A Report of Successful Procedural, Clinical, and Angiographic Outcomes with a Tapered Stent of a Patient in Naturally Tapered Coronary Vessel
Rajendra Kumar Premchand1, Yerra Shiv Kumar2
1 Director and Consultant Interventional Cardiologist, Department of Cardiology, Krishna Institute of Medical Sciences Ltd, Secunderabad, Telangana, India.
2 Consultant Interventional Cardiologist, Department of Cardiology, Mahaveer Hospital, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Rajendra Kumar Premchand, Director and Consultant Interventional Cardiologist, Department of Cardiology, Krishna Institute of Medical Sciences Ltd, Secunderabad-500003, Telangana, India.
E-mail: kumarpre@hotmail.com
In cases involving stenosis or occlusions in major parts of a long vessel, natural tapering of coronary vessels may create dilemma in deciding the optimal stent size during percutaneous coronary intervention. In this regard, tapered stents have been developed recently. Herein, we present a case of 67-year-old male patient with triple vessel disease including two tandem lesions in naturally tapered Left Anterior Descending (LAD) artery. The patient received a 3.0–2.5x60 mm Sirolimus-eluting BioMime Morph stent (Meril life Sciences, Gujarat, India) in the mid-distal LAD lesion along with conventional stent implantations in other two lesions. The procedure was successful and good coronary flow was obtained after revascularization. The patient remained asymptomatic thereafter. At one year, angiographic follow-up revealed good flow and no restenosis in the LAD vessel. We are of opinion that using tapered stents with decremented diameter may offer the advantages of excellent adaptation to vessel size, vessel tapering, and good apposition in patients with long coronary lesions in tapered vessels.
BioMime Morph, Long lesion, Percutaneous coronary intervention
Case Report
A 67-year-old male patient presented with the symptoms of class II-III angina (as per Canadian Cardiovascular Society Grading System), i.e., chest heaviness and shortness of breath on exertion for six months. Two weeks prior to the presentation, his tread-mill test was tested positive, elsewhere. He was admitted to our hospital for further management. He was a known case of chronic rheumatic heart disease with mild mitral stenosis and was suffering from diabetes for past 15 years.
At the time of presentation, his blood pressure was 140/80 mmHg and the pulse rate was 94 beats/min. Physical examination of the patient revealed clear chest and mild diastolic murmur. All haematological and biochemical tests were within normal ranges. Electrocardiogram revealed normal sinus rhythm. Other laboratory examinations were within normal ranges. Subsequently, coronary angiography was performed through transradial approach using 5F Tiger catheter. It revealed two tandem lesions in Left Anterior Descending (LAD) artery, 90% lesion in mid LAD and 95% lesion after third diagonal (D) branch, with ostio-proximal tight lesions in D2 and D3 [Table/Fig-1a]. Further, there was 90% stenosis in mid Left Circumflex (LCX) artery and 90% stenosis in distal Right Coronary Artery (RCA), with mild irregularities in Posterior Descending Artery (PDA) and Posterior Left Ventricular Branch (PLVB). The patient was diagnosed with triple-vessel disease. Patient was advised for Coronary Artery Bypass Grafting (CABG) with mitral valve reconstruction or triple vessel stenting with medical management for mitral stenosis. Treatment options were discussed with the family. The patient and his family opted for triple vessel stenting.
