Knee X-Ray in Short Stature: Helpful Indicator to Diagnose SHOX Deficiency
Partha Pratim Chakraborty1, Rana Bhattacharjee2, Subhankar Chowdhury3
1 Assistant Professor, Department of Medicine, Midnapore Medical College and Hospital, Midnapore, West Bengal, India.
2 RMO-cum-Clinical tutor, Department of Endocrinology and Metabolism, IPGME&R/SSKM Hospital, Kolkata, West Bengal, India.
3 Professor and Head, Department of Endocrinology and Metabolism, IPGME&R/SSKM Hospital, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Partha Pratim Chakraborty, House No: BE:64 Bidhan Nagar (East) P.O: Midnapore Pin: 721101, Midnapore, West Bengal, India.
E-mail: docparthapc@yahoo.co.in
Leri-Weill dyschondrosteosis, SHOX gene, Turner’s syndrome
Case 1
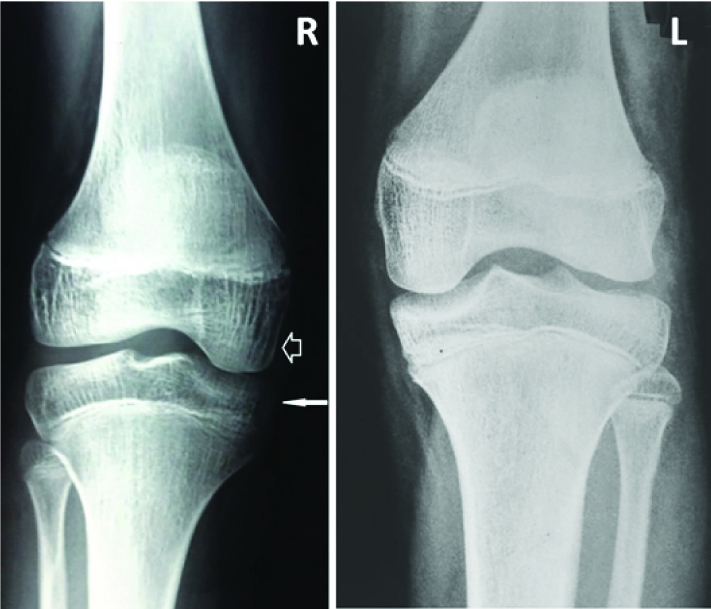
A 15-year-old girl, born of a non-consanguineous union presented with primary amenorrhea and short stature. Axillary and pubic hairs were absent and she did not have breast budding. There were some stigmata of Turner’s Syndrome (TS) like low set ears, low posterior hairline and cubitus valgus. There were no obvious knee deformities. Her karyotype was 45 XO. X-ray of her knees [Table/Fig-1] revealed bilateral and symmetrical enlargement of medial condyles of tibia (thin and solid arrow) and the medial femoral condyle extended downward (thick and hollow arrow) more than the lateral one.
X-ray knee of patient of Turner’s syndrome (Case1) showing bilateral and symmetrical enlargement of medial condyles of tibia (thin and solid arrow). The medial femoral condyle is extended downward (thick and hollow arrow) than the lateral one.
Case 2
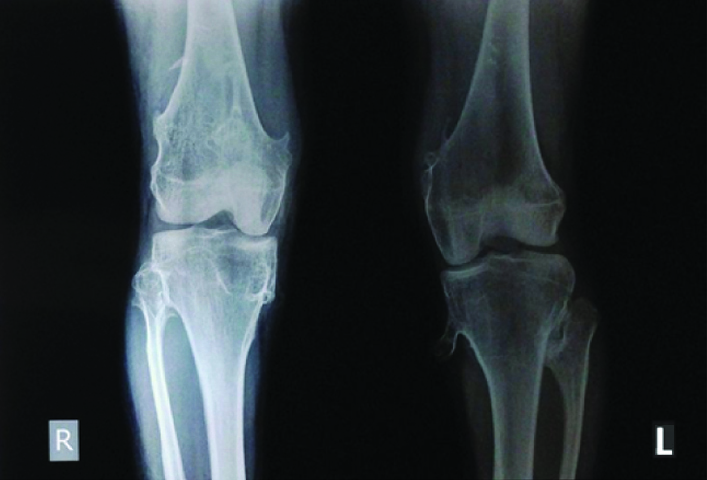
A 14-year-old girl with menarche at the age of 12 year presented with severe short stature and bilateral cubitus valgus. Her breasts and pubic hairs were of Tanner stage 5 and she had cyclic predictable menses. Her karyotype was 46, XX and genetic study documented mutation in one of the Short Stature Homeobox (SHOX) gene confirming Léri -Weill Dyschondrosteosis (LWD). Knee X-ray revealed [Table/Fig-2] downwards displacement of femoral medial condyles compared to lateral condyles bilaterally along with multiple small exostoses projecting from distal femoral and proximal tibial condyles.
X-ray knee of patient of Léri -Weill dyschondrosteosis (Case 2) showing downwards displacement of femoral medial condyles compared to lateral condyles bilaterally along with multiple small exostoses projecting from distal femoral and proximal tibial condyles.
SHOX gene with a cytogenetic location in X(p22.33) and Y(p11.3) plays an important role in chondrogenesis at the growth plates and subsequent long-bone growth. The predominant cause of short stature in TS is SHOX haplo-insufficiency while LWD is the outcome of deletion of the entire SHOX gene or other genetic changes that normally help regulate the SHOX gene’s activity.
There is paucity of data on radiological abnormalities of knees in patients with SHOX abnormalities. Most of the studies involved patients of TS only and knee abnormalities have been reported in up to 60% of such patients [1]. Medial femoral condyles were larger and extend down wards than the lateral ones and the tibial epiphyseal plates were found to be angled obliquely, medially and downward to accommodate the larger medial femoral condyles. These changes were bilateral and symmetric and in some instances a beaklike exostosis was found projecting from medial tibial condyle [2]. In one such study knee abnormality was unique to TS and was present in 2/3 of TS patients aged between 8-42 years. In all of them clinical examination of the knees was otherwise normal [3].
There are suggestions for baseline routine radiological survey prior to SHOX screening in all patients affected with short stature [4], in whom no obvious explanation of short stature have been found. Routine knee X-ray in suspected or proven SHOX related disorders will also help us to properly estimate the frequency of such abnormality in this group of patients.
To conclude, these radiological changes with medial femoral condyle extending downward more than the lateral one, and its contour being more rounded than that of the flattened lateral condyle are highly specific for SHOX haplo-insufficiency and they are worth looking for in appropriate patients, as they may serve as helpful clues for diagnosing such disorders with less obvious clinical features.
[1]. Committee on GeneticsHealth supervision for children with Turner syndrome. American Academy of PediatricsPediatrics 1995 96(6):1166-73. [Google Scholar]
[2]. Levin B, Gonadal dysgenesis. Clinical and roentgenologic manifestationsAm J Roentgenol Radium Ther Nucl Med 1962 Jun 87:1116-27. [Google Scholar]
[3]. Kosowicz J, Changes in the medial tibial condyle: a common finding in Turner’s syndromeActa Endocrinol (Copenh) 1959 31(3):321-23. [Google Scholar]
[4]. Heath KE, Radiological signs of Léri-Weill dyschondrosteosis present in the A170P carrierJ Clin Pathol 2012 65(10):962 [Google Scholar]