) and for Burmese was in 30 to 49-year age group (33.3%). The mean age observed were 28.8±15.1 years for Thai and 38.3±15.5 years for Burmese respectively [Table/Fig-2].
Distribution of ameloblastoma according to age groups.
Summary of data of all ameloblastoma cases from 2002-2015.
| Thai | Burmese | Total |
|---|
| Total number of case (n=30, 100%) | 22(73.3%) | 8(26.7%) | 30(100%) |
| Mean age (year)±S.D. | 28.8±15.1 | 38.3±15.5 | 31.3±15.6 |
| Gender |
| Male | 13(59.1%) | 3(37.5%) | 16(53.3%) |
| Female | 9(40.9%) | 5(62.5%) | 14(46.7%) |
| Clinical features |
| Painless swelling | 19(86.4%) | 8(100.0%) | 27(90%) |
| No swelling | 3(13.6%) | 0(0.0%) | 3(10%) |
| Anatomic location |
| Maxilla |
| Anterior | 1(4.5%) | 0(0.0%) | 1(3.3%) |
| Posterior | 2(9.1%) | 0(0.0%) | (6.7%) |
| Entire left or right side | 1(4.5%) | 0(0.0%) | 1(3.3%) |
| Mandible |
| Anterior | 0(0.00%) | 0(0.0%) | 0(0.0%) |
| Posterior | 16(72.8%) | 3(37.5%) | 19(63.3%) |
| Entire left or right side | 0(0.0%) | 2(25.0%) | 2(6.7%) |
| Whole Maxilla | 0(0.0%) | 0(0.0%) | 0(0.0%) |
| Whole Mandible | 2(9.1%) | 3(37.5%) | 5(16.7%) |
| Radiographic appearances |
| Unilocular radiolucency | 8(36.4%) | 1(12.5%) | 9(30%) |
| Multilocular radiolucency | 14(63.6%) | 7(87.5%) | 21(70.0%) |
| Ameloblastoma subtypes |
| Solid/multicystic |
| Follicular | 3(13.6%) | 2(25.0%) | 5(16.7%) |
| Plexiform | 11(50.0%) | 1(12.5%) | 12(40.0%) |
| Acanthomatous | 2(9.2%) | 1(12.5%) | 3(10.0%) |
| Granular cell | 0(0.00%) | 1(12.5%) | 1(3.3%) |
| Basal cell | 0(0.00%) | 0(0.0%) | 0(0.0%) |
| Unicystic |
| Luminal | 0(0.00%) | 2(25.0%) | 2(6.7%) |
| Mural | 3(13.6%) | 1(12.5%) | 4(13.3%) |
| Intraluminal | 0(0.00%) | 0(0.00%) | 0(0.0%) |
| Desmoplastic | 3(13.6%) | 0(0.00%) | 3(10.0%) |
| Peripheral | 0(0.00%) | 0(0.00%) | 0(0.0%) |
The predominant anatomical distribution of ameloblastoma was in the mandible (86.7%), while the maxilla was affected in 13.3% of the cases. The trend was not different in both Thai and Burmese population in term of jaws distribution (χ2 test, p=0.20). In both jaws, posterior region was the most affected site (χ2 test, p= 0.04). Prevalence of posterior region occurrences was 6.7% and 63.3% for maxilla and mandible respectively. Most frequently involved anatomical site among the four quadrants was right posterior body-ramus-angle region (n=10, 33.3%) followed by the same anatomical location on the left side of mandible (n=9, 30.0%). However, complete involvement of one side (left or right) of maxilla or mandible was observed in three cases (10%). Whole jaw involvement was also seen in total of five cases (16.7%) and all of the cases occurred in mandible (n=2, 9.1% in Thai, n=3, 37.5% in Burmese). Involvement of condylar head and/or coronoid process was found in six cases. (n=5, 22.7% in Thai, n=1, 11.1% in Burmese) [Table/Fig-2].