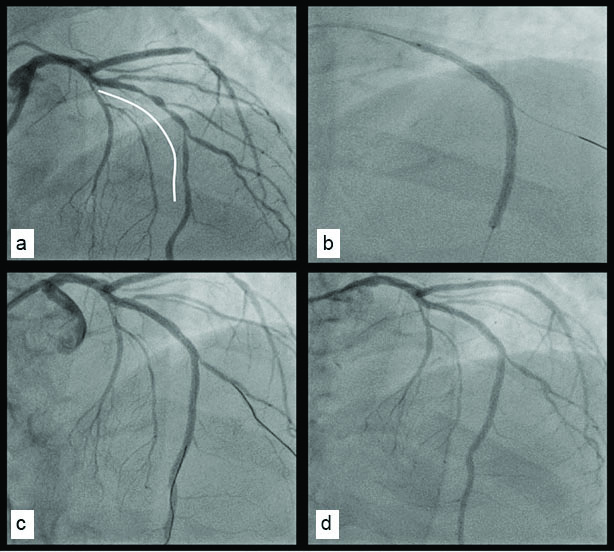
a) Coronary Angiography image of the left anterior descending coronary artery proximal mild and mid two tandem lesion with D2 and D3 ostio-proximal tight lesion; b) Treated with 3.0-2.5 x 60 mm BioMime Morph sirolimus eluting tapered stent (Meril life Sciences, Gujarat, India); c) Angiogram of the left anterior descending coronary artery after revascularization; d) Angiographic follow-up at twelve months show no restenosis
Subsequently, the patient underwent Percutaneous Coronary Intervention (PCI) using 6F EBU 2.5 and 6F JR 3.5 guiding catheters. Considering the tapered nature of the LAD vessel, the patient received a 3.0–2.5x60 mm Sirolimus-eluting BioMime Morph stent (Meril life Sciences, Gujarat, India) in the mid-distal LAD lesion [Table/Fig-1b] after a predilatation with 2.0x10 mm balloon. Subsequently, the ostail and proximal parts of stent dilatations were performed with 3.0x12 mm NC balloon, while mid and distal parts of stent dilatations were performed with 2.5x12 mm NC balloon. A good coronary flow was achieved in the LAD lesion after revascularization [Table/Fig-1c]. Additionally, the patient received a 2.5x24 mm Sirolimus-eluting BioMime stent (Meril life Sciences, Gujarat, India) in the mid LCX lesion and a 2.5x16 mm Sirolimus-eluting BioMime stent (Meril life Sciences, Gujarat, India) in the distal RCA lesion. Overall, the procedure was successful. Post operatively, the patient was managed with antianginal drugs, dual antiplatelets, and statins. He was discharged after satisfactory examinations. He was stable at the time of discharge. Thereafter, the patient was followed-up regularly. The patient remained asymptomatic after the index procedure. At one year angiographic follow up, the patient displayed patent BioMime Morph stent (Meril life Sciences, Gujarat, India) in the LAD vessel with no in-stent restenosis [Table/Fig-1d].
Discussion
Rheumatic heart disease is a highly prevalent disease in developing countries like India. Further, the incidence of coronary artery disease is also on the rise. Hence, the manifestation of comorbid rheumatic heart disease and coronary artery disease becomes more likely [1]. A recent Indian study has estimated the overall prevalence of coronary artery disease is about 11% in patients with rheumatic heart disease (12% in men, 8% in women). Further, the age and male gender are found to influence the occurrence of coronary artery disease in these patients [2]. In literature, published case reports on simultaneous management of rheumatic heart disease along with coronary artery disease are very rare [1]. In this regard, the present case is valuable as the patient was treated successfully with medical management for rheumatic heart disease and PCI with stent implantation for coronary artery disease. Of significance, the patient described her had triple vessel disease along with tandem lesions, which required particular attention.
In general, PCI with stent implantation is the most widely used management option for patients with coronary artery disease, including those with comorbid rheumatic heart disease [1,3]. However, complications such as restenosis can result in the ultimate failure of the procedure. Stent size mismatch has been identified as an important factor, which may lead to restenosis in some patient [4]. This is a particular concern for cases in which coronary vessel diameter changes to a significant degree over the length of a stent. In practice, such cases are commonly encountered due to tapering of coronary vessels. In such cases, clinicians have to decide the stent sizing carefully as a large diameter mismatch may lead to excessive damage in the vessel wall and may increase the risk for clinical failure [3]. Since conventional stents may not be able to adapt effectively in tapered vessels, appropriate stent sizing becomes challenging [5]. In this regard, tapered stents have been developed recently to minimize clinical failure and maximize the clinical benefits in such patients. Herein, we report a case of successful tapered stent implantation in an elderly male with triple vessel disease. The one year angiographic follow up indicated no restenosis in the tapered stent. To the best of our knowledge, this is first such case report demonstrating the one year clinical and angiographic outcomes with a tapered coronary artery stent in an Indian patient. We consider that, using a tapered stent has advantages of excellent adaptation to vessel tapering and good apposition.