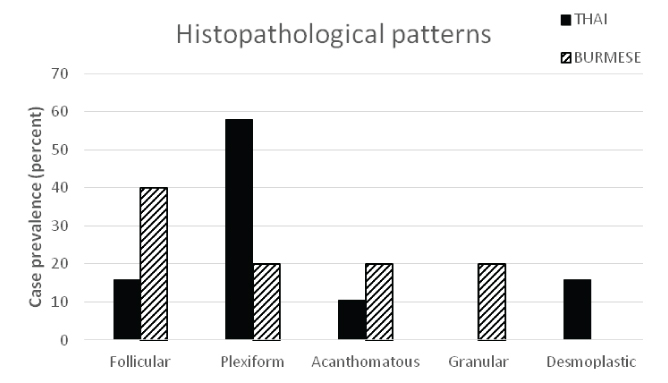
Almost all cases were pain-free (n=29, 96.7%) and most common clinical manifestation was swelling of affected region (n=27, 90.0%). Other less frequent clinical appearances included root displacement, root resorption and bone perforation were observed in seven cases (n=2, 6.7% for root displacement, n=2, 6.7% for bone perforation, and n=3, 10.0% for root resorption). Pain and paresthesia was reported in one case (n=1, 3.3%). Radiographically, multilocular appearance was observed in 70.0% of cases, whereas 30.0% were unilocular. There was no statistical differences between nationalities for radiographic appearances (χ2 test, p=0.148). Embedded tooth associated with the tumour was observed in seven cases (23.3%): four unilocular and three multilocular ameloblastomas. Three subtypes of ameloblastomas were diagnosed: unicystic ameloblastoma (n=6, 20%), conventional solid/multicystic ameloblastoma (n=21, 70.0%), and desmoplastic ameloblastoma (n=3,10%) [Table/Fig-2,3]. In unicystic ameloblastoma, most cases were histologically classified as mural (66.7%) while the luminal type was observed in 33.3% of cases. The most common histologic pattern encountered in the conventional solid/multicystic ameloblastoma was the plexiform type (57.2%) followed by follicular type (23.8%) and acanthomatous type (14.3%). The least common pattern was granular cell type (4.7%). There was no statistical differences in histopathologic subtypes between nationalities (χ2 test, p=0.064) [Table/Fig-4]. In majority of cases total surgical excision of tumours was provided for solid multicystic ameloblastoma whereas, enucleation was done for the cases of unicystic ameloblastoma.
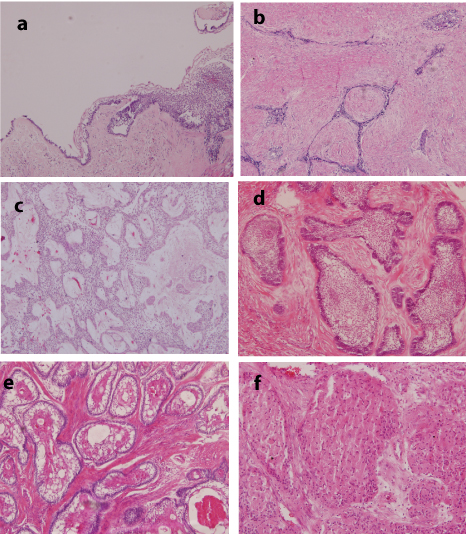
Histological features of biopsy specimens from Southeast Myanmar and lower Northern Thailand populations showing various types of ameloblastoma in this region; a) Unicystic ameloblastoma (H&E stain, 10X); b) Desmoplastic ameloblastoma (H&E, 4X); c) Plexiform type ameloblastoma (H&E, 10X); d) Follicular type ameloblastoma (H&E, 10X); e) Acanthomatous type ameloblastoma (H&E, 10X); f) Granular cell type ameloblastoma (H&E, 40X).
Distribution of ameloblastoma according to histopathologic subtypes in Thai and Burmese population.
Discussion
In most parts of the world, ameloblastoma is ranked number two in odontogenic tumours [5], but this is not true in Thailand and may not also be applicable in Southeast Asian countries. According to Worawongvasu R and Dhanuthai K et al., ameloblastoma was the most common odontogenic tumour in Thailand [22,23]. However, there are not many publications in English literature that report information solely for ameloblastoma in Thailand, despite of its high incidence. The only study dedicated for analysis of ameloblastoma in Thailand was published by Sirichitra V et al., which discussed only intraosseous ameloblastoma of the jaws [24]. Similarly, studies from other Southeast Asian countries discussed ameloblastoma only briefly while evaluating other odontogenic tumours rather than a separate work of its own entity. Furthermore, in a recently formed country like Myanmar, information about ameloblastoma is not much exposed and needs to be explored. This present study is among one of the first to report ameloblastoma profile from border of Southeast Myanmar and lower Northern Thailand regions to provide precise information of ameloblastoma in populations residing in this geographic area.
The prevalence of ameloblastomas in these local region is 5% which considered high when compare with countries in North America (0.21%) but in line with other Asian countries (4.46%) [25]. In Southeast Asia, a prevalence of 9.96% was reported from one institution in Vietnam. Incidence of 27.6%, 35.0% and 51.3% among odontogenic tumours was reported from one institution in Malaysia and other two institutions in Thailand respectively [22,23,25,26]. However, relative incidence of ameloblastoma may not reflect real occurrences because studies from this region are generally carried out at academic centers and most cases were acquired from biopsy recorded in dental school where ameloblastoma were diagnosed more frequently than other odontogenic tumours that can be caught from radiograph in the clinic.
There is generally no gender preference for ameloblastoma [25], however in Thai population it showed slightly male predilection (M:F; 1.4:1). Even though this is not relevant with the M:F ratio of 1:1.1 reported by Dhanuthai K [23] but the inference from present study is in line with 1.3:1 ratio observed by Worawongvasu R and Tiensuwan M in their study of odontogenic tumours in Thailand [22]. Greater occurrence in men was also documented in one study from Malaysia showing exactly the same M:F ratio of 1.4:1 [26]. Male to female ratio in Burmese population shows slightly female predominance with ratio of 1:1.6. These gender variations of ameloblastoma in this region comply with aberrant sex distribution as in many countries in different locations of the world such as in India and Nigeria the predilection of ameloblastoma was reported in males [16,27], but in Brazil the prevalence was comparable between males and females [28].
Although wide age range was affected, ameloblastoma occurred more often in the second, third and fourth decades of life in this present study. The peak prevalence in second decade (27.3%) indicates high frequency of ameloblastoma in young patients in Thai population whereas, peak prevalence for Burmese was 10-years older. This finding in Thais is in contrast with relatively low (10%-15%) occurrences of ameloblastoma in young patients (< 19 years) reported by Kim SG JH in Korea [12] but goes along with the study of Pereira FAC ML in Brazil [28] which reported 25% prevalence of ameloblastoma affected young patient. Furthermore, similar findings from other studies also reported higher prevalence in younger age [16,28] whereas other Thai studies reported third decade to be the peak prevalence of ameloblastoma [22,23].
For both Thais and Burmese, ameloblastomas involved mandible more frequently, where the posterior body-ramus-angle region of right and left mandible were the two most commonly affected sites respectively. Statistically significant difference was observed (χ2 test, p=0.04) in terms of posterior or anterior anatomic sites distribution which is well recognized in the literature [7,9–12,15,16,21,22,25,28]. However, entire involvement of one side or whole jaw involvement is not infrequent. In this study, severe involvement of the whole jaw was found only in mandible of the patients from both countries. Even condylar head and/or coronoid process were also involved by ameloblastoma and lesions with wide extent were found more in Burmese population. Delayed diagnosis of such extensive ameloblastoma may be because of socioeconomic status of patient living along the border of Thai-Myanmar territory as well as commutation difficulty in that area.
Asymptomatic slow growth of affected area is a consensus in the literature for the manifestation of ameloblastoma which is consistent with the results of the present study [7,11,12,22,25,28]. Besides, less frequent symptoms such as pain, paresthesia, root displacement, root resorption and bone perforation were also present. Embedded tooth associated with the lesion was also present in this study. Radiographic appearance for both Thais and Burmese demonstrated the predominance of multilocular radiolucency which is the most common radiographic appearance of ameloblastoma. In a study conducted in Thailand by Worawongvasu R and Tiensuwan N [22], the authors observed that almost 41.1% of the cases corresponded to multilocular lesions. However, in a multicentric study of ameloblastoma by Dhanuthai K et al., the number of multilocular cases was comparable to that of the unilocular radiolucency [25].
In the present study, conventional solid/multicystic ameloblastoma were predominant histological subtypes in both Thai and Myanmar populations which is in accordance with previous reports from Brazil [3], Tanzania [18], Estonia [21], Malaysia [26], Korea, Vietnam, Thailand, Canada and the United States [25]. Plexiform ameloblastoma was the most common histological pattern for Thais but not for Burmese in this present study. This histological subtype was also found more frequently in the study from Malaysia [26] but is not in line with other reports from Thailand and Brazil, in which follicular pattern revealed a greater frequency over the plexiform pattern [25,28]. This highlights the difference in trends of histologic patterns in Thai population living in different geographic area and also shows a younger age of diagnosis of ameloblastoma in this area. Unicystic ameloblastoma was equally found in both Thais and Burmese. Rare type of ameloblastoma such as basal cell ameloblastoma was not found. However, one case of granular cell ameloblastoma was presented in Burmese. Peripheral and desmoplastic ameloblastomas are also considered rare. However, desmoplastic subtype was documented in three Thai patients in this study.
Surgical removal is the main stay cost-effective treatment for ameloblastoma [29]. To avoid recurrence, radical surgery with safe margin is the best primary method for treating solid/multicystic ameloblastomas. However, to prevent extensive deformity of orofacial structure for patient with first decade diagnosis, conservative method may be considered in case of non-soft tissue involvement unicystic ameloblastoma located at anterior mandible only [30].
Limitation
Unfortunately, in this study postoperative and follow up records could not be accessed for all patients due to retrospective nature of study. Other limitation is that information in regards to biopsy specimens and demographic data were collected and analyzed in only one institute. Collaboration with neighboring hospitals as well as hospitals in Myanmar employing multicentric study would enhance our knowledge of ameloblastoma in the future.
Conclusion
Prevalence of ameloblastoma in Southeast Myanmar and lower Northern Thailand populations corresponds with data from other geographic areas of Thailand and other Asian countries. However, some demographic and histopathological profiles are different, with more occurrences observed in young patient and plexiform type being the most common histologic subtype in this study.