Tapering is defined as the ratio of the area change to the vessel length [6]. Earlier, Zhang LR et al., have determined the coronary anatomy of 526 adult subjects from Asia. They identified that the average diameter of LAD was 3.92 mm at origin and 2.10 mm at distal end, with a decremented ratio of 7.7%; the average diameter of LCX was 3.57 mm at origin and 2.10 mm at distal end, with a decremented ratio of 9.7%; and average diameter of RCA was 3.97 mm at origin and 2.15 mm at the distal end, with a decremented ratio of 5.1% [7]. In another study, Banka VS et al., determined the degree of taper between 1 cm proximal and distal to the stenosis. They found that 23% arteries showed ≥1 cm taper, 19% arteries showed 0.5–0.99 mm taper, and 8% arteries showed reverse taper [8]. These findings indicate that the dimensions naturally taper along the length of coronary arteries [7,8]. In cases involving stenosis or occlusions in major parts of a long vessel, natural tapering may create dilemma for optimal balloon sizing and optimal stent sizing during PCI [3].
Some clinicians may prefer to deploy multiple overlapping stents against one long stent. However, the available literature suggests that stent overlapping is associated with delayed healing and increased inflammation at the site of deployment. Further, it has been demonstrated that overlapping stents is associated with impaired angiographic and long-term clinical outcome, including death or myocardial infarction [9]. Considering this, we opted for using one long tapered stent in our patient. The procedural as well as one year clinical and angiographic follow-up outcomes in our patient were satisfactory.
Conclusion
In conclusion, we opine that tapered stents may provide optimal outcomes in tapered arterial segments with few complications and may offer a new approach to overlapping stents. We believe that using stents with decremental diameter may offer the advantages of excellent adaptation to vessel size, vessel tapering, and good apposition in patients with long coronary lesions in tapered vessels.
[1]. Harikrishnan S, Bhat A, Tharakan J, Percutaneous balloon mitral valvotomy and coronary stenting in the same sittingHeart Vessels 2003 18(3):150-52. [Google Scholar]
[2]. Narang R, Chadha DS, Goel K, Mishra S, Bajaj N, Sharma S, Screening coronary angiography prior to surgery in rheumatic valvular heart disease: A study of 2,188 patientsJ Heart Valve Dis 2009 18(4):455-60. [Google Scholar]
[3]. Timmins LH, Meyer CA, Moreno MR, Moore JE Jr, Mechanical modeling of stents deployed in tapered arteriesAnn Biomed Eng 2008 36(12):2042-50. [Google Scholar]
[4]. Chan R, Lim R, Does Stent Size “Mismatch” Predispose to Restenosis?Heart Lung Circ 2010 19:S128 [Google Scholar]
[5]. Van Geuns RJ, Awad K, IJsselmuiden A, Koch K, The role of self-expanding stents in patients with atypical coronary anatomyInterventional Cardiology Review 2014 9(1):11-16. [Google Scholar]
[6]. Roach MR, MacLean NF, The importance of taper proximal and distal to Y-bifurcations in arteriesFront Med Biol Eng 1993 5(2):127-33. [Google Scholar]
[7]. Zhang LR, Xu DS, Liu XC, Wu XS, Ying YN, Dong Z, Coronary artery lumen diameter and bifurcation angle derived from CT coronary angiographic image in healthy people [Article in Chinese]Zhonghua Xin Xue Guan Bing Za Zhi 2011 39(12):1117-23. [Google Scholar]
[8]. Banka VS, Baker HA 3rd, Vemuri DN, Voci G, Maniet AR, Effectiveness of decremental diameter balloon catheters (tapered balloon)Am J Cardiol 1992 69(3):188-93. [Google Scholar]
[9]. Räber L, Jüni P, Löffel L, Wandel S, Cook S, Wenaweser P, Impact of stent overlap on angiographic and long-term clinical outcome in patients undergoing drug-eluting stent implantationJ Am Coll Cardiol 2010 55(12):1178-88. [Google Scholar]